



Few years ago the distribution of hepatitis C virus (HCV) genotypes in Mexico was unknown. An important exception is the study written by Alvarado-Esquivel et al in 1998. That study reported results of 516 blood donors from 21 states obtained in two referrals blood-banks, and 235 patients with liver disease from the States of Mexico, Jalisco, Michoacan and Oaxaca.1 In the last year four studies on this topic were published in different journals, even one in Annals of Hepatology.2 These new studies intended to obtain «national representativeness». The genotypic variability of HCV has implications that included differences in pathogenecity,3,4 sensitivity of diagnostic techniques,5 response to treatment, and vaccine efficacy.6 For this reason it’s important to review the methodology used in each study, and their findings (consistencies and inconsistencies). Afterwards, it will be possible to define a better picture of the genotype distribution of HCV in Mexico. In this sense, it is important to remember that, in addition to clinical objectives for each infected patient, from a public health perspective the occurrence recognition of a disease is one important step to identify and promote preventive strategies, and define cost-effectiveness treatments. In this letter we want to analyze briefly the methodology used in these papers, and propose a national distribution of HCV genotypes.
The first study was written by Chiquete & Panduro.7In this study they carried out a systematic review of studies indexed in Medline, Imbiomed, MedicLatina, Artemisa and Medigraphic databases. The authors found three articles with information on genotype distribution in Mexico, two of them were multicenter studies. One of these two latter studies is also an abstract from the Dehesa-Violante et al study.8,9 To obtain a unique estimator to each genotype we calculated the mean of these three observations since the homogeneity of data included. Sánchez-Avila et al included in their study patients infected with HCV (n = 1 390) from different regions of the country (2003-2006), previous to receive antiviral treatment. The biological samples were analyzed in the Quest Diagnostics Nichols Institute, San Juan Capistrano, CA.2 The study by Dehesa-Violante et al, reported the genotype distribution of patients from 22 hospitals of some Mexican cities (Ciudad Obregón, Cualiacán, Guadalajara, México City, León, Monterrey, Puebla, Tijuana, Torreón, and Veracruz). More recently, Santos-Lápez et al,10 reported the findings of a new systematic review. The search was realized in PubMed, MedicLatina, Imbiomed, Medigraphic, and Scielo databases. Data were extracted from 11 studies with asymptomatic and high-risk subjects. Given the relative homogeneity of data, we summarized the information with the mean again. All these estimates are shown in Table I. Note that results are similar, but with some differences related to genotypes 3, 4 and 5.
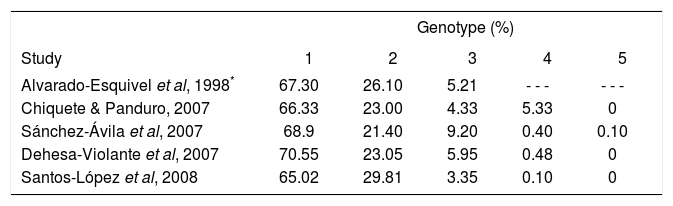
Distribution of hepatitis C virus genotypes in Mexico according to studies with «national representativeness».
| Genotype (%) | |||||
|---|---|---|---|---|---|
| Study | 1 | 2 | 3 | 4 | 5 |
| Alvarado-Esquivel et al, 1998* | 67.30 | 26.10 | 5.21 | - - - | - - - |
| Chiquete & Panduro, 2007 | 66.33 | 23.00 | 4.33 | 5.33 | 0 |
| Sánchez-Ávila et al, 2007 | 68.9 | 21.40 | 9.20 | 0.40 | 0.10 |
| Dehesa-Violante et al, 2007 | 70.55 | 23.05 | 5.95 | 0.48 | 0 |
| Santos-López et al, 2008 | 65.02 | 29.81 | 3.35 | 0.10 | 0 |
Representativeness is the most important consideration to define which study is better to obtain national estimators of occurrence. A sample is representative when the variable distribution reflects the distribution of the original population, and it doesn’t require to be a probability sampling method.11 In this sense, the study of Sánchez-Avila et al2 better fulfills the requirement of representativeness because it selected individuals from different Mexican regions, and it was the only study that reports regional differences in the genotype 3 distribution and the presence of genotype 5. When we compared the proportions described in the articles, it was possible to find differences between studies related with the distribution of HCV genotype 3. In conclusion, based on the available data we suggest that the most prevalent HCV genotypes are 1 and 2. The other genotypes have lesser prevalences, but and specific estimator of each one is not available. Further studies may explore the distribution of non-1/2/4 genotypes. Until now, we consider that the study published in Annals of Hepatology, is the best available evidence on this topic. Further epidemiological studies will permit to improve the accuracy of these preliminary estimations.
Conflict of interestsAJI received research funds from Schering-Plough, Mexico, for participation in a pharmacoeconomic study on treatment of HCV infection.



