


The “accordion effect” is a mechanical remodeling of the arterial wall produced by endoluminal introduction of stiff guidewires, leading to vessel wall shortening and development of multiple eccentric constrictions. This phenomenon is unresponsive to vasodilators and may lead to unnecessary stenting of the pseudo-lesions. It must be suspected with the development of multiple lesions and when a tortuous artery assumes a linear shape after advancing distally a stiff wire. In the situation of a complete occlusion of the artery the diagnosis may be challenging. Stenting in this scenario can be demanding because of the difficulty to appropriately size the length of the stent to the true lesion. We present a case of an unrecognized accordion phenomenon in an occluded coronary artery with a long dissection treated with two stents that after retrieving the wire were insufficient to cover the whole dissection.
El «efecto acordeón» es una remodelación mecánica de la pared arterial producida por la introducción endoluminal de guías de alambre rígido, que provoca un acortamiento de la pared vascular y la aparición de múltiples constricciones excéntricas de la misma. Este fenómeno no responde a los vasodilatadores y puede dar lugar a la colocación innecesaria de endoprótesis para tratar estas seudolesiones. Deben sospecharse ante la aparición de múltiples lesiones asociadas a una arteria coronaria tortuosa que asume una forma lineal después de avanzar distalmente una guía de alambre rígido dentro de la misma. Cuando se presenta una oclusión completa de una arteria coronaria, el diagnóstico suele ser difícil. La selección de la endoprótesis, en este escenario, debe ser la apropiada dada la dificultad que presenta la elección adecuada de la longitud de la endoprótesis a implantar para tratar la verdadera lesión. A continuación se presenta el caso de un fenómeno de acordeón no comunicado en una arteria coronaria ocluida con una disección coronaria larga tratada con 2 endoprótesis, y en el que después de retirar la guía de alambre se presenta una falta de cobertura en la totalidad de la disección inicial.
The terms “crumpled coronary artery or accordion effect” are used to describe a transient angiographic effect observed during percutaneous angioplasty and produced by vessel wall shortening of tortuous segments, attributed to crumpling, invagination or intussusceptions with accordion like appearance.1,2 It is a reversible phenomenon that can cause narrowing and ischemia and must be recognized because it is not responsive to vasodilators, and disappears by retrieving the stiff part of the wire.3
Stenting of lesions in “crumpled” coronary arteries may be challenging because of the difficulty in assuming the length and position of the real stenosis, avoiding stenting of pseudo-stenosis.
We present a case in which two overlapping stents were deployed entirely covering a long dissection, and after retrieving the wire the artery recovered its normal shape and length, and an uncovered gap appeared between the stents.
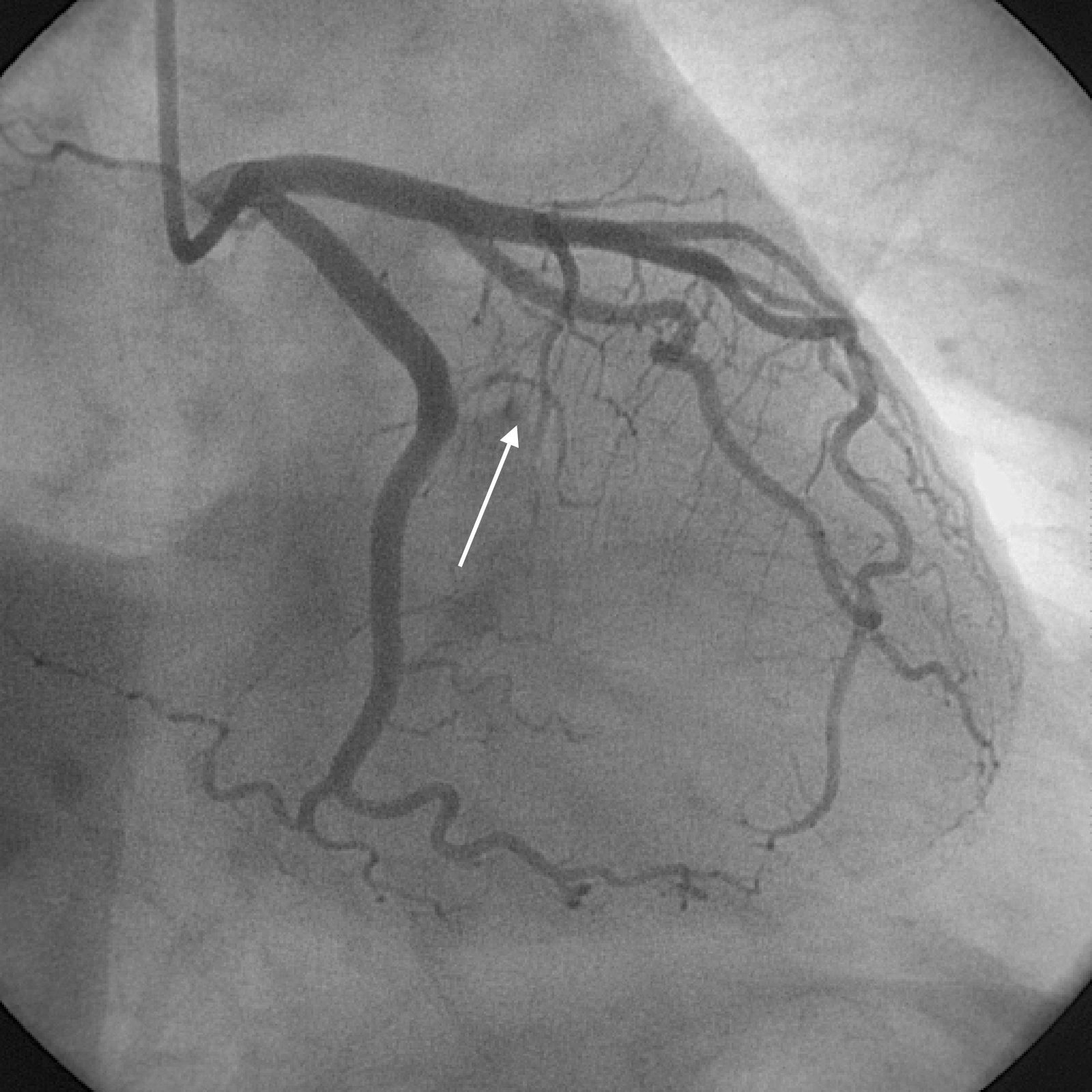
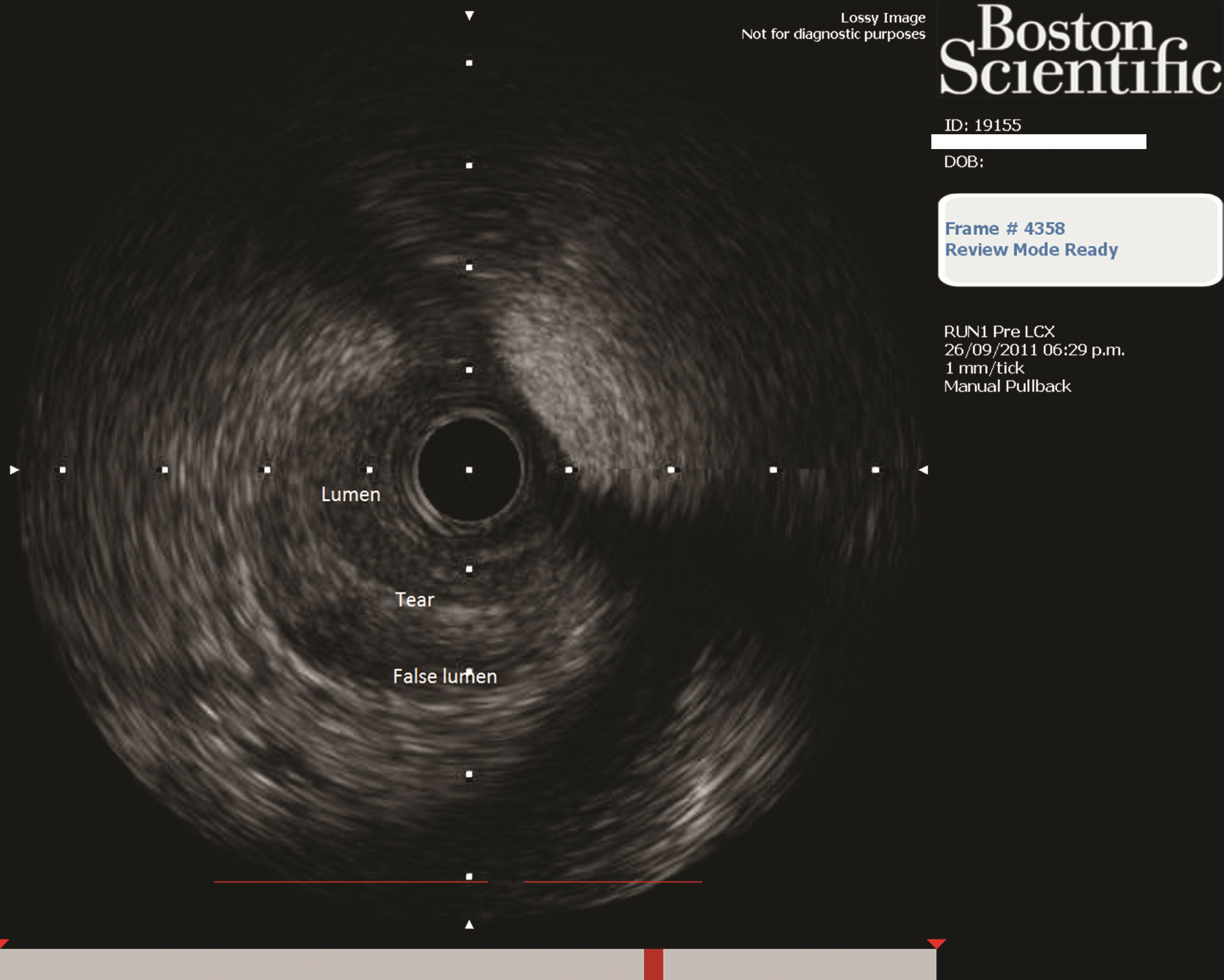
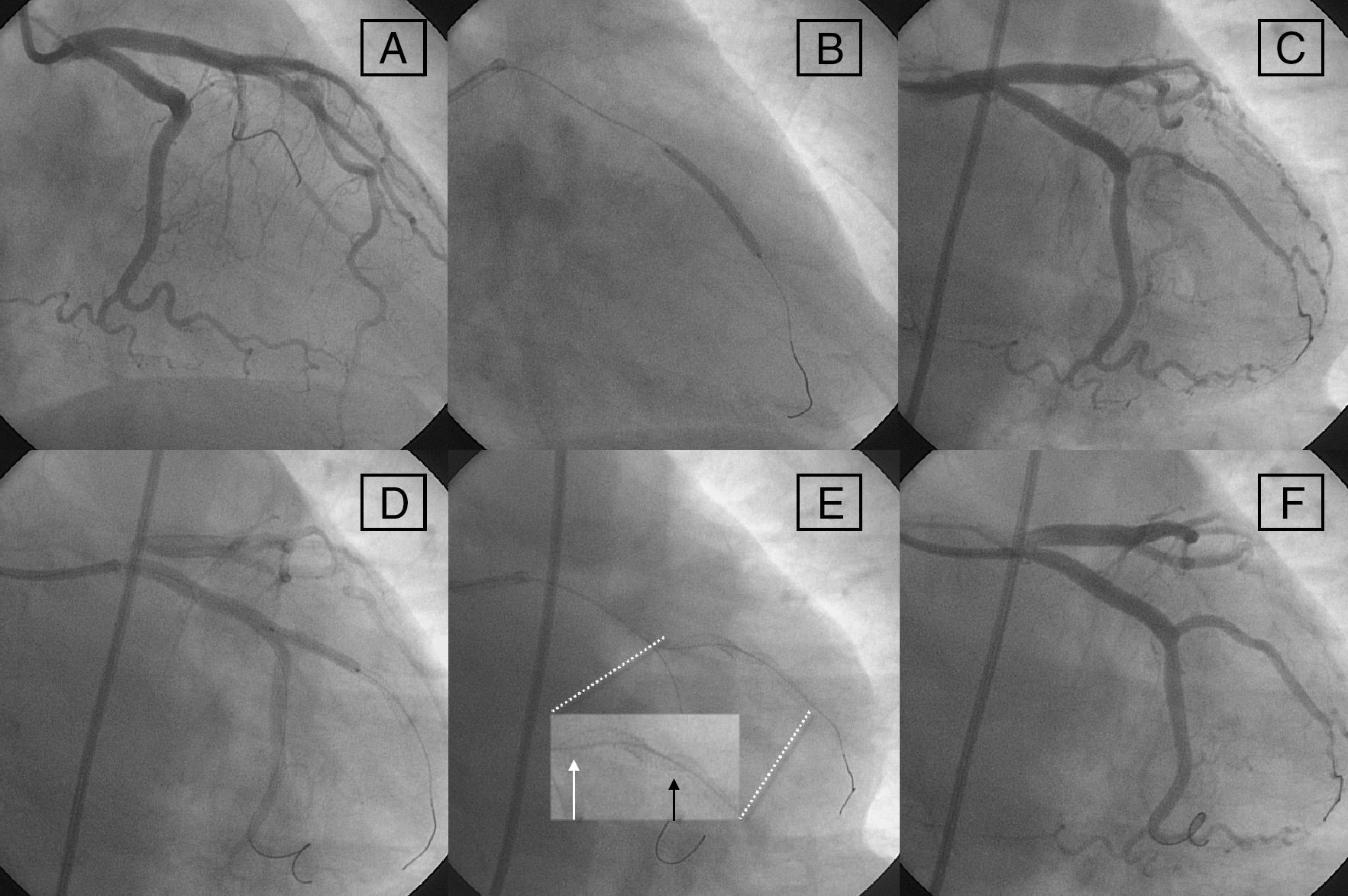
Case reportA 52-year-old woman, without history of heart disease or risk factors was admitted in the Coronary Care Unit (CCU) with an acute myocardial infarction and immediately transferred to the Cath Lab for primary angioplasty. Coronary angiography revealed a complete occlusion of the first marginal branch without evidence of atheromatosis in the remaining vessels (Fig. 1). After beginning anticoagulation with unfractioned IV heparin a 6 Fr EBU 3.5 (Medtronic, Inc.) guiding catheter was positioned in the left ostium. A 0.014in. Choice® Floppy guidewire (Boston Scientific) was advanced with some difficulty through the occluded vessel and a 2.5mm×20mm Maverick® balloon (Boston Scientific) was inflated with only partial restoration of the lumen and incomplete distal filling. An Atlantis® SR Pro (Boston Scientific) intravascular ultrasound catheter (IVUS) was advanced and a long dissection extending from the ostium to the distal part of the artery was observed (Fig. 2). In that moment two PROMUS® (Everolimus-Eluting Coronary Stent, Boston Scientific) stents, 2.25mm×24mm and the second one of 2.25mm×16mm were deployed with 1mm overlapping between them, thus completely covering the long dissection and restoring normal flow (Fig. 3A–F).


 Filiform filling of 1st MB; (B) distal stent deployment; (C) angio post distal stent; (D) proximal stent deployment; (E) stents correctly positioned from the ostium of the 1st MB (white arrow in zoom) with 1mm overlapping (black arrow in zoom) between them; and (F) final result without retrieving the wire.")
Angioplasty sequence in RAO. (A) Filiform filling of 1st MB; (B) distal stent deployment; (C) angio post distal stent; (D) proximal stent deployment; (E) stents correctly positioned from the ostium of the 1st MB (white arrow in zoom) with 1mm overlapping (black arrow in zoom) between them; and (F) final result without retrieving the wire.
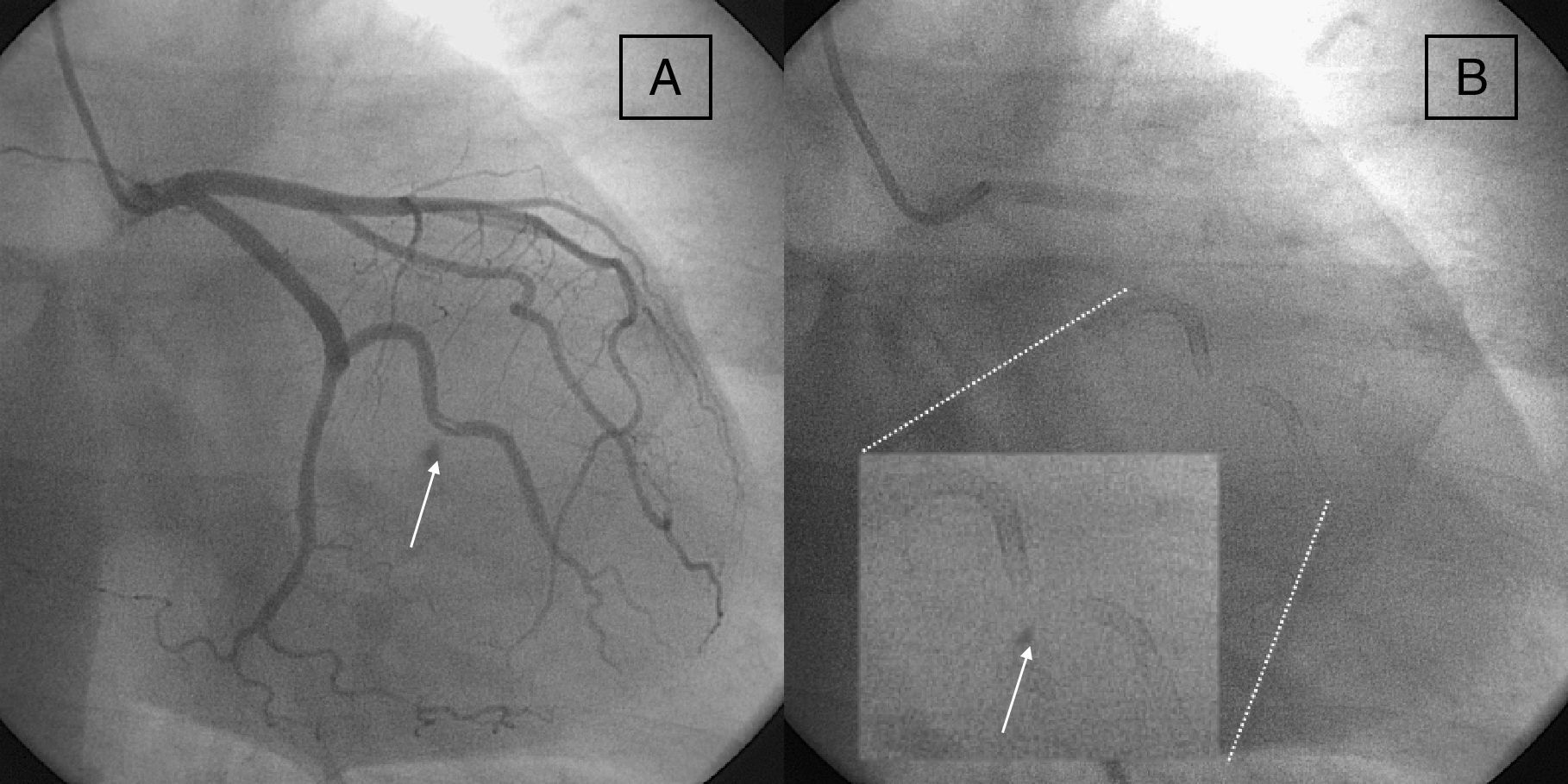
After retrieving the wire a new angio showed two gaps, one between the ostium and the proximal side of the proximal stent, and another between the two deployed stents, with a nonocclusive dissection between the stents (Fig. 4A and B). We tried to reposition the 0.014in. wire in the artery but the attempt was unsuccessful because of the tortuosity of the vessel and the struts of the stents, so we decided conservative management.
 Note the dissection in the mid portion of the artery (white arrow). (B) Note the gap between the previously overlapped stents (white arrow in zoom). RAO=right anterior oblique.")
The patient had an uneventful recovery and was discharged 72h later. A stress test with eco performed two months later was normal.
DiscussionThe “accordion effect” during the course of routine coronary angioplasty has been reported previously and is not uncommon.4,5 It can be described as a spasmodic shortening of a tortuous vessel that mimics bowel intussusceptions and is produced only when the stiff part of the wire is inside the artery. It was unresponsive to vasodilators, and disappears by completely removing the wire or keeping inside only its floppy tip.6 This can lead to a true ischemia and significant intracoronary pressure gradients have been observed, this is why the term “pseudostenosis” should be replaced by “transient or functional” stenosis.7–9 Intravascular ultrasound may be useful for ruling out severe atherosclerosis and coronary dissections; severe lumen asymmetry and a characteristic image of a flattened, three layered wall, overlying a hypoechogenic space have been associated with this phenomenon.10 It has been proposed to advance a microcatheter as an alternative to confirm the diagnosis without loosing the distal position.11 The development of transient stenosis may lead to unnecessary ballooning or stenting of undiseased segments.12
In this scenario, stenting of the real lesion may be challenging. In this case of a young woman with an acute myocardial infarction, the first marginal branch was totally occluded; distal positioning of a floppy wire was difficult but possible and after inflating the balloon the lumen was only partially restored. The suspicion of a long dissection as the main mechanism of the occlusion was confirmed with IVUS. Deployment of the two stents was easy and special care was taken in the ostial position of the proximal stent and in overlapping with the distal stent in order to cover the whole dissection. After retrieving the wire the artery assumed a tortuous shape and two uncovered gaps appeared, one between the ostium of the marginal branch and the proximal margin of the stented segment, and the other between the two stents (previously overlapped stents). Neither the proximal nor the distal stents moved from its original place. Our diagnosis is that the artery was crumpled and after retrieving the wire assumed its original length, thus leaving two small dissected segments without stent covering. The diagnosis of “accordion effect” could not be previously done in a totally occluded artery with a long dissection.
ConclusionsStenting of a crumpled coronary artery may be challenging. Special attention has to be observed in order to achieve a complete covering of the diseased segment without stenting undiseased segments of the vessel. When the accordion effect is suspected, an angiography with only the floppy tip of the wire or a microcatheter inside the artery has to be done, if possible, before stent deployment.
FundingThe authors declare not receiving any funding for this study.
Conflicts of interestThe authors declare that they have no conflicts of interest.