





Date palm pollen allergy is frequently associated with polysensitisation. Observational studies have suggested that date-palm-sensitised individuals could be included in a distinct group of polysensitised patients. The objectives of the study were to analyse the clinical characteristics of a group of patients diagnosed of date-palm pollen allergy and to compare them with pollen allergic patients without date-palm sensitisation.
MethodsForty-eight palm-pollen sensitised individuals were classified as Group A. A control group of 48 patients sensitised to pollens but without palm-pollen allergy were included as Group B. All individuals were skin prick tested with a common battery of aeroallergens. Information about age, sex, family history of atopy, respiratory symptoms, food allergy and sensitisation to other pollens were considered variables of the study. Specific IgE and the allergogram to date-palm pollen were determined in a subgroup of Group A.
ResultsSignificant differences in the family history of atopy and number of sensitisations were observed. Both parameters were significantly higher in Group A. Group A showed high prevalence of asthma and higher level of sensitisation to foods (p<0.05). Significant differences were obtained for sensitisation to epithelia and pollens. Pho d 2 was the most commonly recognised allergen (83.3%) in the palm-pollen allergic group.
ConclusionsDate-palm pollen allergic patients constitute a homogeneous group characterised for showing bronchial asthma, sensitisation to food allergens and polysensitisation. These results suggest that the reasons for sensitisation to date-palm pollen remain to be elucidated, but could relate to the existence of as yet non-identified pan-allergens.
Allergy to pollen of different species of the botanical family of Palmaceae has been widely documented worldwide1–4 but has not been extensively investigated, especially in relation to symptoms, severity, epidemiology, polysensitisation or cross-reactivity with other pollens. The family Palmaceae includes more than 200 genus and 2600 species, characterised by a tall columnar trunk bearing large leaves grouped in apical tufts and an inflorescence clustered in bunches.5 These plants, especially palm trees, are abundant in tropical and subtropical regions where rainfall is not abundant. The genus Phoenix is one of the best known genera in the Mediterranean latitudes and two species, P. dactylifera and P. canariensis, are the most representative members. Other autochthonous genera have been described in America and Australia but until now allergic sensitisation to these has not been related.
Previous published papers have demonstrated that palm pollen grains from different genus induce respiratory symptoms in allergic sensitised patients.6,7 Kwaasi et al. described six major allergens of date palm pollen, with molecular weights between 12 and 65-67 kDa; four of them were recognised by 80-93% of patients’ sera (12, 14.4, 57 and 65-67 kDa).8 Recently, two new proteins (20 and 90 kDa), with capacity to bind IgE,have been described.9 An allergen of about 14 kDa, named as Pho d 2, has been identified as a profilin,10 a pan-allergen present in all eukaryotic cells and considered one of the allergens most often involved in cross-reactivity between different pollens and between pollens and plant-derived foods.11
In Spain, date palm pollen sensitisation is common on the Mediterranean Coast, where the presence of this tree is abundant. In Elche, Alicante, where the biggest date palm tree area is situated, prevalence of sensitisation to this pollen is 5.6%,12 while in Zaragoza, a non-Mediterranean area, where this tree is scarce, sensitisation to this pollen is about 29.4% in polysensitised individuals.13 In other Mediterranean areas, near Elche, the prevalence of sensitisation is 14-18.9% in Cartagena,13,14 and 11.3% in some regions of Valencia.15 Despite these differences, all the Spanish studies conclude that sensitisation to date palm tree is generally associated to polysensitised individuals.12–16 These results suggest that, in the Spanish Mediterranean area, cutaneous sensitisation to this pollen could be related to the existence of a pan-allergen,15 probably a profilin,10 and that palm pollen-sensitised patients could be forming a distinct group of pollen-sensitised individuals.
The objectives of this study were to analyse the clinical characteristics of a group of previously diagnosed pollen allergic patients, with positive skin prick test (SPT) to date palm pollen and residing in the urban area of Cartagena, Spain and to compare their sensitisation profile with an also diagnosed pollen allergic patient group with negative SPT to date palm pollen and residing in the same area.
MethodsPatient populationIn the present retrospective study, a total of 96 individuals residing in the urban area of Cartagena, Murcia, Spain who attended to Allergy service (Hospital General Básico de la Defensa, Cartagena) between 2004 and 2006 were included. Patients residing in rural areas were excluded. All of them had been previously diagnosed as allergic to different pollens and all of them experienced respiratory symptoms (rhinoconjunctivitis and/or bronchial asthma) after pollen exposure. All individuals were administered SPT with a common battery of biologically standardised aeroallergens at 30 HEP/ml for pollens and 100 HEP/ml for mites, manufactured following internal procedures (Laboratorios Leti S.A. Tres Cantos, Madrid, Spain), following international recommendations16 including mites (Dermatophagoides pteronyssinus, Dermatophagoides farinae, Lepidoglyhus destructor and Tyrophagus pustrenscentiae), moulds (Alternaria tenuis), epithelia (dog and cat) and pollens (grass mix, Olea europaea, Plantago lanceolata, Platanus spp., Artemisia vulgaris, Salsola kali, Parietaria judaica, Chenopodium album, Cynodon dactylon, Cupressus arizonica and Phoenix dactylifera (Bial-Arístegui S.A. Bilbao, Spain). Patients referring symptoms with different foods were also given SPT with the responsible food allergen extracts.
Individuals were divided into two groups:
- Group A.
48 consecutive individuals (females 54.2%) who met the inclusion criterion and with positive SPT to date palm pollen. Serum samples from 16 individuals who attended a second revision during the period of study were collected in order to determine the specific IgE against date palm pollen, after giving their informed consent.
- Group B.
(Control group) 48 individuals (females 70.8%) who met the inclusion criterion and had negative SPT to date palm pollen. These patients correspond to those individuals who met the inclusion criteria and attended to our Allergy Service in the same period as the patients included in Group A.
Age, sex, family history of atopy, respiratory symptoms (rhinitis, conjunctivitis and bronchial asthma), food sensitisation after contact or ingestion, sensitisation with pollens and other aeroallergens and cosensitisation with Parietaria judaica and grasses (cross-reactivity between both pollens has been suggested5,8), Salsola kali and Plantago lancelolata, (a positive association between these two pollens and date palm pollen has been documented)17 and olive (included in the study as it is an important allergen in Mediterranean countries) were considered variables of the study. The study was retrospective, and the methodology was based on the review of the clinical history, thus ethical committee approval was not considered necessary.
Specific IgESpecific IgE levels to P. dactylifera was determined in 16 patients from Group A, by CAP system (Phadia, Upsala, Sweden) using solid phase commercially available immunoCAPs and following the manufacturer's instructions. Values were expressed in kUI/l.
AllergogramAn amount of 20μg of proteins/lane from date palm tree extract was separated by Sodium dodecyl sulphate-polyacrylamide gels electrophoresis and electrotransferred to P-immobilon membrane (PVDF) (Millipore, Bedford, Massachusetts, USA). The membranes were dried at room temperature for 4hours and incubated overnight with individual sera (1:2 dilution in phosphate-buffered saline Tween 0.1%). After washing, membranes were incubated with anti–human IgE-peroxidase (Ingenasa, Madrid, Spain), developed with luminol solutions (Immun-Star HRP Chemiluminescent Kit; BioRad Laboratories, Hercules, CA, USA) and detected using chemiluminescence (ChemiDoc XRS; BioRad Laboratories).
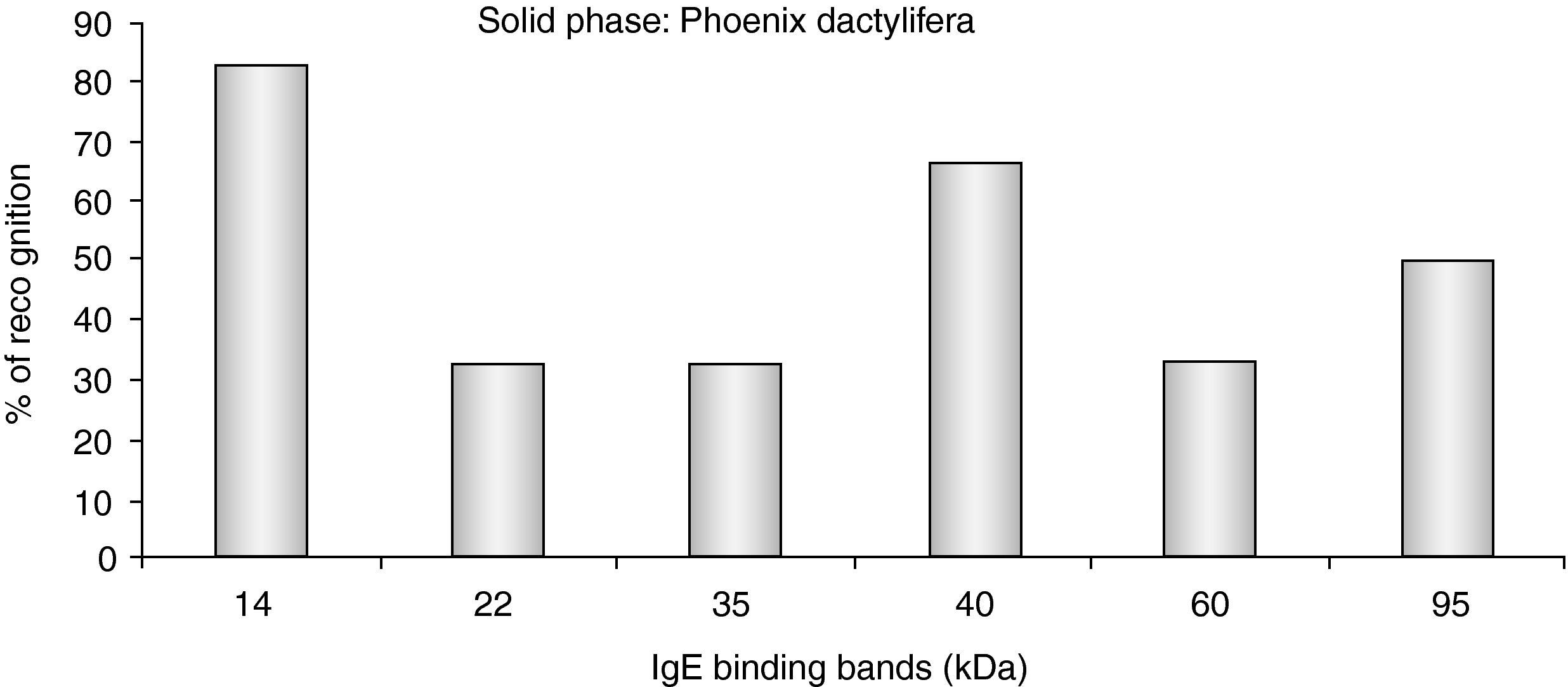
IgE binding bands in all individuals were visualised and analysed using Quantity One software (BioRad Laboratories) in order to determine the exact molecular weight respect to the standard. Bands at 14, 22, 35, 40, 60 and 95 kDa were selected and an allergogram, with the 16 serum samples, was prepared in order to determine the percentage of recognition of each band.
Statistical analysisDescriptive, parametric and non-parametric statistics were applied. Chi-square (Yates correction) was calculated for comparison between qualitative variables. Statistically significant differences were obtained when p values were ≤ 0.05. Software SPSS Inc. (Chicago, Il, USA) was used for the statistical analysis.
ResultsPatient populationNon-significant differences were observed in age or sex distribution between Groups A and B. Significant differences were observed in the family history of atopy and the number of sensitisations. Both parameters were significantly higher in Group A (Table 1). In symptoms, Group A showed high prevalence of asthma (p<0.05) and non-significant differences were observed when rhinoconjunctivitis was analysed. Group A showed higher frequency of sensitisation to foods (p<0.05) (Table 1).
Clinical characteristics of the patient population.
| Group A Date palm (+) | Group B Date palm (−) | P | |
| Age (Years) | 30.52±18.45 (range 4-67) | 27.0±16.86 (range 3-82) | N.S. |
| Sex distribution | M=26 (54.2%) F=22 (45.8%) | M=34 (78.8%) F=14 (29.2%) | N.S. |
| Family History of Atopy | N=30 (62.5%) | N=20 (41.7%) | 0.041 |
| Rhinoconjunctivitis | N=47 (97.9%) | N=46 (95.8%) | N.S. |
| Bronchial Asthma | N=35 (72.9%) | N=22 (45.8%) | 0.007 |
| Food Allergy | N=11 (22.9%) | N=2 (4.2%) | 0.02 |
| Average number of sensitisations to different pollens | 7.25 | 3.31 |
Thirteen individuals reported symptoms after food ingestion and showed positive SPT to these food extracts. Eleven of them (84.6%) where sensitised to date palm pollen (Group A). Nine (81.8%) had oral allergy syndrome after food ingestion and five (45.5%) referred symptoms after peach ingestion (Table 2).
Allergic patients sensitised to food allergens. Allergens involved and symptoms.
| Patient | Date palm pollen | Food allergens | Symptoms |
| 1 | + | Peach | OAS |
| 2 | _ | Nuts | Urticaria |
| 3 | + | Peas | OAS |
| 4 | + | Melon/Peach | OAS/Urticaria |
| 5 | _ | Peach | OAS |
| 6 | + | Melón/Banana | OAS/OAS |
| 7 | + | Melon/Peach | OAS/OAS |
| 8 | + | Tomato/Peach | OAS/OAS |
| 9 | + | Kiwi | Angio-oedema |
| 10 | + | Nuts | OAS |
| 11 | + | Peach | OAS |
| 12 | + | Peas | Urticaria |
| 13 | + | Peas/Nuts | OAS |
When sensitisation to different aeroallergens was compared, non-statistically significant differences were obtained in mites and moulds. Statistically significant differences were obtained with epithelia and pollens (P. judaica, S. kali, P. lanceolata, grasses, and olive) (Table 3).
Skin prick test to the aeroallergens included in the study.
| Group A Date palm (+) | Group B Date palm (−) | P | |
| Mites | N=26 (54.2%) | N=25 (52.1%) | N.S. |
| Moulds | N=6 (12.5%) | N=3 (6.3%) | N.S. |
| Epithelia | N=29 (60.4%) | N=13 (27.1%) | 0.002 |
| Grasses | N=40 (83.3%) | N=25 (52.1%) | 0.002 |
| Parietaria judaica | N=22 (45.8%) | N=7 (14.6%) | 0.002 |
| Salsola kali | N=39 (81.3%) | N=23 (47.9%) | 0.001 |
| Plantago lanceolata | N=47 (97.9%) | N=12 (25%) | 0.0001 |
| Olea europaea | N=47 (97.9%) | N=35 (72.9%) | 0.001 |
A total of nine individuals of the 16 tested from Group A (56.3%) showed positive specific IgE to P. dactylifera. The medium value was 0.96 KU/l (range 17.6-0.7 kU/l).
AllergogramOnly six of the 16 serum samples included in the study recognised individual bands in the immunoblot experiments. Five individuals (83.3%) recognised a band of 14 kDa (Pho d 2); two (33.3%) the 22 kDa band; two (33.3%) the 35 kDa band; four (66.7%) the 40 kDa band; two (33.3%) the 60 kDa band; and three (50%) the 95 kDa band (Figure 1).
Discussion
Date palm pollen pollinosis has not been widely analysed in European Mediterranean countries with the exception of some studies describing the prevalence of sensitisation in Southern Spain. In this area, it has been demonstrated that sensitisation to date palm pollen is highly prevalent among polysensitised individuals.12–16
Using a retrospective study with 96 individuals, all of them suffering from respiratory symptoms after pollen exposure, we have observed that patients sensitised to date palm pollen experience a high prevalence of bronchial asthma, are sensitised to a higher number of pollens and also refer more plant-derived food allergies. These results suggest that skin sensitisation to date palm pollen could be an indicator of severity of pollinosis in our area, probably because patients polysensitised to different allergens show higher risk of suffering bronchial asthma,18,19 although these findings could also be explained because patients were mainly sensitised to some allergens related to specific clinical manifestations such as bronchial asthma or food allergy.
With regard to the patient population, after analysing both groups, non-significant differences were observed in age or sex distribution in both groups. However, these differences between groups were statistically significant (p<0.01) when clinical symptoms and number of sensitisations to different pollens were evaluated.
Focussing our attention in our geographical area, and according to the observational results obtained in this revision, we can hypothesise that individuals sensitised to P. dactylifera show a different clinical profile of sensitisation, probably related with one or more specific pan-allergens, and not only profilin, as has been previously suggested.15 Supporting this theory, some topics can be highlighted: a) clinical symptoms showed for date palm pollen sensitised individuals, especially food allergy with oral allergy syndrome related with profilin sensitisation.20 b) A positive correlation has been described between birch and date palm tree sensitisation.15 Birch pollen grains contain high quantities of profilins; however their presence in semi-desertical areas is very rare; c) Prevalence of sensitisation to date palm pollen oscillates between 14% and 18.9% in pollen-allergic patients.13–15 These values are comparable with prevalence of sensitisation to profilins in central Europe, estimated to be around 20%.11
On the contrary, the allergenic profile of date palm pollen-sensitised individuals showed the presence of IgE binding bands corresponding to different allergens described in date palm tree8,9 and not only profilin (12-15 kDa)21 (Figure 1). Another point to consider is that in our geographical area, skin sensitisation to profilin is near 6%.23 Many patients sensitised to date palm pollen are SPT negative to profilin, although most profilin-sensitised individuals were sensitised to date palm pollen.22 Moreover, patients sensitised to date palm pollen showed major bronchial asthma, a typical symptom related with sensitisation to polcalcin.21 These results suggest that patients sensitised to date palm pollen could be sensitised not only to profilin but also to other allergens, not yet described in the extracts.
Another significant aspect in the study is that only nine patients of the 16 tested individuals with positive SPT to date palm pollen extract had positive specific IgE to date palm pollen. The cause should be analysed in detail but Phoenix extracts are not yet biologically standardised, the allergenic composition must be analysed in detail, CAP system and SPT use different date palm pollen extracts and finally, similar results have been published suggesting a different allergen composition of date palm cultivars.23
According to these observations, the clinical profile of patients and the association with other food and pollen sensitisation suggests that these patients could be sensitised to date palm pollen allergens or yet to be described pan-allergens such as polcalcins or carbohydrate determinants. These hypotheses could explain sensitisation to other studied pollens such as grasses, olive, P. judaica, P. lanceolata and S. kali, pollens belonging to different taxonomical families. These data corroborate cross-reactivity previously described with grasses8 or P. judaica5 or the correlation previously mentioned with P. lanceolata and S. kali.18
In conclusion, in the present preliminary observational and retrospective study we have observed that patients sensitised to date palm pollen constitute a subgroup of pollen-sensitised individuals, showing a particular clinical profile, probably because some allergens of the date palm tree are pan-allergens and are responsible for a common sensitisation. Further studies are needed in order to identify potential new pan-allergens and cross-reactivity in date palm pollen, a pollinosis not well understood and with high prevalence in some areas, where sensitisation reaches 10% of the population.13–16
Conflict of interestThe authors have no conflict of interest to declare.
