


Objective: Our aim was to evaluate the effect of the baroreflex mechanism upon peripheral blood volume during sympathetic stimulation by orthostatism.
Methods: Nineteen clinically healthy volunteers were included (12 men), 28.4 ± 6.2 years old. Blood pressure was monitored with a Finometer and blood volume with a photoplethysmograph during supine position and orthostatism (15 minutes each), in order to obtain systolic blood pressure (SBP), diastolic blood pressure (DBP), systolic volume (SysV), diastolic volume (DiaV), and inter beat intervals (IBI) measurements. Baroreflex sensitivity index (IBI/SBP) and baroreflex effect on blood volume (IBI/SysV) were estimated by the sequence method. The pertinence of using only systolic values was tested by linear regression analysis of systolic versus diastolic measurements.
Results: More than 70% of DBP and DiaV variations can be explained by SBP and SysV, respectively (p<0.001), with coherence >0.5 in frequencies between 0.04 and 0.15 Hz. IBI/SBP and IBI/SysV were linearly correlated (r>0.4) and both decreased during orthostatism (p<0.05).
Conclusion: The sequence method showed a strong baroreflex effect upon peripheral blood volume that became more apparent during sympathetic stimulation with orthostatism. This approach could be clinically useful for the evaluation of blood volume regulation for many diseases such as diabetes mellitus and heart failure, and during therapeutic interventions such as hemodialysis.
Objetivo: Evaluar el efecto del mecanismo barorreflejo sobre el volumen sanguíneo periférico durante estimulación inducida por ortostatismo.
Métodos: Se incluyeron 19 voluntarios sanos (12 hombres), con edad de 28.4 ± 6.2 años. La presión arterial se midió con un Finometer y el volumen sanguíneo con un fotopletismógrafo, ambos durante posiciones supina y ortostatismo activo (15 minutos cada una), para obtener los valores de presión arterial sistólica (PAS), presión arterial diastólica (PAD), volumen sistólico (VS), volumen diastólico (VD) e intervalo inter pulso (IIP). Se estimó la sensibilidad barorrefleja (IIP/PAS) y el efecto barorreflejo sobre el volumen sanguíneo (IIP/VS) mediante el método de secuencias. La pertinencia de usar sólo variables sistólicas, se evaluó mediante análisis de regresión lineal de las mediciones sistólicas versus las diastólicas.
Resultados: Más de 70% de las variaciones de presión arterial diastólica y volumen diastólico pueden ser explicadas mediante presión arterial sistólica y volumen sistólico, respectivamente (p<0.001), con coherencia >0.5 en frecuencias entre 0.04 y 0.15 Hz. IIP/PAS y IIP/VS tuvieron correlación positiva (R>0.4) y ambos disminuyeron durante ortostatismo (p<0.05).
Conclusiones: El método de secuencias demostró un importante efecto barorreflejo sobre el volumen sanguíneo periférico que se hizo más notable durante estimulación simpática con ortostatismo. Este enfoque podría ser clínicamente útil en la evaluación de la regulación del volumen sanguíneo en distintas enfermedades como diabetes mellitus o falla cardiaca, y durante intervenciones terapéuticas como la hemodiálisis.
Introduction
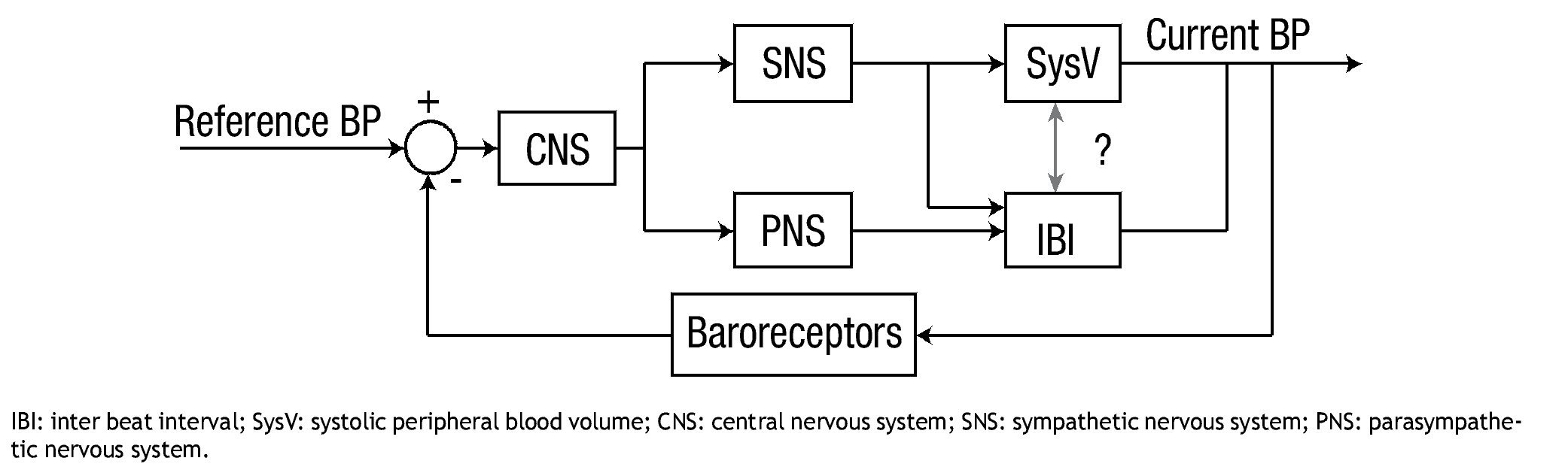
The baroreflex mechanism allows an adequate short-term control of blood pressure (BP), in response to daily-life stimuli such as orthostatism.1-3 The neural and cardiovascular components of the baroreflex mechanism are complex, both anatomically and physiologically.4,5 However, the basic baroreflex function is often referred as a negative feedback mechanism, as it is illustrated in Figure 1. The reference variable (i.e. the BP) is "monitored" by the central nervous system through the baroreceptors, and in response to changes of BP, the central nervous system modulates the autonomic activity towards the heart and blood vessels, with the aim of increasing or decreasing BP by changes in heart rate (or inter beat interval, IBI) and peripheral arteries resistance.2,6 The baroreflex sensitivity is then defined as the magnitude of the change in IBI with respect to a change in BP,7 which normally takes effect between 1 to 3 seconds of the BP change (baroreflex delay).8-11
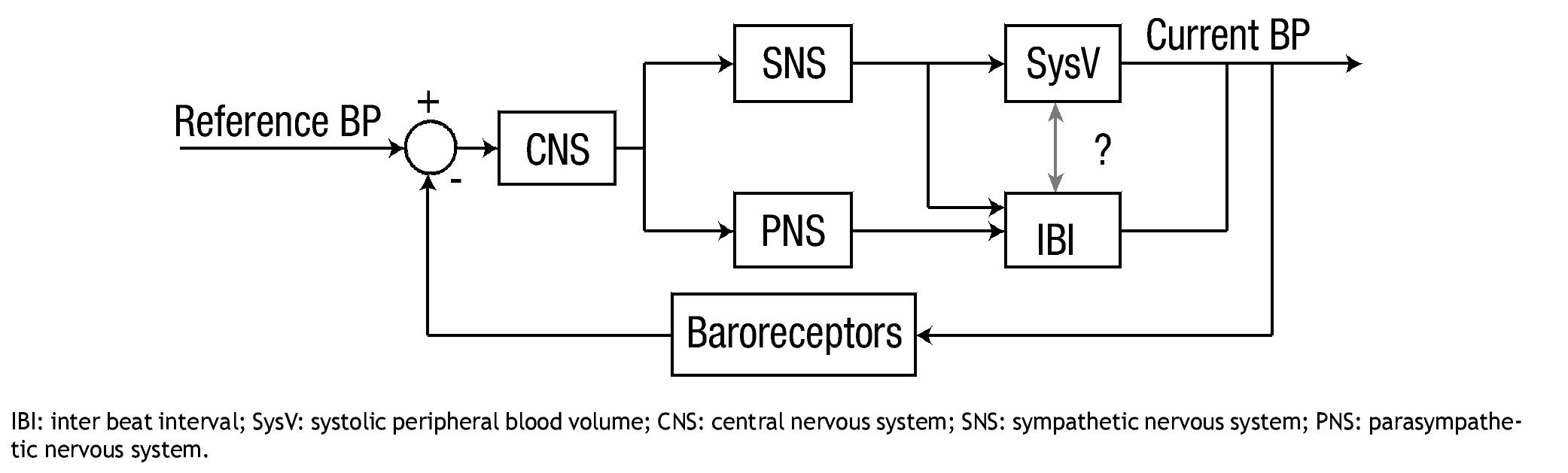
Figure 1. The control of blood pressure (BP) by the baroreflex mechanism is represented as a negative feedback system.
Impairment of the baroreflex mechanism, evidenced by decreased baroreflex sensitivity, occurs in many diseases such as essential arterial hypertension,1,12 diabetes mellitus,13 myocardial infarction14 and chronic renal failure.15 Two examples of clinical implications are: 1) the association of low baroreflex sensitivity with a high risk of cardiac mortality in patients with myocardial infarction,14and 2) the observation of reduced baroreflex sensitivity during hypotension in patients with chronic renal failure prone to intra-hemodialysis hypotension.16
Several non-invasive methods for baroreflex sensitivity evaluation have been developed,7,17,18 that have contributed to the understanding of the pathophysiology of the baroreflex mechanism. However, most studies are focused on the heart rate as the controlled variable, and little is known about the effect that the baroreflex has upon the peripheral blood volume. Considering that sympathetic regulation of peripheral resistance is one of the regulated variables necessary to control BP,6 we hypothesize that, given that the blood volume regulation has an important role on the cardiovascular control through the baroreflex mechanism19,20 this contribution must be seen in photoplethysmographic recordings. According to the representation proposed in Figure 1, correlated changes in systolic blood volume (SysV) and IBI (highlighted by a question mark) could be associated to sympathetic control on both variables. In that case, and considering no other confounding variables, the spectral coherence between both signals would be significant within the frequency band of 0.04 to 0.15 Hz. Furthermore, the effect of the baroreflex mechanism has been studied by systolic blood pressure (SBP) in most methods, but the equivalence of using systolic measurements or diastolic values has not been tested.
The aim of this work was to evaluate the effect of the baroreflex mechanism upon the peripheral blood volume as it is seen by photoplehysmography. Linear regression analysis was applied to the systolic and diastolic measurements of BP and photoplethysmographic volume (PV), to test the pertinence of using only the systolic values in the subsequent analysis. We applied a non-invasive method for assessment of baroreflex sensitivity to measurements of SBP, SysV and IBI, both in supine position and during active orthostatism.
Methods
Subjects
The study included 19 volunteers (12 men and 7 women) with age 28.4 ± 6.2 years old and body mass index 26.5 ± 4.6 kg/m2. All participants were evaluated as healthy by a physician based on the medical history and physical examination only. The participants were not smokers, and were asked to avoid intake of medications or stimulants such as caffeine during 12 hours before the study. The study protocol was completely non-invasive, it complies with the ethical standards laid down in the 1964 "Declaration of Helsinki", and informed consent was obtained from each participant.
Recording equipment
BP was recorded with a Finometer (Finapress Medical Systems),21 and PV was obtained by a previously validated photoplethysmograph.22 The PV signal was incorporated into a channel of the Finometer, in order to capture and digitize simultaneously both signals (BP and PV) with the same equipment. The photoplethysmographic signal is associated with blood volume changes in the microvascular bed of tissue.23 Since PV is not a direct quantitative measurement, it is represented in arbitrary units (a.u.). The sampling frequency was predefined by the Finometer equipment as 200 samples per second, which complies with the international recommendations for analysis of variability of heart rate and BP.24
Recording protocol
BP measurements with the Finometer21 were calibrated for each patient by compressive sphygmomanometry. The pressure sensor (thimble) was secured on the middle finger and the PV sensor on the index finger, both in the left hand, with the arm resting on a sling to reduce hand movements. The first recording started after five minutes on supine position, and lasted 15 minutes. Then the patient changed to active orthostatism. The second recording started after five minutes of position change and lasted 15 minutes. All recordings were obtained between 11:00 am and 1:00 pm, and participants were instructed to breath normally at all recording times (spontaneous breathing).
Signal processing
BP and PV signals were analyzed with techniques implemented in Matlab (Mathworks®, Inc), as briefly described below.
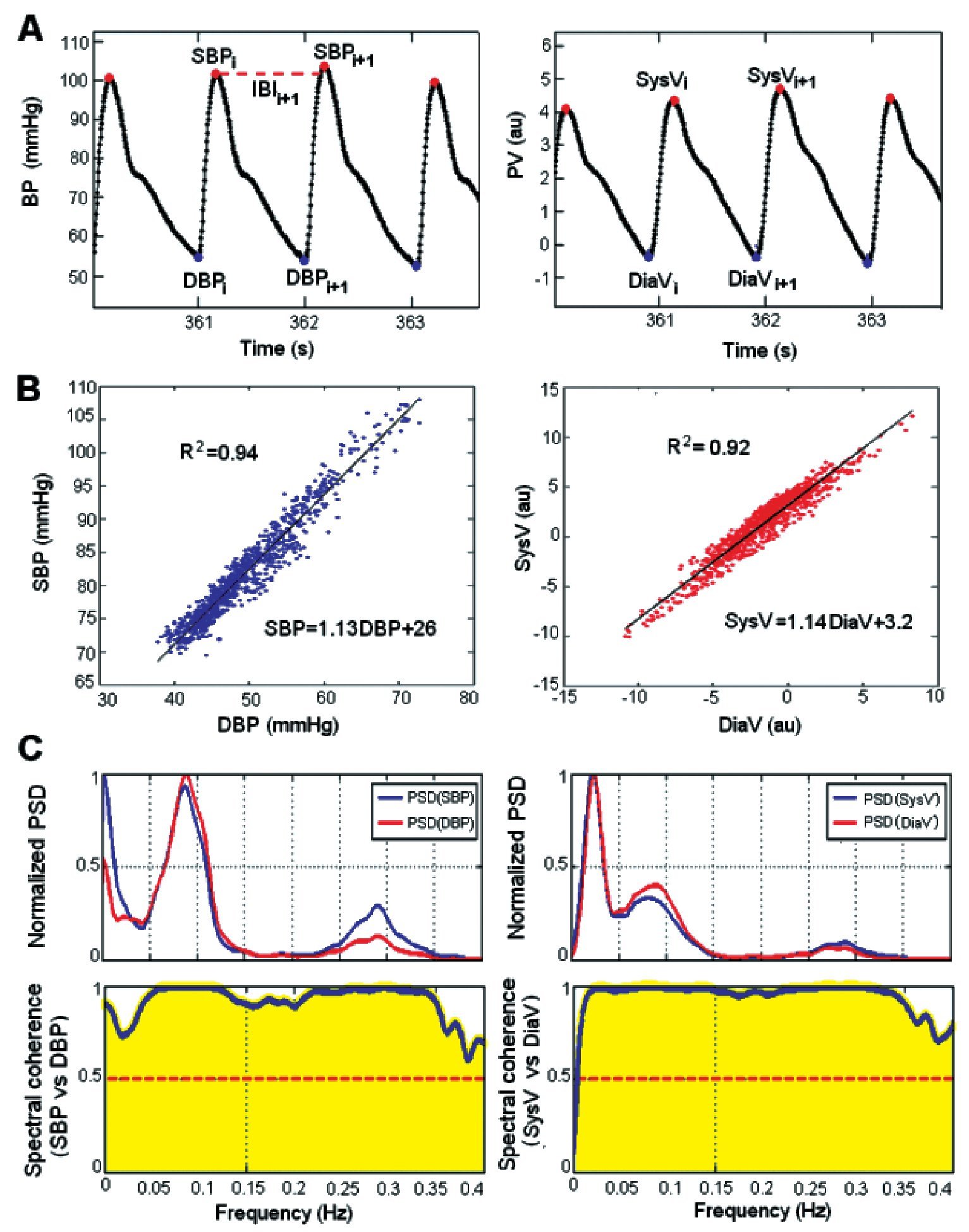
The first step was the identification of each heartbeat and its corresponding values of SBP, diastolic blood pressure (DBP), SysV, diastolic blood volume (DiaV) and IBI. The BP signal was filtered by a second derivative algorithm,25 it was rectified to positive values and a threshold was applied in order to find the peaks that correspond to SBP (Figure 2A). Correct identification of the SBP for all heartbeats was verified manually. Then, the minimum value between consecutive SBP values was measured to obtain the DBP. The PV signal was filtered with a moving average filter with bandwidth of 0.02 to 10Hz, in order to improve the signal quality for better identification of SysV and DiaV in each heartbeat. Filtering the PV signal did not affect the frequency band of interest for SysV and DiaV (known as low-frequency band, LF, from 0.04 to 0.15Hz).24,26 Then, the occurrence time for SBP and DBP of each heartbeat was used to locate the corresponding SysV and DiaV values from the PV signal. IBI was obtained by the time difference of SBP between consecutive heartbeats.
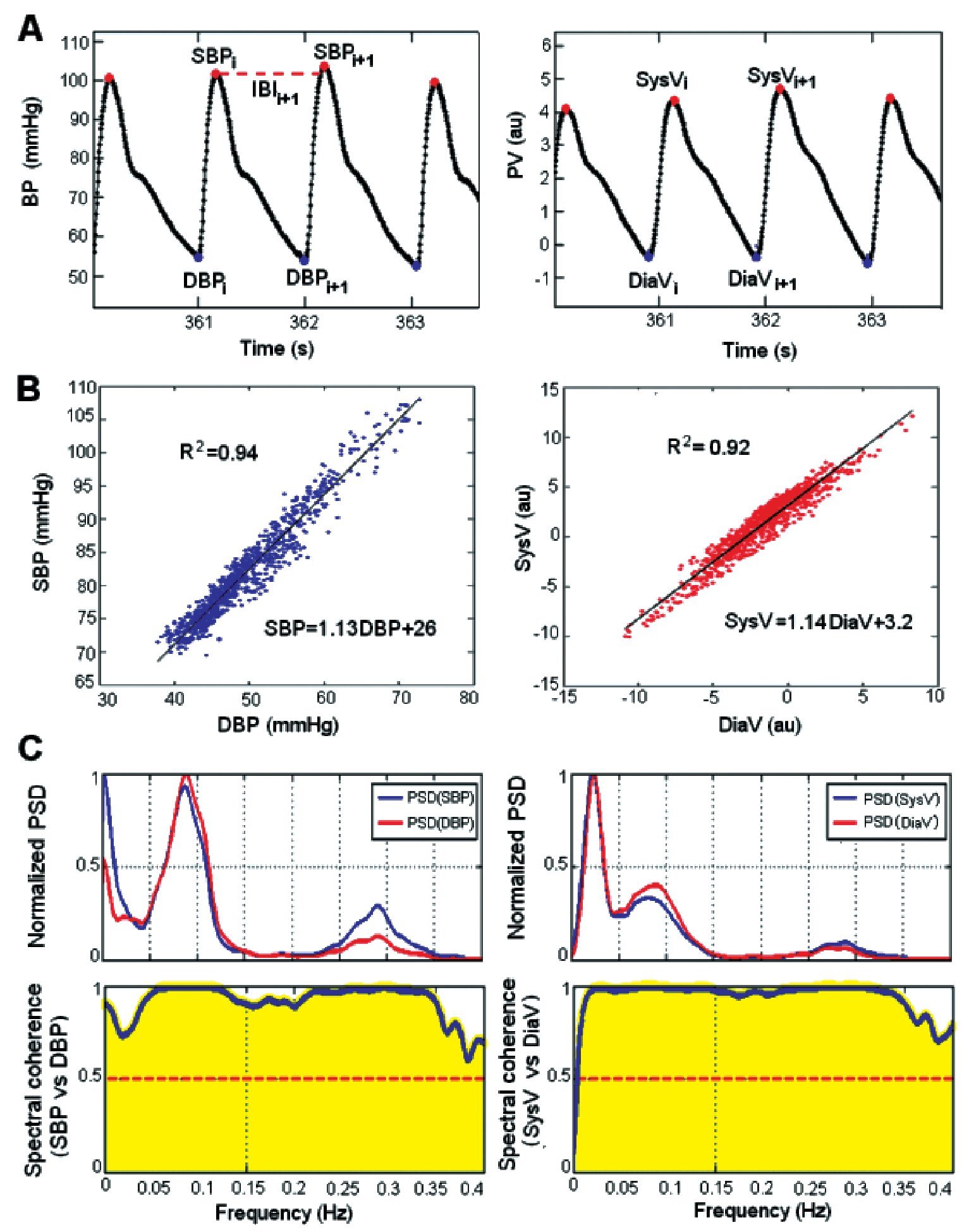
Figure 2.A) Measurement of systolic blood pressure (SBP), diastolic blood pressure (DBP), interbeat interval (IBI), systolic volume (SysV) and diastolic volume (DiaV) from a non-invasive recording of blood pressure (BP) and photopletismographic volume (PV). B) Example of linear regression analysis of systolic variables versus their corresponding diastolic variables, from one patient in supine position (R2 indicates the determination coefficient). C) Power spectrum density (PSD) of systolic and diastolic variables of the same example, and their corresponding spectral coherence spectra, a.u. = arbitrary units, i = number beat index.
The systolic variables (SBP and SysV) were compared against their corresponding diastolic variables (DBP and DiaV) by bivariate linear regression analysis. For each recording, the prediction equation of simple linear model and the determination coefficient (R2) was obtained using the least squares method27 and comparing the diastolic signals (x-axis or independent variable) versus the systolic signals (y-axis or predicted variable) (Figure 2B). The statistical significance (p) of each R was evaluated for each regression line according to the size of the recording.
The value of R was considered as statistically significant if p≤0.01, in this linear regression analysis.
In order to test the frequency range of the linear correlation between the systolic and diastolic variables, a spectral coherence analysis was performed. Since the sampling time all variables is not constant, they were re-sampled at 3 Hz to preserve their harmonics with frequencies up to 0.4 Hz.28 In order to maintain the same resolution in frequency (df) for all recordings, the systolic and diastolic re-sampled signals of BP and PV in supine position and orthostatism of each subject were cut-off to 2550 samples. Spectral leakage was decreased by fitting a straight line that was subtracted from the re-sampled signal. The power spectral density (PSD) of each patient was obtained by the Welch periodogram28 with a 50% overlap and a Hanning window of 300 points (i.e., window size of 100 s) (Figure 2C). The spectral coherence between diastolic and systolic signals of the BP and PV was calculated using Equation 1, where f is the frequency in Hertz, PSDxy denotes the crossed PSD between the diastolic signal (x) and the systolic signal (y), PSDx refers to the PSD of the diastolic signal (x), and PSDy is the PSD of the systolic signal (y).
Equation 1: Cxy(f) = |PSDxy(f)|2 / (PSDx(f) · PSDy(f))
A value of spectral coherence Cxy≥0.5 was considered significant, and this was considered of interest within the LF band because blood vessels have no parasympathetic innervations (Figure 2C).4,6,26,29
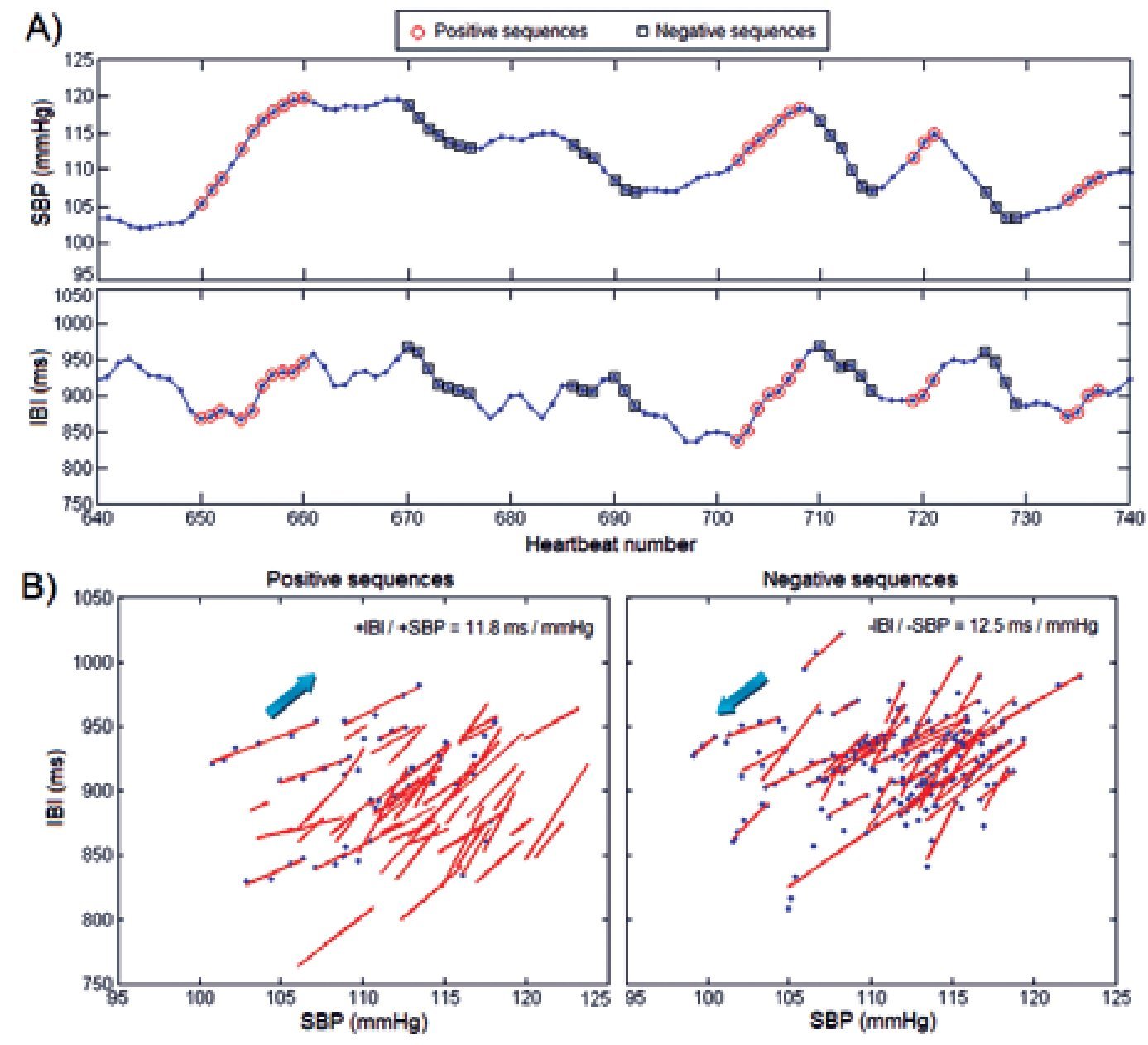
The baroreflex effect estimation was performed as follows. Considering that arteries receive only sympathetic innervations,4,29 and the spectral content of interest falls within the LF band,24 a low pass filter with moving average cut-off frequency of 0.15 Hz was applied to SBP, SysV and IBI. The number of points needed to filter each signal was calculated with the sampling rate (approximated by the average IBI) divided by the cut-off frequency (0.15 Hz). Using the sequences method, each sequence comprised data points where three or more consecutive beats increase or decrease in SBP and IBI concurrently (Figure 3).7,30 The sequences were plotted (IBI vs SBP), and the least squares method was applied to obtain the slope of the linear fit for each sequence (Figure 3). The baroreflex sensitivity was then estimated as the average of all slopes, either in a positive (+IBI/+SBP) or negative (-IBI/-SBP) direction. The same procedure was applied to SysV and IBI signals, obtaining the baroreflex effect on SysV as the averaged values of all positive sequences (+IBI/+SysV) and negative sequences (-IBI/-SysV).
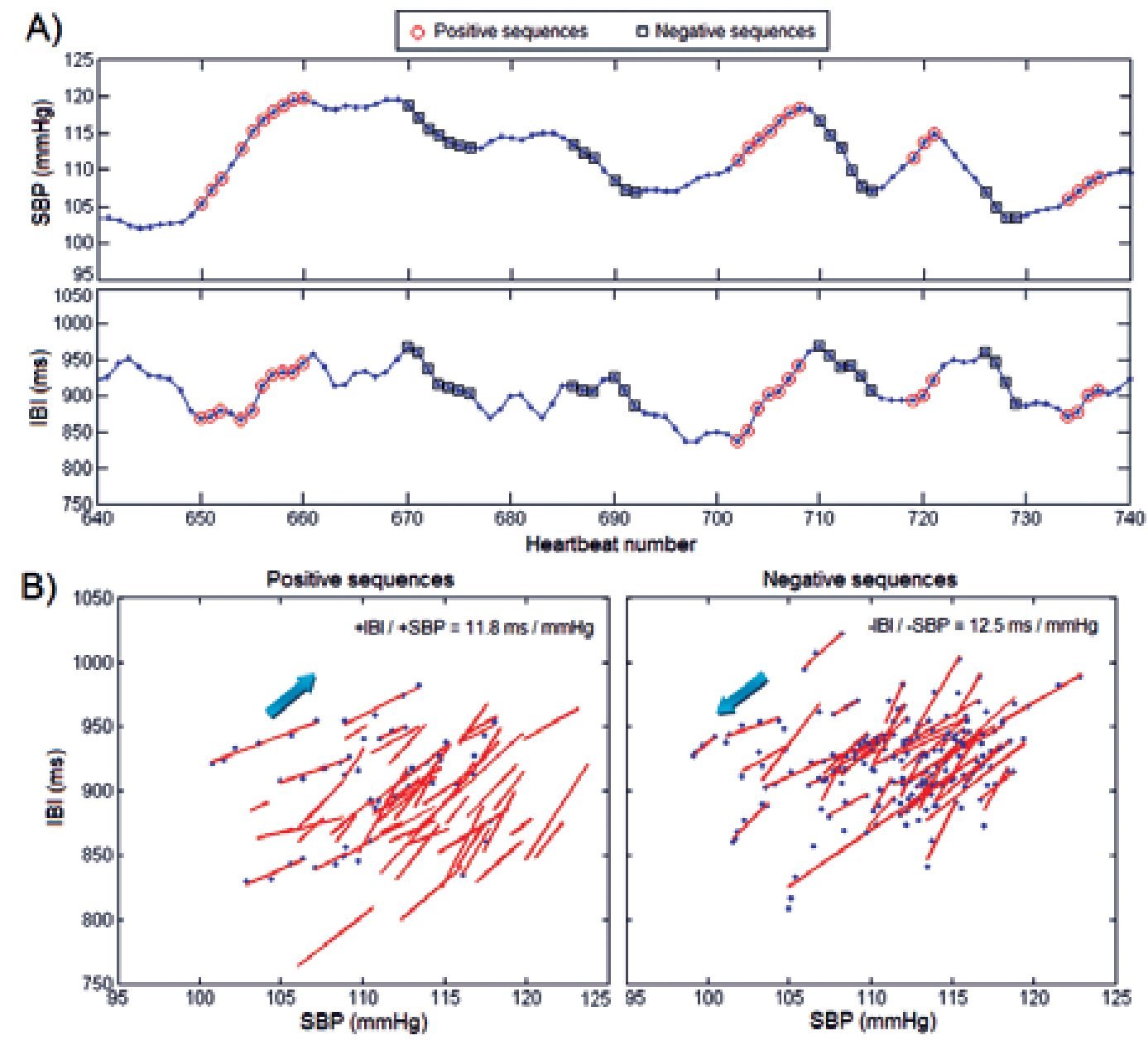
Figure 3. Baroreflex sensitivity analysis by the sequences method. A) Identification of sequences with concurrent change in SBP and IBI, positive sequences are indicated by circles and negative sequences are indicated by squares. B) Linear regression applied to each sequence allows estimation of the BRS index as the mean slope of all sequences. The calculation is performed separately for positive and negative sequences.
Statistical analysis
Results are given as mean ± standard deviation. Statistical analysis was performed using SPSS ver. 15 (StatSoft®, Inc.). Normal distributions of all variables were verified by Kolmogorov-Smirnov tests. The variables were compared by paired-t tests (supine position versus orthostatism). The linear correlation between the baroreflex sensitivity and the baroreflex effect on SysV was estimated by Pearson's correlation coefficient (R), considered statistically significant if p<0.05 and R>0.335 in each case (n=35).
Results
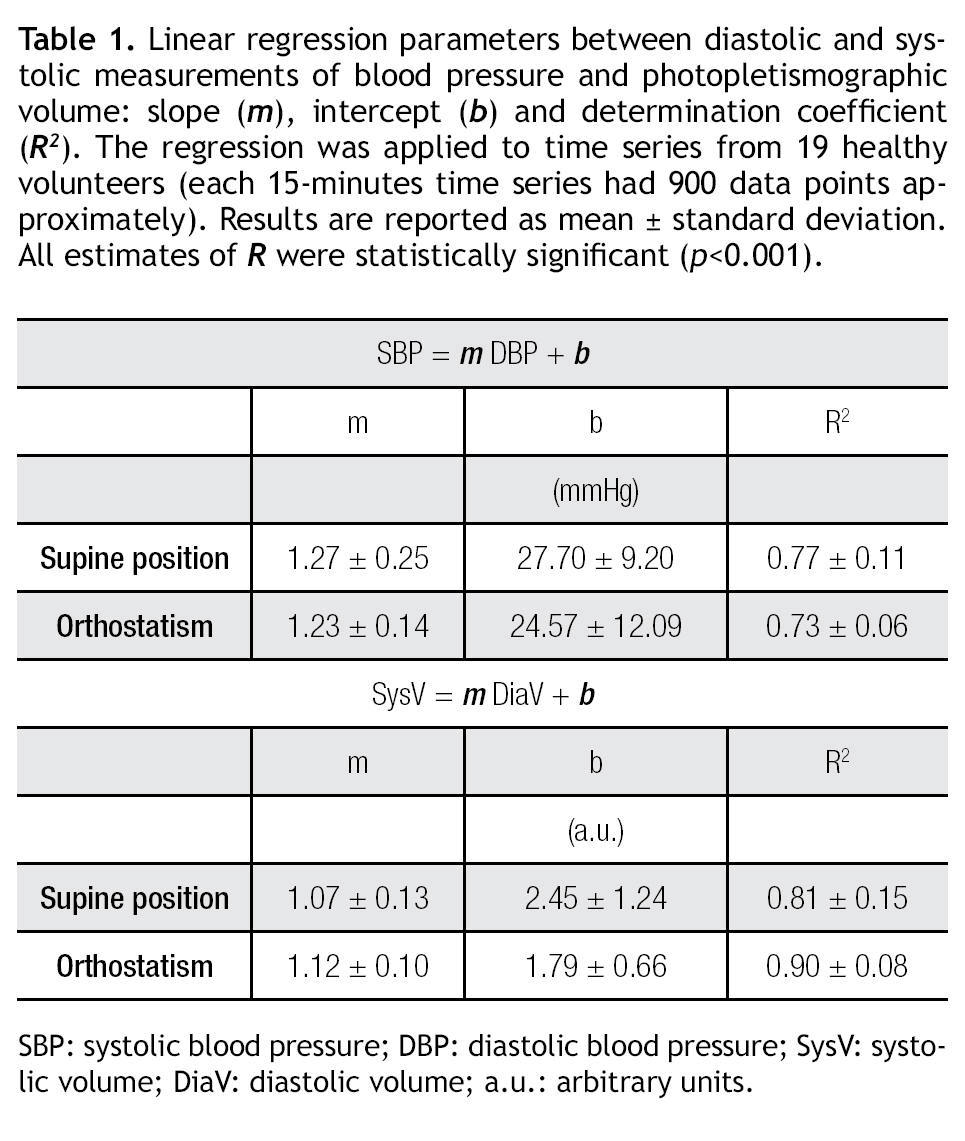
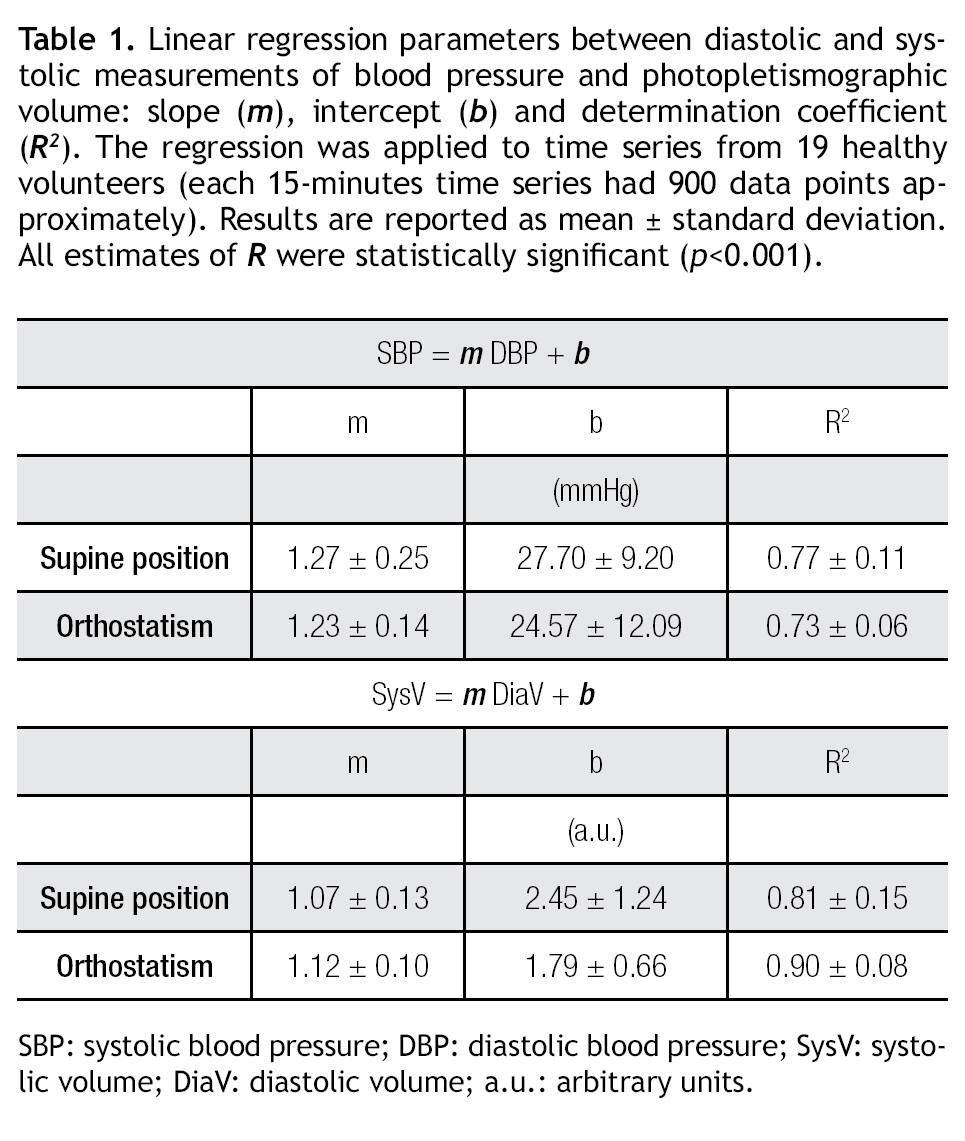
The results of the linear regression analysis between systolic and diastolic measurements are shown in Table 1. In all cases (n=19) the correlation coefficient (R) was statistically significant (p<0.001) according to the number of data for each signal (between 900 and 1200 data points), with R2>0.7. Therefore, a significant amount of DBP variation can be explained by SBP and also a significant amount of variation of DiaV can be explained by SysV.
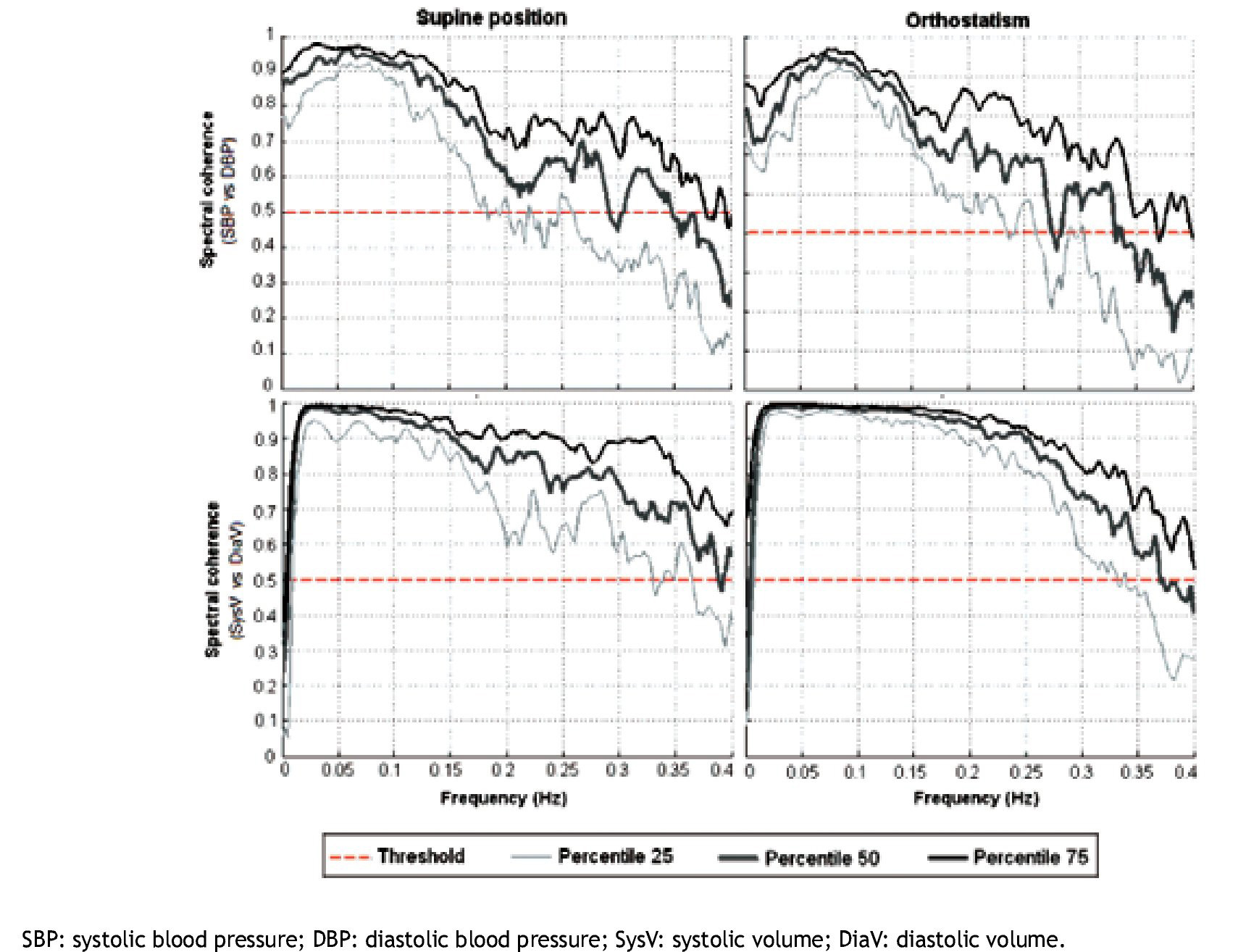
The spectral coherence analysis of diastolic versus systolic variables is summarized in Figure 4. From all cases, 15 subjects had a spectral coherence greater than 0.5 in the frequency band of interest (LF, 0.04 to 0.15 Hz), which confirms a strong linear association between the systolic and diastolic variables for each frequency within LF.
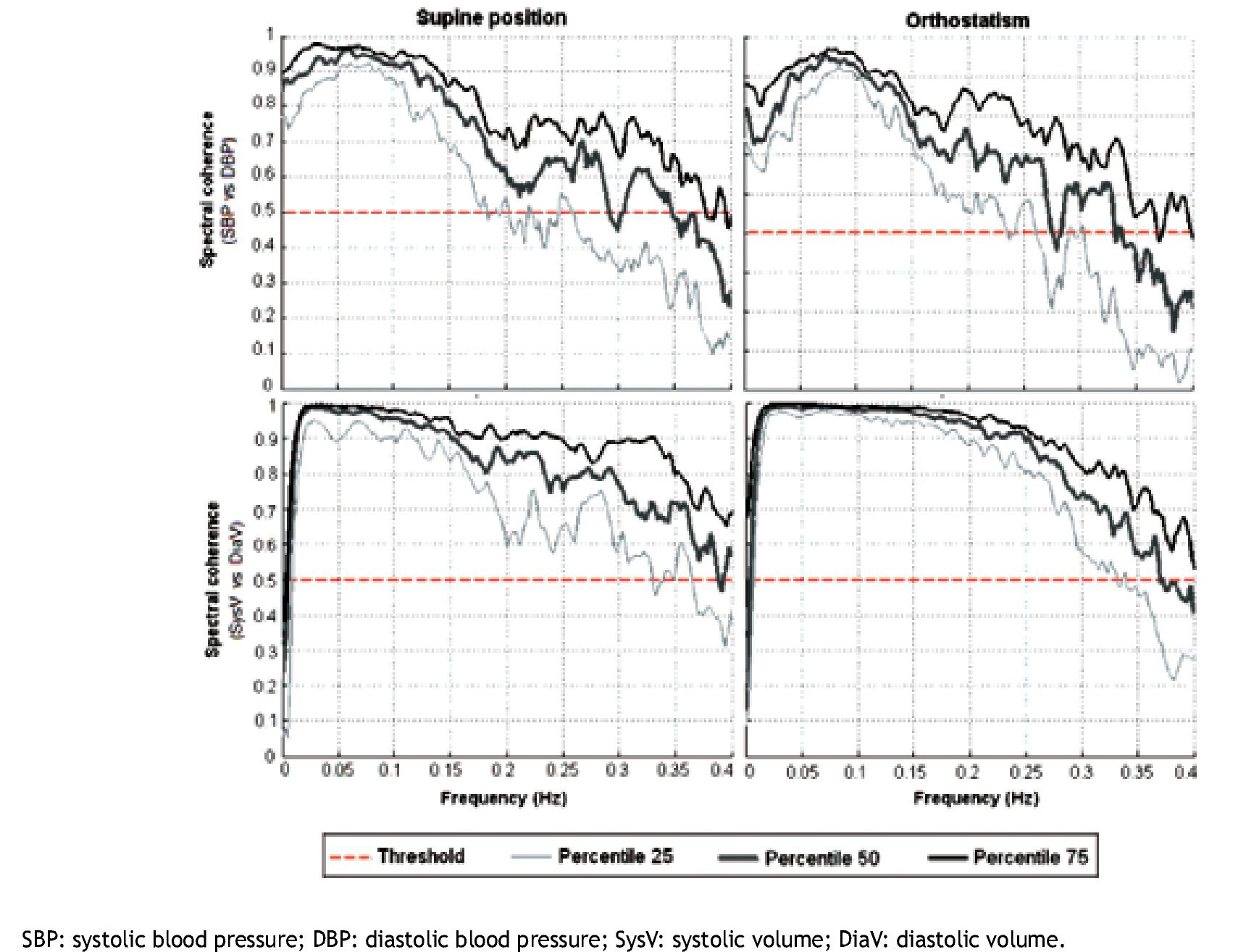
Figure 4. Results of the spectral coherence analysis. The lines correspond to percentiles 25, 50 and 75 of the systolic vs diastolic signals of blood pressure and photopletismographic volume from 19 healthy subjects.
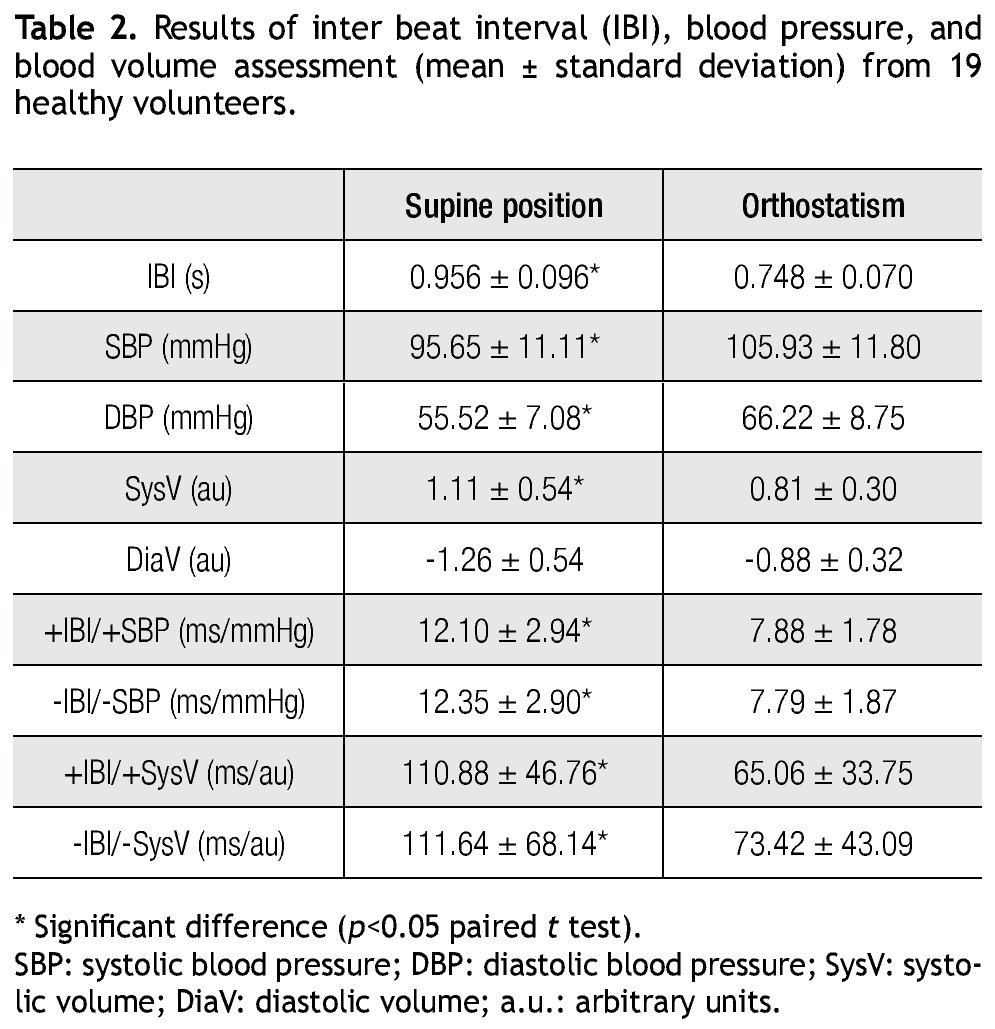
The effect of the orthostatic challenge on all evaluated variables is summarized in Table 2, including the baroreflex sensitivity index (i.e. IBI/SBP) and the estimated baroreflex effect upon PV (IBI/SysV). Compared to the supine position, orthostatism induced higher heart rate (i.e. shorter IBI), higher BP (both SBP and DBP), lower PV (both SysV and DiaV), lower baroreflex sensitivity and lower baroreflex effect upon PV.
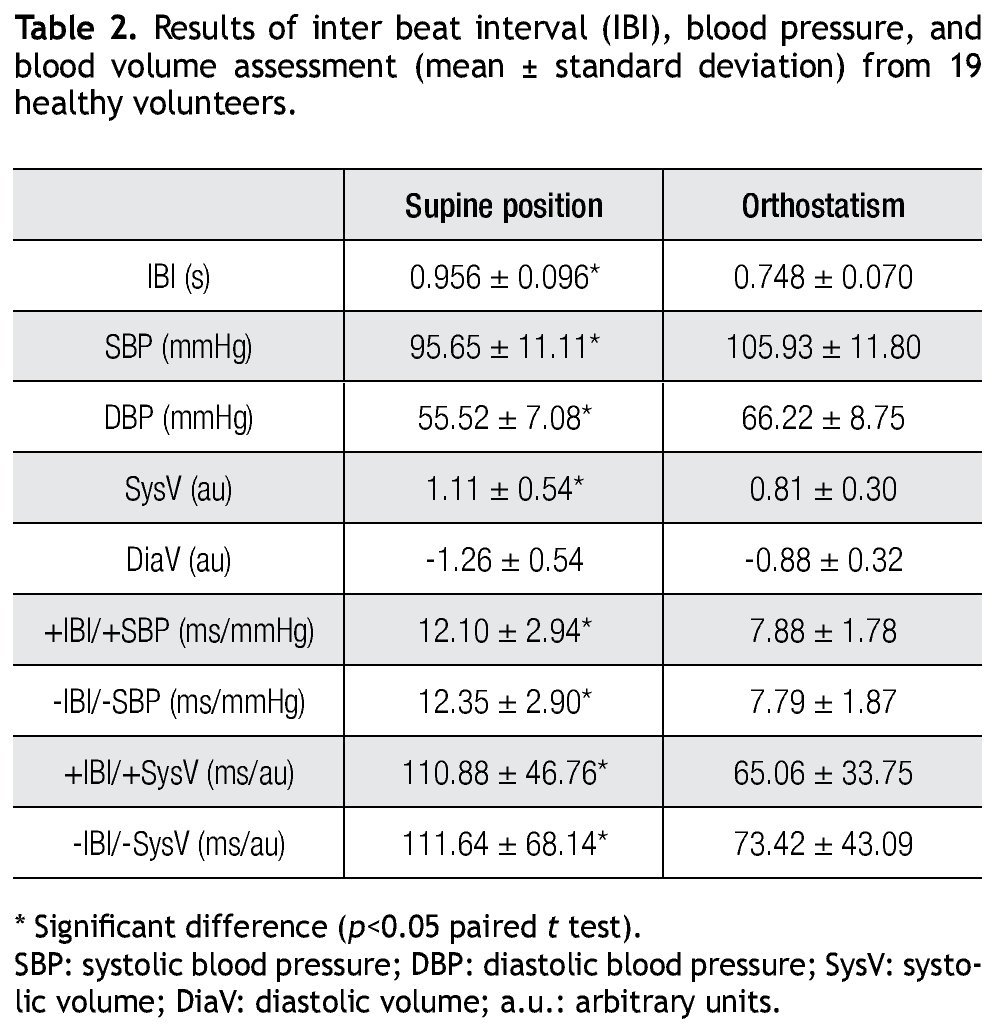
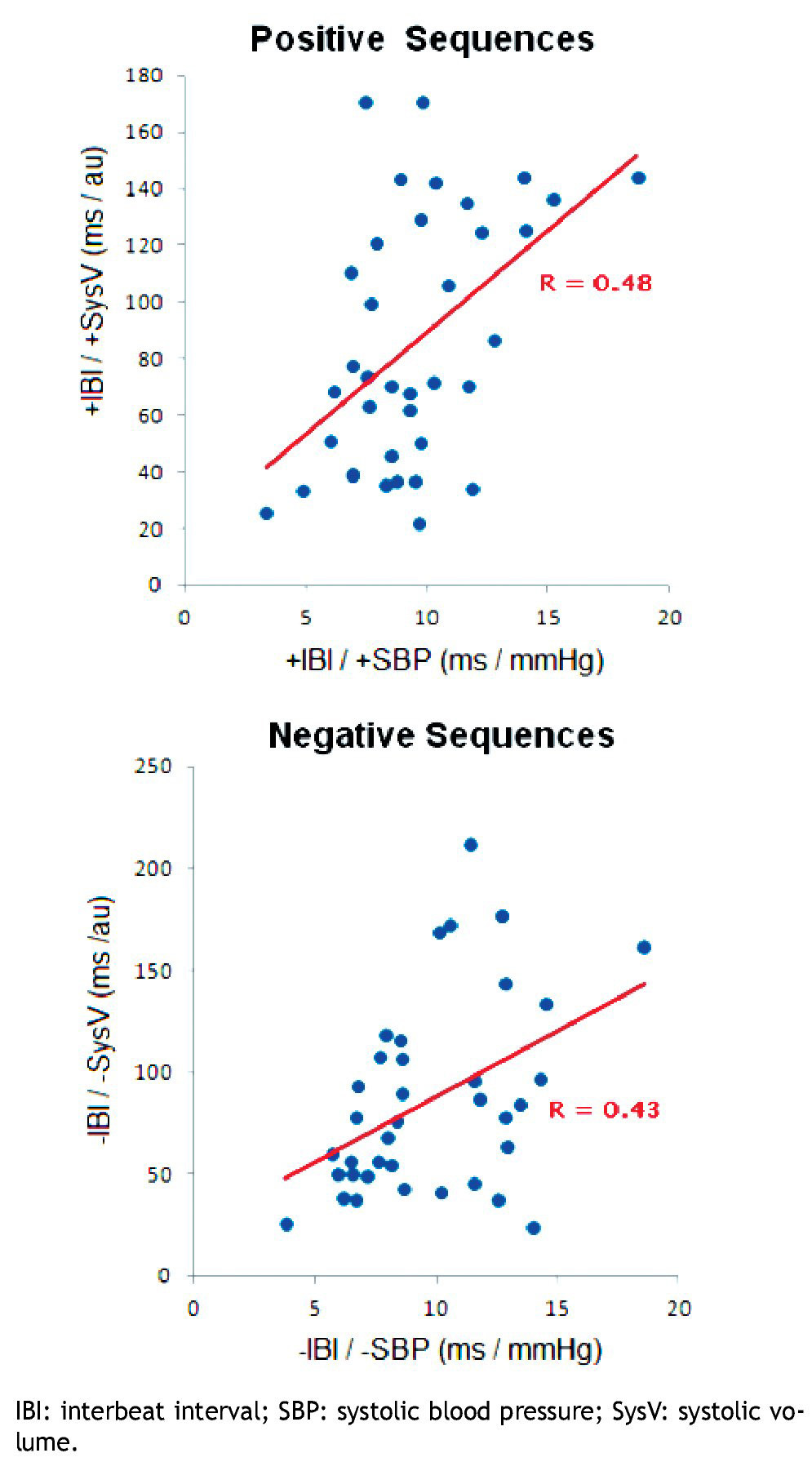
Figure 5 Shows the correlation coefficient (R) between the baroreflex sensitivity (IBI/SBP) and the baroreflex effect on SysV (IBI/SysV), for all subjects in supine position and orthostatism. In both type of sequences (positive and negative), a significant correlation between these two estimators was confirmed (p<0.05).
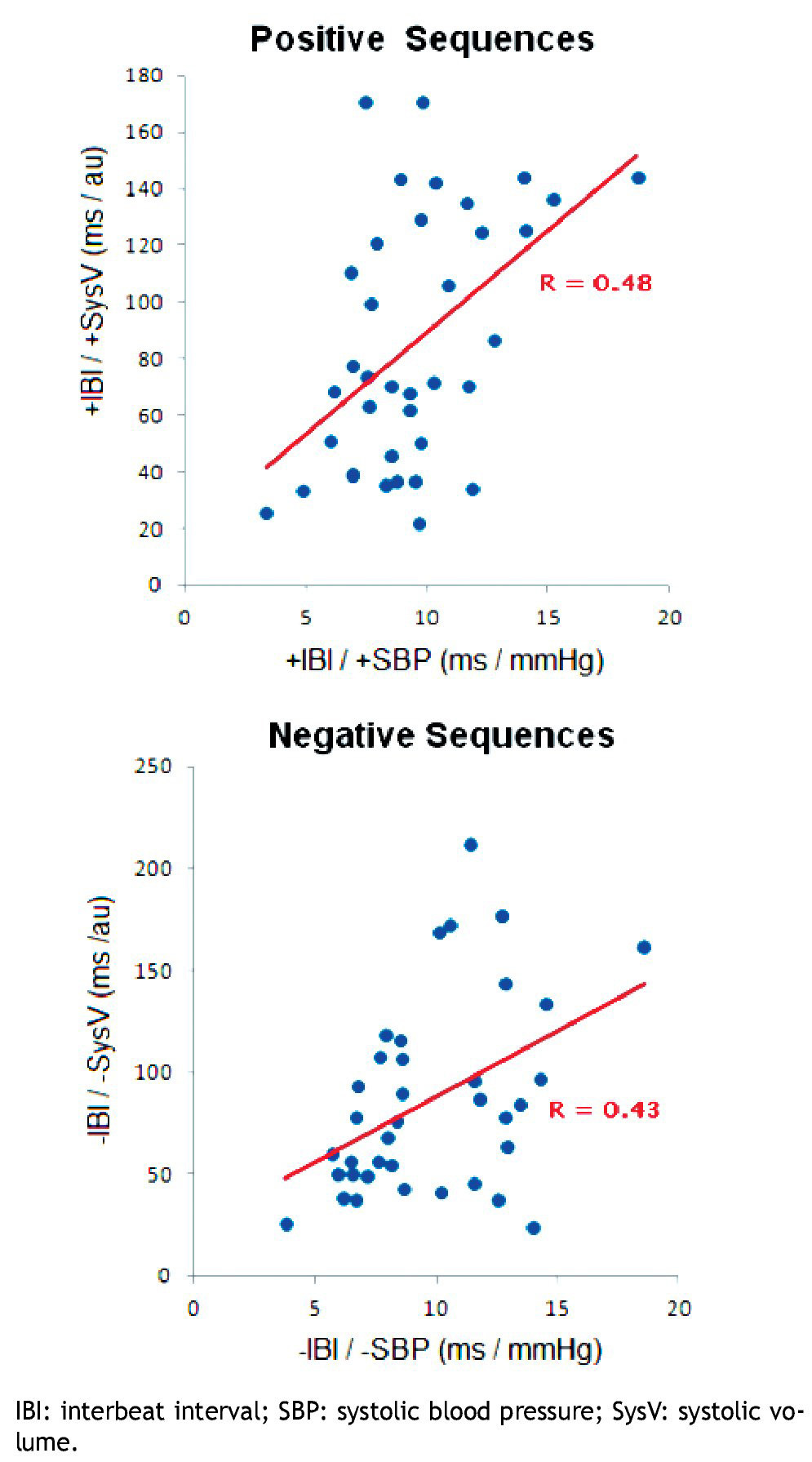
Figure 5. Linear correlation (R) of baroreflex sensitivity indexes estimated with the sequence method using the systolic blood pressure or the photopletismographic volume.
Discussion
Orthostatism is a common activity in daily life that represents an important challenge for the cardiovascular control system. Normal response to orthostatism includes decreased baroreflex sensitivity,30 which is attributed to vagal withdrawal and sympathetic activation towards the heart,4,6 and sympathetic activation towards blood vessels.31 Our results are concordant with those observations, and showed also that peripheral blood volume experiences important change due to orthostatism, manifested by a mean decreased of both SysV and DiaV (which has already been reported)31 and by a decreased baroreflex effect on blood volume (IBI/SysV index). Our results support the proposal that the correlation of changes in Sys and IBI are mediated by the sympathetic nervous system,8,32 since both variables were significantly coherent at all frequencies within the frequency band of 0.04 to 0.15 Hz. Nevertheless, non all changes in SysV and DiaV observed by photopletysmography should be ascribed to sympathetically modulated vasoconstriction or vasodilation. Many other factors (such as respiration, nitric oxide, endothelin, hormones, and the renin-angiontensinaldosteron sytem) could influence the variability of SysV and DiaV. Such factors could have local, regional or even central origin and some of them could be independent of the baroreflex mechanism. PV is a reflex of stroke volume, but its waveform and variability is conditioned by changes in the vessels properties (capacitance, inductance and resistance), which are dynamically affected by all mentioned factors including the sympathetic modulation. In this pilot study, none of these factors were controlled, which could explain the high dispersion within the indexes IBI/SBP and IBI/SysV (Figure 5). In spite of this, the current work demonstrated a significant linear correlation between these indexes.
Abnormal responses of the baroreflex reaction to orthostatism have been observed in patients prone to hypotension and syncope2 and in patients with hypertension either essential1,12 or secondary to chronic renal failure.15,16 In both extremes of abnormal BP, the main invoked culprit is the autonomic nervous system: syncope is preceded by increase of vagal tone and decrease of sympathetic activity (towards the heart, which produces bradycardia) and decreased sympathetic activity towards blood vessels2,8 (which decreases arterial resistance producing vasodilatation), while hypertension is associated to increased sympathetic activity both to the heart and blood vessels.12 Since variations of sympathetic activity to the arteries can cause significant changes in their blood volume, it is surprising that few studies have considered the variations in blood volume themselves as a key factor to explain the abnormal response to orthostatism31 and other stimuli such as hemorrhage,33 vasoconstriction induced by smoking,34 respiratory variations or apnea,35 local cold exposure,36 sympathetic blockade by epidural anaesthesia37 or even carotid baroreceptors denervation and thoracic sympathectomy.38 Although here we presented only the normal response of blood volume to one particular stimulus (orthostatism), we consider that this novel approach of estimation of the baroreflex effect on blood volume could be very relevant in further studies with different pathologies. The advantages of this approach include its non-invasiveness, the evaluation of the cardiovascular dynamics on a beat-to-beat basis, and the requirement of relatively short-time measurements.
Conclusions
The main contribution of this work is the evidence of a strong baroreflex effect upon the peripheral blood volume, which was more apparent during stimulation of the cardiovascular system with an orthostatic challenge. This approach could be clinically useful for the evaluation of blood volume regulation for many diseases such as diabetes mellitus and heart failure, and during therapeutic interventions such as hemodialysis.
Acknowledgements
The authors thank Brayans Becerra for the technical assistance during the recording of signals. During the development of this work, P. Martínez-García was supported by CONACyT with a scholarship for graduate studies (Masters Degree on Medical Physics).
Received on March 14, 2011; accepted on February 2, 2012.
Corresponding author:
Oscar Infante Vázquez.
Departament of Electromechanical Instrumentation,
Instituto Nacional de Cardiología Ignacio Chávez.
Juan Badiano # 1, Sección XVI, Tlalpan.
Z.P. 14080. Mexico City, Mexico.
Telephone: +52 (55) 5573 2911, ext 1386. Fax. +52 (55) 5573 0926.
E-mail address: infosc@cardiologia.org.mx