


CASE REPORT
A 34-year-old woman was diagnosed when she was two as having asthma. She has been treated since then with salbutamol but has shown no improvement. The patient suffers from persistent disnea which gets worse with exercise. She also has a slow digestive system. In the physical examination we find a persistent shrill (shrill? probablemente "wheeze") during expiration.
Skin-prick test to house dust mites (D. pteronyssinus, D. farinae), molds, animal dander and most common pollens were performed. Total and specific IgE to HDM and molds by CAP method were measured. A spirometry with DLCO, a chest X-ray, and a fibroscopic exploration from nose to larynx were also done.
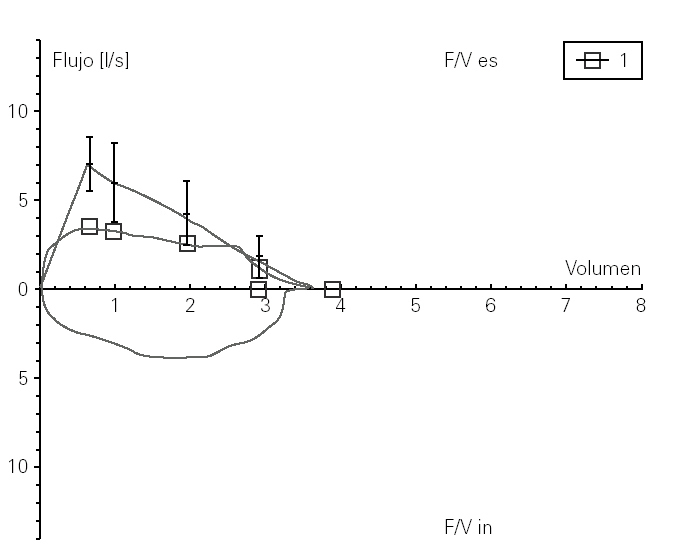
The skin-prick tests were all negative; total IgE was 43.50 U/ml with negative specific IgE to house dust mites and molds. The functional lung test (fig. 1) showed an altered PEF (3.37) 48.5 % of that normally predicted with FEV1, FVC and DLCO. The thorax X-ray showed a mild trachea displacement and the fibroscopic exam was normal.
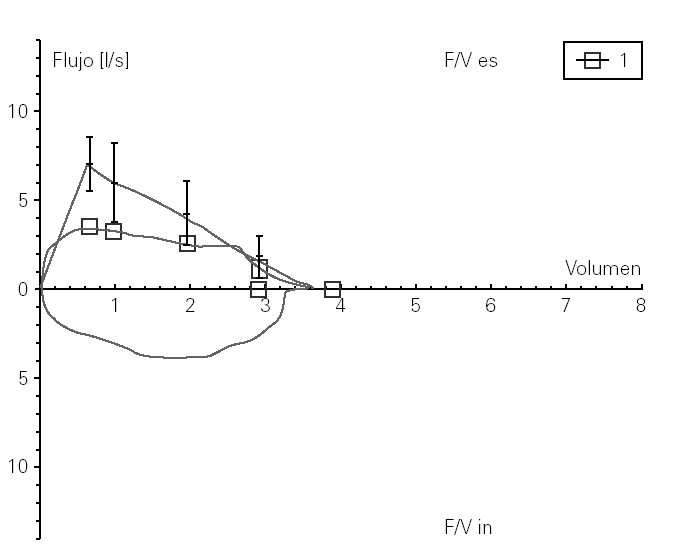
Figure 1.--Functional lung test showing an altered PEF.
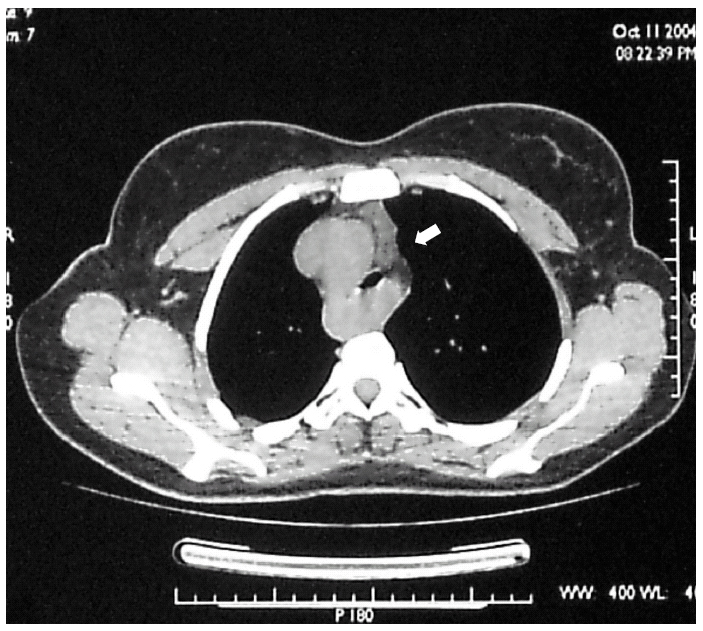
In view of the results we ordered a thorax CT-scan which showed a right aortic arch and an abnormal subclavia situation that compressed trachea and esofagus (fig. 2). This result was confirmed with a cateterisism.
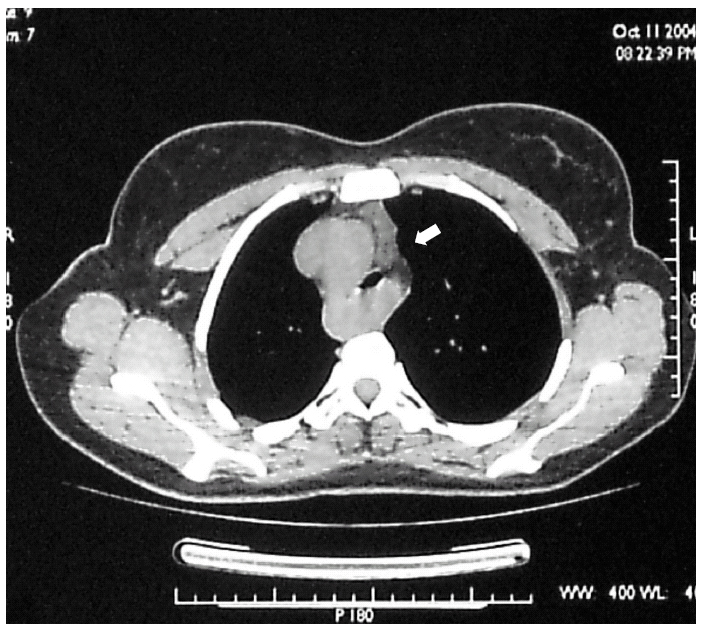
Figure 2.--Thorax CT-scan.
The patient is having a vascular surgical procedure in order to re-locate the subclavia in the correct anatomical position.
COMMENTARIES
Asthma is probably the most common disease in children that causes persistent disnea, but there are a lot of anatomical abnormalities that can be detected with a thorax x-ray and functional lung test. Trachea extrinsic compressions can have different causes 1, and right sided aortic arch is one of them. Occasionally this anatomic abnormality does not cause symptoms 2, but most of the time it does 2 and sometimes is misdiagnosed and the patient is treated as having asthma 3. The diagnosis is often made in childhood because symptoms usually start then.
A CT-scan is recommended in these patients, and a magnetic resonance or an angiography can also help the diagnosis 4. Surgical treatment is the most common course of action 5,6, but when the extrinsic compression is not caused by a vascular structure a self-expanding stent can be used 1.
We have to consider anatomical malformations and other diseases such as cystic fibrosis and gastro-esophageal reflux before making the diagnosis. If the diagnosis is not correct, the treatment will not improve the patient's life.
Furthermore, this case also reminds us of the importance of radiology and the functional lung test in the study of respiratory diseases. Before diagnosing a patient as having asthma we must rule out other diseases with these tests.
Declarations
The authors disclose that this manuscript is absent from any source of funding or interest in the subject matter with pharmaceutical manufacturers.
This manuscript is original, is not under consideration by another journal and has not been previously published.
Transfer of Copyright statement
The authors assign to Allergología et Immunopathologia the copyright in this manuscript in all forms and media, throughout the world, in all languages, for the full term of copyright and all extensions and renewals thereof, effective when and if the manuscript is accepted for publication.
