








Introduction. Elevated aminotransferase levels(ATLs) are alert the physicians for liver-affecting disease and may reflect liver injury. We aimed to determine the prevalence of elevated ATLs and the association of elevated ATLs with the metabolic syndrome(MetS) in a northern province of Turkey.
Materials and methods. Elevated ATLs were evaluated among 1,095 individuals of the Tokat Prevalence Study which have been described in detail elsewhere. 1,095 participants had been selected by a simple random sampling method among 530,000 inhabitants in 70 (12 urban and 58 rural) areas in the province of Tokat which is located in the Black Sea Region of Turkey.
Results. The prevalence of elevated serum ALT, AST, and ALT and/ or AST were found as 11%, 7.2%, and 13.3%, respectively. Increased BMI, fatty liver, and MetS were higher in our general population with elevated ATLs. After exclusion of individuals with hepatitis B or hepatitis C infection, 132 individuals with elevated ATLs (91 male and 41 female) were evaluated. MetS was found in 59 participants and its prevalence was markedly higher in females with elevated ATLs (p < 0.0001). When the males with elevated ATLs were evaluated, the ALT levels of the persons who have no risk of MetS (p = 0.007) and the persons who have one risk of MetS (p = 0.001) were lower than the persons with MetS.
Conclusions. Elevated ATLs are common and it’s an important cause is MetS in Northern Turkey.
Elevated aminotransferase levels (ATLs) are alert the physicians for liver-affecting disease and may reflect liver injury. The alanine aminotransferase (ALT) levels are more specific indicators of liver injury than aspartate aminotransferase (AST) levels.1 Some factors like chronic hepatitis, fatty liver, cho-lelithiasis, hyperglycemia, hyperlipidemia, obesity, medications, alcohol consumption, hemochromato-sis, Wilson’s disease, and alphal-antitrypsin deficiency may affect ATLs.1-3 Moreover, some previous studies shown that the prevalence of elevated liver enzymes is higher in individuals with metabolic syndrome (MetS).4,5
The causes of elevated ATLs may change according to ethnicity, geographic region, and develop situation of countries. If these causes (which effect liver enzymes) are known, the most of all factors may be forecast. Thus, the etiologic factor should be determined with low cost and less time.
To date, no study has assessed the relationship of elevated ATLs and the MetS in a population-based study of Turkey. In this study, we aimed to determine:
- 1.
The prevalence of elevated aminotransferase levels.
- 2.
The association of elevated aminotransferase levels with the metabolic syndrome in urban and rural population in a northern province of Turkey.
The individuals of Tokat Prevalence Study, have been described in detail elsewhere,6,7 were evaluated in this study. Briefly, one thousand and ninety five participants had been selected by a simple random sampling method among 530,000 inhabitants in 70 (12 urban and 58 rural) areas in the province of Tokat which is located in the Black Sea Region of Turkey.
All subjects gave informed consent and the study protocol was approved by The Ethics Committee of Gaziosmanpasa University. These individuals were interviewed face to face by an internist and a radiologist. Demographic data were obtained, upper abdomen ultrasonographies were done, weight, height, and waist and hip circumference were measured, and blood samples were drawn for each subject. Waist circumference was measured at the mid-point between the lower border of the rib cage and the iliac crest, whereas hip circumference was similarly obtained at the widest point between the hip and buttock, waist-to-hip ratio was calculated. Fatty liver was diagnosed by ultrasonographic findings of liver-kidney contrast, vascular blurring, and deep atte-nuation.8 Systolic and diastolic blood pressure was measured twice on the right arm with a sphygmoma-nometer (Erka, Germany) and the mean of both measurements used for the analyses.
BMI (kg/m2) was calculated as weight divided by the square of height. Subjects with BMI ≥ 25 kg/m2 were classified as overweight. Physical activity was categorized as scarce, mild, intensive, and competitive. Ethanol intake was assessed by a validated questionnaire and expressed as weekly (g/wk) consumption. The cut-off value listed by the test manufacturer for ALT and AST were 55 U/L and 37 U/L, respectively.
MetS, define according to the Adult Treatment Panel III of the National Cholesterol Education Program, was the identification of 3 of the following 5 risk factors: abdominal obesity (>102 cm in male and >88 cm in female), elevated triglycerides (≥ 150 mg/dL), decreased HDL levels (< 40 mg/dL in male and < 50 mg/dL in female), elevated blood pressure (> 130/85), and elevated fasting plasma glucose levels (>110 mg/dL).
Statistical Analysis: Data are expressed as the mean ± SD. Statistical comparison was done by using the Chi-Square and Independent Samples Test or Mann-Whitney U Test according to distributions or numbers of values. Values of p less than 0.05 were evaluated as statistically significant.
ResultsThe prevalence of elevated serum ALT, AST, and ALT and/or AST were found as 117 (120 indivi-duals), 7.27 (79 individuals), and 13.37 (146 of 1095 individuals), respectively. The mean age of 146 persons were 41.7 ± 16.1 years (range, 18-86) and the rate of male/female was 97/49 (66.4/33.6 percent). In the participants with elevated ATLs, the mean of elevated serum alanine aminotransferase levels in males and in females were 68.7 ± 22.0 U/L and 67.4 ± 31.2 U/L, respectively and statistically significance was not found between gender (p = 0.8). The prevalence of elevated ATLs was higher in males than females (p < 0.0001).
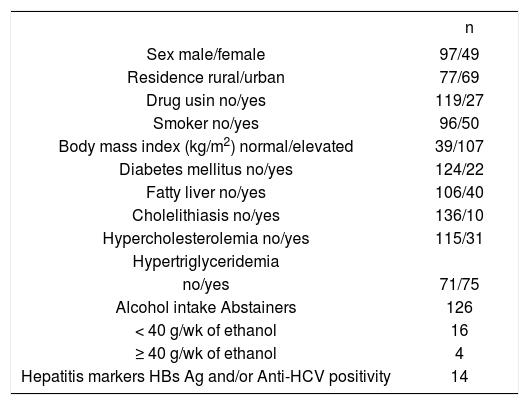
There have a history for drug using in 27 persons (18.57), for smoking in 50 persons (34.27), for alcohol intake (≥ 40 g/wk of ethanol) in 4 persons (2.77), HBs Ag positivity in 8 persons (5.57), and Anti-HCV positivity in 6 persons (4.17). Grade 1, grade 2, and grade 3 steatosis were detected in 25 (17.17), 14 (9.67), and 1 (0.77) individuals of the 146 participants, respectively. The distributions of factors associated with elevated ATLs are shown in table 1. All individuals have a history of at least one risk factor.
Demographic characteristics of individuals with elevated aminotransferase levels (ALT and / or AST).
| n | |
|---|---|
| Sex male/female | 97/49 |
| Residence rural/urban | 77/69 |
| Drug usin no/yes | 119/27 |
| Smoker no/yes | 96/50 |
| Body mass index (kg/m2) normal/elevated | 39/107 |
| Diabetes mellitus no/yes | 124/22 |
| Fatty liver no/yes | 106/40 |
| Cholelithiasis no/yes | 136/10 |
| Hypercholesterolemia no/yes | 115/31 |
| Hypertriglyceridemia | |
| no/yes | 71/75 |
| Alcohol intake Abstainers | 126 |
| < 40 g/wk of ethanol | 16 |
| ≥ 40 g/wk of ethanol | 4 |
| Hepatitis markers HBs Ag and/or Anti-HCV positivity | 14 |
After exclusion of individuals with hepatitis B or hepatitis C infection, 132 individuals with elevated ATLs (91 male and 41 female) were evaluated (Tables 2 and 3). MetS was found in 59 participants (44.7%) (31 of 91 males, 34.1%; 28 of 41 females, 68.3%) of these individuals and its prevalence was markedly higher in females with elevated ATLs (p < 0.0001). Moreover, the prevalence of MetS in the individuals with elevated ATLs were higher than with normal ATLs (p = 0.015). ALT and AST levels in males with MetS were higher than without MetS (p = 0.022 and p = 0.025, respectively) (Table 4).
The p values of comparisons between normal and elevated aminotransferase levels in all participants, male and female.
| All Participants | Male | Female | |
|---|---|---|---|
| No. (normal/elevated*) | 949/132 | 444/91 | 505/41 |
| Age (year) | NS | NS | NS |
| Physical activity | NS | NS | NS |
| Height (cm) | 0.038 | NS | NS |
| Weight (kg) | < 0.0001 | 0.004 | 0.002 |
| Waist circumference (cm) | < 0.0001 | 0.001 | 0.003 |
| Hip circumference (cm) | NS | 0.015 | NS |
| Waist-to-hip ratio | < 0.0001 | 0.009 | 0.023 |
| Systolic blood pressure (mmHg) | NS | NS | NS |
| Diastolic blood pressure (mmHg) | 0.050 | NS | 0.045 |
| Body mass index (kg/m2) | 0.012 | NS | <0.0001 |
| Blood glucose level (mg/dL) | NS | NS | NS |
| Total cholesterol level (mg/dL) | < 0.0001 | < 0.0001 | 0.002 |
| LDL cholesterol level (mg/dL) | 0.004 | 0.024 | 0.005 |
| HDL cholesterol level (mg/dL) | 0.040 | NS | 0.010 |
| Triglyceride level (mg/dL) | < 0.0001 | < 0.0001 | 0.003 |
* Except the individuals with hepatitis
NS: Not significant;
The comparisons of participants with elevated aminotransferase levels according to metabolic syndrome.
| All participants (n=132) | Male (n=91) | Female (n = 41) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| MetS (+) (n = 59) | MetS (-) (n = 73) | p-value | MetS (+) (n = 31) | MetS (-) (n = 60) | p-value | MetS (+) (n = 28) | MetS (-) (n = 13) | p-value | |
| Age, year | 46.1 ± 15.9 | 38.6 ± 14.7 | 0.006 | 43.6 ± 17.0 | 39.5 ± 15.3 | NS | 48.8 ± 14.4 | 34.6 ± 9.1 | 0.002 |
| ALT | 71.4 ± 28.3 | 64.6 ± 22.8 | NS | 76.8 ± 29.3 | 63.4 ± 15.8 | 0.022 | 65.5 ± 26.4 | 70.3 ± 43.0 | NS |
| AST | 42.8 ± 15.4 | 35.6 ± 9.8 | 0.003 | 40.1 ± 13.3 | 34.0 ± 8.8 | 0.025 | 45.7 ± 17.3 | 43.2 ± 11.2 | NS |
MetS: Metabolic syndrome. NS: Non significant.
Alcohol intake (p = 0.015), smokers (p < 0.0001) and drug using (p = 0.002) were higher in individuals with elevated ATLs.
The participants with MetS had more elevated ALT levels compared with the participants without MetS, but this difference was not significant (71.4 ± 28.3 U/L vs. 64.6 ± 22.8 U/L, p = 0.136).
When the males with elevated ATLs were evaluated, the ALT levels of the persons who have no risk of MetS (p = 0.007) and the persons who have one risk of MetS (p = 0.001) were lower than the persons with MetS (Figure 1, Table 5). However, there were no statistical significant in females with elevated ATLs for risk factors of MetS.

The distributions of risk factors for metabolic syndrome in men with elevated aminotransferase levels.
| Metabolic Risk Factors | ||||
|---|---|---|---|---|
| No risk | One risk | Two risk | > Three risk (MetS)* | |
| No. | 10 | 23 | 27 | 31 |
| Mean ALT | 59.8 ± 12.8 | 59.6 ± 12.6 | 68.0 ± 18.3 | 76.8 ± 29.3 |
* Metabolic syndrome.
The ALT levels of the participants with elevated aminotransferase in living rural and urban areas are 67.2 ± 26.7 and 68.1 ± 24.4, respectively (p = 0.837). Similarly, we didn’t find statistically significant differences in males and females according to residence (p = 0.775 and p = 0.576, respectively).
DiscussionThe prevalence of elevated serum ATLs (ALT and / or ASTA was found 13.3% in our asymptomatic general population. Moreover, about 117 of our participants (120 persons) had elevated ALT levels. Ioannou et al found that the prevalence of elevated ALT, AST, or either ALT or AST were 8.9%, 4.9%, and 9.8%, respectively.9 Jamali et al in general population of Iran10 and Liu et al in Taiwan11 declared that the elevated ALT levels were 7.9% and 7.2%, respectively. Papatheodoridis et al found that elevated liver enzymes are present in approximately 15% of Greek blood donors.12 Our study showed that the prevalence of elevated ATLs was relatively higher in our population. Although the prevalence of alcohol consumption is very low, this result may relate to the increased ratio of smoking, hepatitis, obesity, and MetS.
It was demonstrated that elevated aminotransfe-rase levels have a relationship with features of the MetS.13-15 The most common causes associated with elevated ATLs were elevated BMI, fatty liver, and MetS in our general population. Interestingly, the participants with the MetS had more elevated ALT levels than those without the MetS. However, this difference was not significant. The prevalence of MetS in individuals with elevated ATLs was higher in females than males. Moreover, elevated ATLs have been associated with at least one etiologic factor such as MetS, fatty liver, drug using, hepatitis, etc. in all participants. However, we found that ALT levels have a relationship with risk of MetS only in males with elevated ATLs.
The waist circumference is an important marker of central obesity.16 When we were evaluate hip-waist circumference, waist-to-hip ratio and BMI bet-ween the participants with normal and elevated ATLs, there were a statistical significant for waist-to-hip ratio as waist circumference. This finding shows the importance of waist-to-hip ratio. De Lé-dinghen, et al. found that liver fibrosis is statistically associated with tobacco use, elevated BMI and diabetes in 272 asymptomatic patients with unexplained chronically elevated ALT levels.17 Elevated ATLs were more common among males than fema-les.12,17,18 Similarly, our study confirmed that the ratio of elevated ATLs was higher in males and in smokers.
Fatty liver was found in 64% of 149 asymptomatic participants with elevated serum aminotransfera-ses.19 Daniel et al demonstrated that a lot of participants with chronic elevated transaminase have liver steatosis.20 Liver biopsy is often recommended in patients with elevated serum aminotrans-ferases in order to determine the causes. It was a deficiency of our study that we did not perform liver biopsy.
ConclusionElevated aminotransferase levels are common and MetS is an important cause of elevated ATLs in Northern Turkey. The ALT levels increase with the number of risk of the MetS in males. Moreover, the results of our study indicate that the most common causes associated with elevated ATLs may be prevented with lifestyle modification such as dietary habits, physical activity in our population.
Abbreviations- •
ATLs: Elevated aminotransferase levels.
- •
MetS: Metabolic syndrome.
- •
ALT: Alanine aminotransferase.
- •
AST: Aspartate aminotransferase.
This project was funded by The Society of Science Research Projects in Gaziosmanpasa University, Project number: 2005/26.
recomendados



![]()
