



Hepatic inflammatory myofibroblastic tumors are uncommon low grade malignant neoplasms. They can be confused clinically and by imaging studies with abscess.
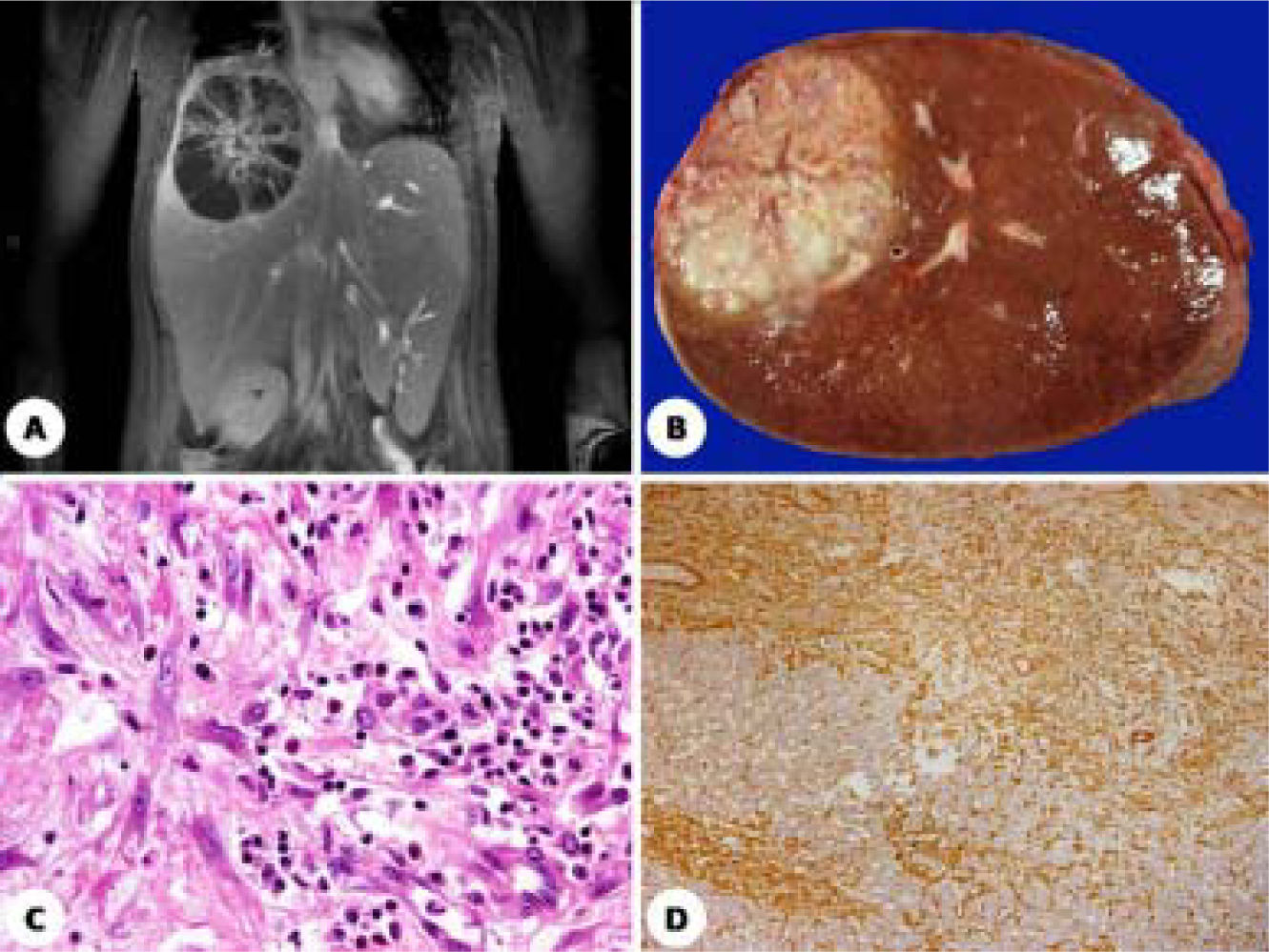
Six days before admission to the hospital this 23 year-old woman developed fever, diaphoresis and right hypochondrium pain. Laboratory studies showed only leukocytosis. An ultrasound and computed tomography revealed an heterogeneous rounded hepatic lesion of 7 cm in greatest dimension (Figure 1A). The clinical and radiological diagnosis was pyogenic hepatic abscess. The patient received antimicrobial treatment but the high fever persisted. A right hepatic lobectomy was performed. Grossly, a non-encapsulated but well demarcated hepatic tumor with central necrosis of 11 cm in greatest dimension was seen (Figure 1B). Microscopically, the tumor was composed of spindle myofibroblastic cells arranged in fascicles. The neoplastic cells were mixed with numerous leukocytes, lymphocytes and plasma cells (Figure 1C). The myofibroblastic cells were strong and diffusely positive for smooth muscle actine (Figure 1D). Cellular atypia or mitotic figures were not present. The central portions of the tumor showed necrosis and numerous foamy macrophages. The diagnosis of hepatic inflammatory myofibroblastic tumor was made.
Discussion. D. Diffuse immunoreactivity for smooth muscle actine.")
Inflammatory myofibroblastic tumors (IMT) have been reported in many anatomic sites, including lung, urinary bladder, breast, pancreas, large bowel, prostate, orbit, liver, extrahepatic bile ducts, etc.1-4Hepatic myofibroblastic tumors are exceedingly rare and occur in adult men with a mean age of 56 years.4 Its size is variable from 1 to 20 cm. Some of these tumors may simulate abscess because of the abundant inflammatory infiltrate and central necrosis. Inflammatory myofibroblastic tumors recur locally (25%) while others behave as low grade malignant neoplasms that can metastasize (< 5%).3 Some inflammatory myofibroblastic tumors have been associated with autoimmune pancreatitis and primary sclerosing cholangitis.5 In these cases, the IgG4 serum levels are elevated and therefore useful in the diagnosis. Immunohistochemistry for IgG4 usually shows numerous IgG4-positive plasma cells.5 In a few reports, inflammatory myofibroblastic tumors have also been associated with Epstein-Barr virus infection.



