


Children born after in vitro fertilisation (IVF) are under greater risk of development of some health problems than those children born after spontaneous conception. Yet it is not exactly known what the prevalence of asthma and other allergic diseases among these children is.
Aims of the studyTo investigate the prevalence of asthma, allergic rhinitis and atopic dermatitis in children born after IVF, and controls born after spontaneous pregnancy using questionnaires of International Study of Asthma and Allergies in Children (ISAAC).
MethodsWe recruited 158 children (mean age: 4.60±2.14 years) born after IVF pregnancies and 102 children (mean age: 5.27±2.8 years) as control group to investigate the prevalences of asthma, atopic dermatitis and allergic rhinitis. The questions in the questionnaire were asked to the parents by telephone or face to face.
ResultsWheezing ever has been reported in 19 % of the children born after IVF and in 17.6 % of the control group (p>0.05). No significant differences were found between groups, in terms of use of any anti-asthma drugs, physician diagnosed asthma and admission to emergency room with wheezing (p>0.05). In addition, prevalence of allergic rhinitis and atopic dermatitis were also comparable between two groups (p>0.05).
ConclusionsPrevalences of asthma, allergic rhinitis and atopic dermatitis are similar in children born after IVF and children born after spontaneous conception.
The prevalence of childhood asthma and other allergic diseases have increased tremendously, especially in recent years, despite the absence of a satisfactory explanation for this increase1,2. Up to now, many factors in the antenatal and neonatal periods have been suggested as playing a role in the development of allergic diseases in children3,4.
Since the first child conceived after in-vitro fertilisation (IVF) was born in the UK in 1978, more than one million babies worldwide have been born with this method. Many papers have been published on the health problems of children born after IVF comparing them with children born after spontaneously conceived pregnancies5,6.
The prevalence of allergic diseases and asthma have been studied extensively in normal populations and in some risk groups, yet it is not exactly known if there is an increased risk for allergic diseases and asthma among children born after IVF.
In this study we plan to document the prevalence of asthma, allergic rhinitis and atopic dermatitis among children born after IVF and compared with controls.
Materials and MethodsWe recruited 158 children (mean age: 4.60 ± 2.14years) born after IVF pregnancies in an international hospital between 2002–2004 and 102 children (mean age: 5.27 ± 2.8years) born after spontaneous pregnancies as control group to investigate the prevalences of asthma, atopic dermatitis and allergic rhinitis. All of the parents of children born in the in-vitro fertilisation centre of international hospital were called and invited to join the study and the controls were randomly selected among the children of a day care centre in the hospital from a similar socioeconomic level. The questions in a Turkish version of the International Study of Asthma and Allergies in Children (ISAAC) questionnaire were asked to the parents by telephone or face to face7. The children from both groups with known causes of wheezing such as pneumonia, laryngomalacia/tracheomalcia, congenital heart diseases, cystic fibrosis and gastro-oesophageal reflux were excluded from the study. The study protocol was approved by the institutional ethics committee and verbal consent was obtained from the parents of the children after the aim of the study was described in detail.
Statistical analysisDescriptive statistics were provided for the numeric and categorical variables using means, standard deviations and percent distributions where necessary. Student t test was used to compare quantitative data and Chi-square test and Fisher's Chi-square test to compare qualitative data. A P value of less than 0.05 was used as the cut-off for statistical significance.
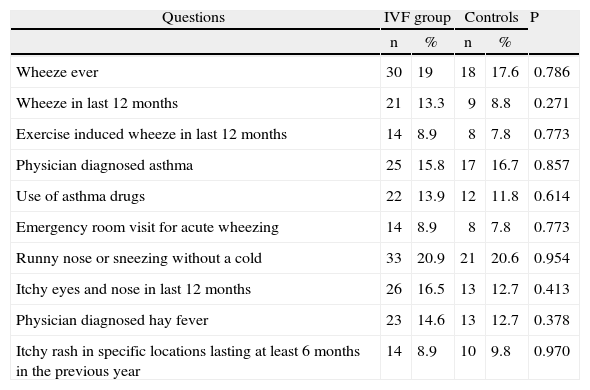
ResultsAlthough more than 250 parents were invited, only parents of 158 children accepted to join the study. The total number of children in the day care centre was about 110 and we did not want to join more controls from other day care centres to maintain the socioeconomic similarity between the study and control groups. Therefore the study group consisted of 40 twins (80 children) and 78 single children; and the control group of 102 children. The female/male ratio was 0.82 among study group and 1.04 among controls (p > 0.05). The mean number of people in the home was also similar (4.3 people in study groups and 4.1 people in controls) (p > 0.05). All of the study and control groups were born in Istanbul. Wheezing ever has been reported in 19 % of the children born after IVF and in 17.6 % of the control group (p > 0.05) (table 1). No significant differences were found between groups, in terms of parental allergic diseases, use of any anti-asthma drugs, physician diagnosed asthma and admission to emergency room with wheezing (p > 0.05). In addition, prevalences of allergic rhinitis and atopic dermatitis were also comparable between two groups (p > 0.05) (table I).
Prevalences of allergy and asthma symptoms in children born after IVF and controls
| Questions | IVF group | Controls | P | ||
| n | % | n | % | ||
| Wheeze ever | 30 | 19 | 18 | 17.6 | 0.786 |
| Wheeze in last 12months | 21 | 13.3 | 9 | 8.8 | 0.271 |
| Exercise induced wheeze in last 12months | 14 | 8.9 | 8 | 7.8 | 0.773 |
| Physician diagnosed asthma | 25 | 15.8 | 17 | 16.7 | 0.857 |
| Use of asthma drugs | 22 | 13.9 | 12 | 11.8 | 0.614 |
| Emergency room visit for acute wheezing | 14 | 8.9 | 8 | 7.8 | 0.773 |
| Runny nose or sneezing without a cold | 33 | 20.9 | 21 | 20.6 | 0.954 |
| Itchy eyes and nose in last 12months | 26 | 16.5 | 13 | 12.7 | 0.413 |
| Physician diagnosed hay fever | 23 | 14.6 | 13 | 12.7 | 0.378 |
| Itchy rash in specific locations lasting at least 6months in the previous year | 14 | 8.9 | 10 | 9.8 | 0.970 |
Although the reasons for the dramatic increase in allergic diseases have not been clarified yet, some important explanations and hypotheses have been proposed to date8. It is generally accepted that a genetic background and exposure to some environmental factors account for the rise in the prevalence of these diseases9.
Thousands of children are now born worldwide every year after IVF, but many studies have suggested that children born after IVF have an increased risk of developing certain health problems such as some malignancies10 and neurological problems11. On the other hand the long-term effects of IVF on the development of allergies and asthma in children born after IVF are not exactly known, although some increased risk has been reported for asthma12. When planning this study we wondered if the hormones and drugs used in IVF caused epigenetic modification in DNA and effect gene expression and thus activated or inhibited the genes related to asthma and other allergic diseases. In our study prevalences of wheeze ever, wheezing in last 12months, symptoms of allergic rhinitis and atopic dermatitis were comparable with former studies from our society13,14. However, prevalences of physician diagnosed asthma and allergic rhinitis were found to be a little higher than in former studies. This may be due to the fact that both the study and control group come from the higher socioeconomic income groups of the population and they visit the hospitals and pediatricians more often than the middle or lower socioeconomic groups.
In conclusion: prevalences of asthma, allergic rhinitis and atopic dermatitis are similar in children born after IVF and children born after spontaneous pregnancies.
