





Abstracts from XVII Mexican Congress of Hepatology
Más datosHemolytic anemia can be associated with various types of solid tumors; however, in hepatocarcinoma, it is extremely rare.
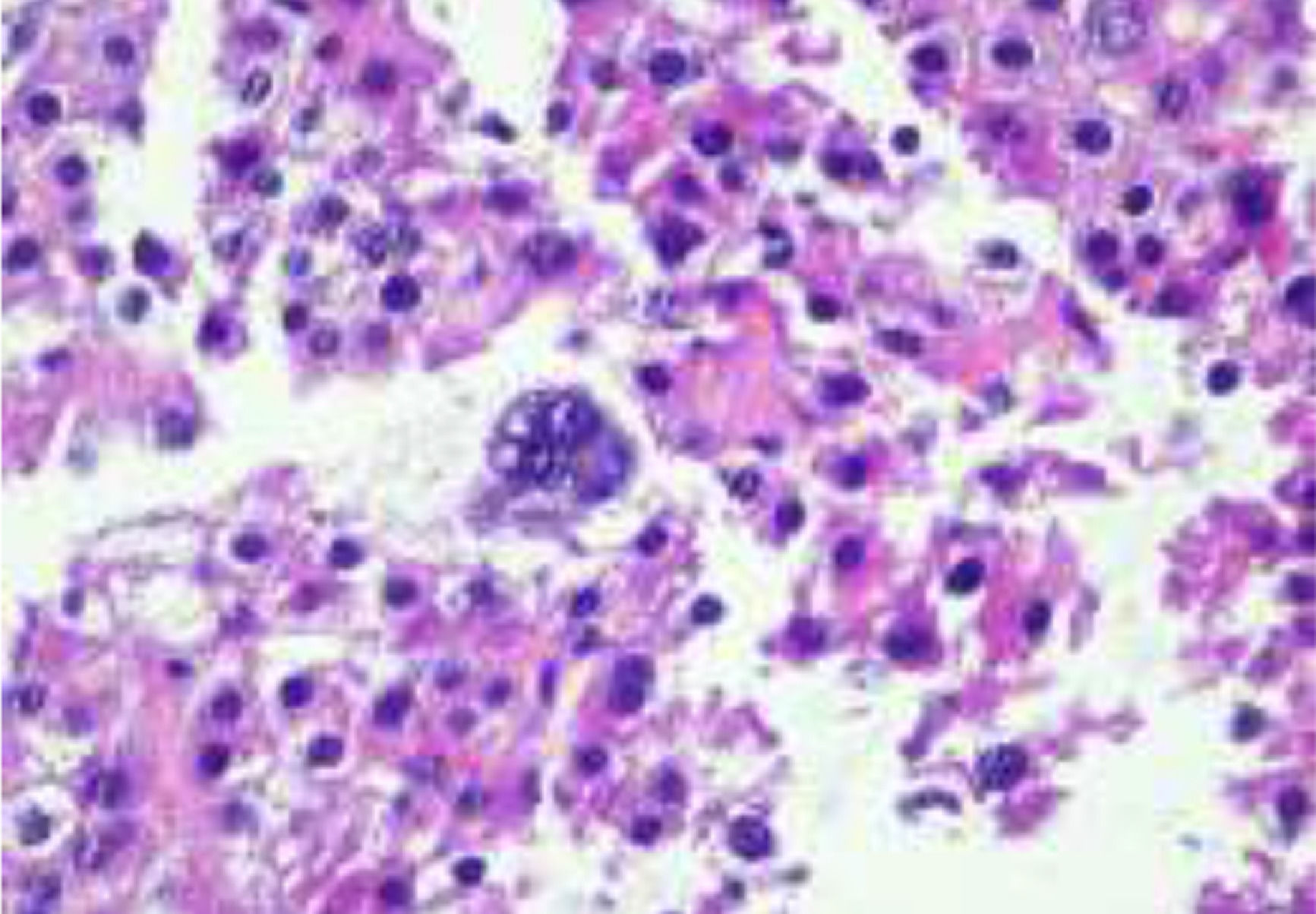
Case SummaryMan 74 years old. Symptoms of two months with dyspnea, asthenia and adynamia. On physical examination, generalized pale skin and sclera, normal heart and lung area, soft, depressible abdomen, with peristalsis present, palpation of the liver edge 5 cm below the costal margin. Laboratories with leukocytes 6.1 103/Al, neutrophils #4.1, lymphocytes #1.3, HB 6.2 g/dL, HTC 16.8%, MCV 103fL, HCM 38pg, platelets 395.00 103/Al; BD 0.5 mg/dL, BI 2.80 mg/dL, BT 3.30 mg/dL, DHL 403 IU/L. Direct Coombs is performed positive dilution 1:128. FSP with anisocytosis, red blood cell agglutination, macrocytosis and macroplatelets, reticulocytes 1.48%, alpha-fetoprotein 12.7 IU/mL. Warm antibodies (IgG) attached to the erythrocyte membrane were documented. Simple and contrast-enhanced abdominopelvic tomography, with images suggestive of multifocal cellular hepatocarcinoma. Liver biopsy, which reports findings of hepatocarcinoma. Management with oral steroid drugs was initiated jointly, reversing the hematological alterations without requiring blood products.
DiscussionThere are few cases in the medical literature on hematological alterations associated with solid tumor metastases. In this case, the hematological involvement of the patient was not due to metastasis but to a paraneoplastic syndrome since the first manifestation found was anemia with jaundice secondary to hemolysis.
ConclusionThe diagnosis must be reached by exclusion, ruling out other causes such as primary hematological alterations, metastases, or vascular processes.
FundingThe resources used in this study were from the hospital without any additional financing
Declaration of interestThe authors declare no potential conflicts of interest.



