


Ventricular diverticula are rare entities whose incidence has been estimated in 0.013% of all congenital cardiopaties.1 They can originate in both ventricles.
The mechanisms that give rise to a congenital diverticulum have been widely discussed. It is believed by the failure of primitive mesoderm development in its somatic and splenic portions.2 The left ventricle diverticulum is more frequent. Right ventricle malformations are exceptional; if found they are situated in the outflow tract. They are associated to cardiac malformations.3
Complications of this anomaly are rupture (obstruction of the mouth of the diverticulum early in systole), peripheral embolism and heart failure. Surgical management consists of resection of the diverticulum either as an isolated operation or at the time of correction of accompanying malformations.1,4
We report the case of a one-month-old male patient. The aim of this case report is the rarity of the association of a right ventricle diverticulum and midline malformations and also because of its clinical behavior and evolution. Cardiovascular illness had been present in the patient since birth with a history of diaphoresis during feeding. Physical exploration showed cyanosis, SatO2 76%, rhythmic cardiac sounds and no significant murmurs, a unique second heart sound, and a supra-umbilical mid abdominal line defect with a soft pulsating purplish membrane measuring 2×3cm. The X-ray study showed situs solitus, left aortic arch, mild cardiomegaly, and a diminished vascular pulmonary pattern, no osteo-muscular defects were notice. The EKG study showed a sinus rhythm with an incomplete right bundle branch block, the presence of an electrical situs solitus, a QRS of −60°, an S1Q3 pattern and, in V1, a tight qs pattern with a positive T wave. Ecocardiography reported pulmonary atresia with a VSD, the right ventricular diverticulum was unnoticed because it is technically complicated to achieve adequate visualization of this defect by this method. Cardiac catheterization demonstrated systemic saturation of 50%, equalized pressures in both ventricles, pulmonary atresia, confluent pulmonary branches, sub-arterial VSD, a long and tortuous PDA with severe stenosis in the joining point with the left pulmonary branch and important hypoplasia of the pulmonary trunk and both pulmonary branches (Fig. 1a and b), McGoon index 1.2, Nakata index 145mm/m2. The presence of a ventricular diverticulum that drained into a sacular structure located in the abdominal region was also reported (Fig. 2a and b). The case was discussed in a medical session, and it was concluded that it was not eligible for surgical treatment because of the severe hypoplasia of the pulmonary trunk and its branches. It was also not suitable for placement of a stent in the PDA in the cath lab because of the morphology of the duct. In respect to ventricular diverticulum it was decided to observe it in the outpatient setting since the main reason of gravity and therefore the decision taking was the complex congenital heart disease. The patient is being followed up in the outpatient clinic.
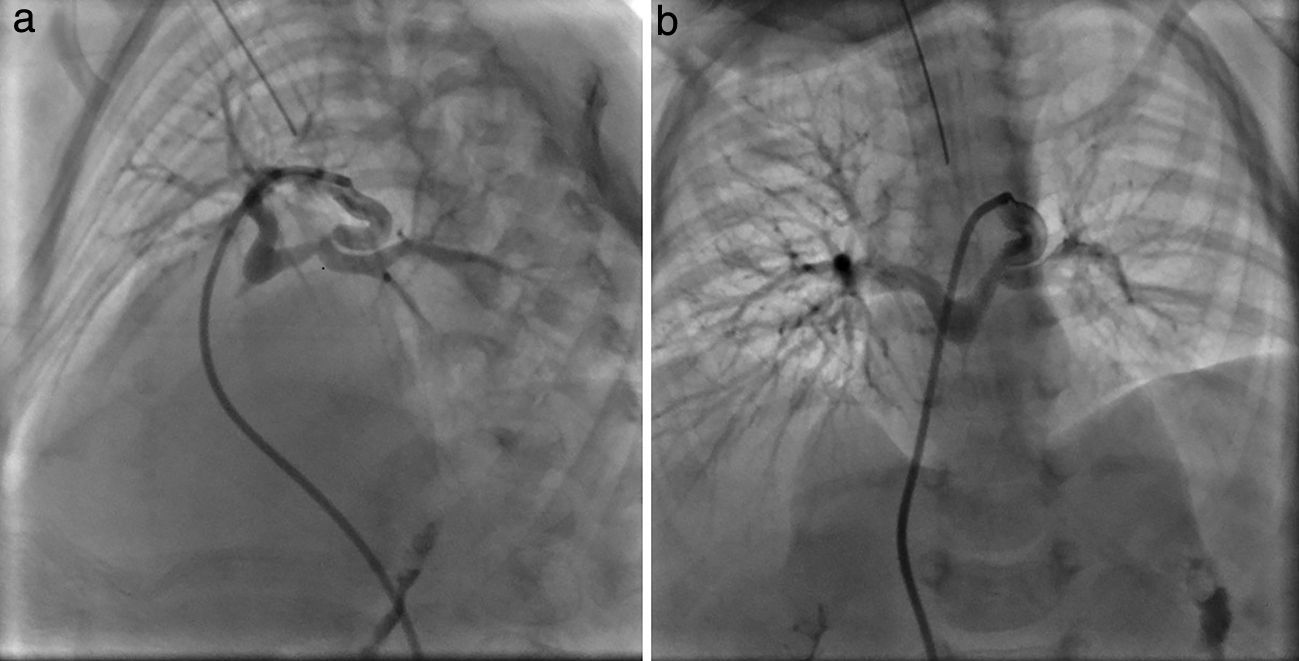
 LAO projection: selective angiography of a PDA can be seen; confluent pulmonary branches are perfused by the PDA. (b) PA projection: angiography in the PDA observing confluent and hypoplastic pulmonary branches with severe stenosis in the joining site with left pulmonary branch.")
(a) LAO projection: selective angiography of a PDA can be seen; confluent pulmonary branches are perfused by the PDA. (b) PA projection: angiography in the PDA observing confluent and hypoplastic pulmonary branches with severe stenosis in the joining site with left pulmonary branch.
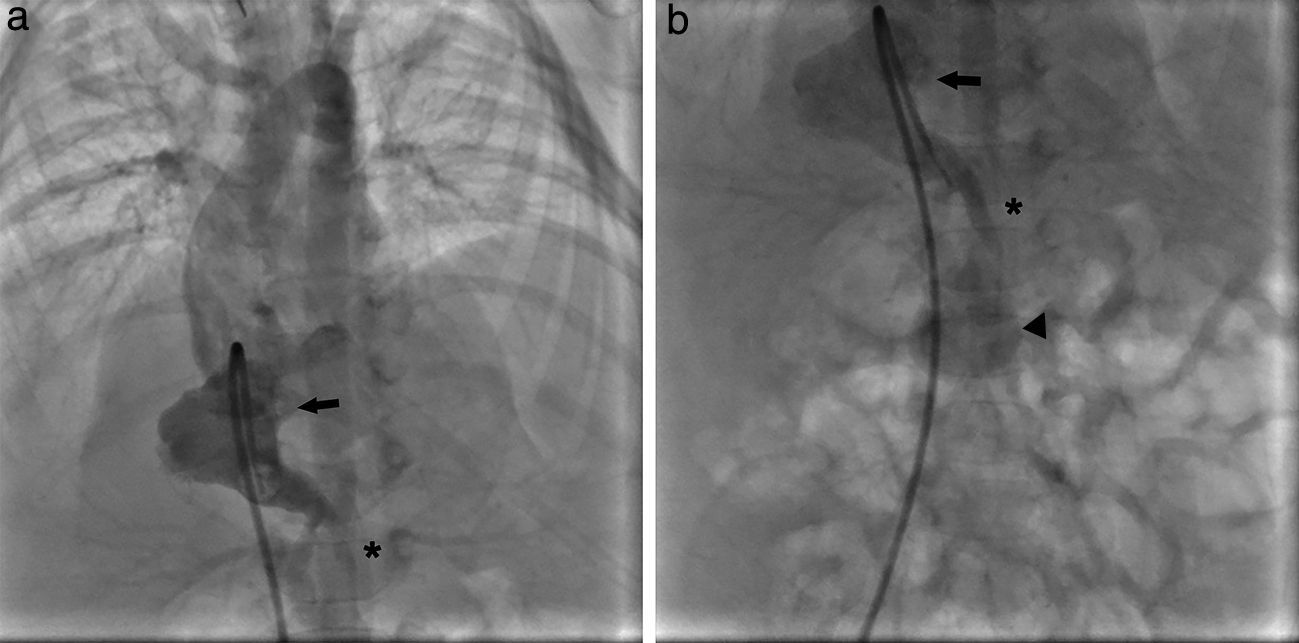
 PA projection: right ventriculography (arrow) observing the birth of a diverticulum (asterisk) from the apical part of this ventricle. (b) A diverticulum that drains in a secular structure (arrowhead) in the mid abdominal line region can be seen.")
Ventricular diverticula are small sacculations, described in the majority of cases as part of malformative syndromes. In 1958, Cantrell et al.5 were the first to refer to them describing the association between dextrocardia, congenital heart disease, pericardium defects and midline thoracic and abdominal malformations.
In the present case, alterations of the sternum, absence of the pericardium or diaphragmatic anomalies were not found. However, since the apical diverticulum drained to a structure at the level of the abdominal midline, a defect at the diaphragmatic level that allowed the communication from the thoracic to the abdominal cavity must have been present. We could not establish if there was a pericardic defect, however, it has been described that the pericardium that constitutes the diverticular wall can go along the same pathway as the cardiac layers and reach the umbilical region showing no defects.
In the case reported here, the diagnosis was made in the cath lab, where the presence of concordant systolic movement of the diverticulum and the saccular vascular structure with the rest of the right ventricular cavity was found. As it was previously commented, the presence of right ventricle diverticula is exceptional and hence the importance of reporting this case. Calderón et al.1 published six cases of cardiac congenital diverticulum, 66% originated from the right ventricle and were associated with congenital cardiopathy; their findings were similar to our case report. Less than 30 patients with right ventricle diverticulum have been reported worldwide.
The EKG in these patients usually shows a delay in the intraventricular conduction. However, in the case here shown there is a S1Q3 pattern in the electrocardiogram that might be interpreted as a dextro rotation of the heart. It has been previously reported that diverticula might cause a heart rotation to the right. We were also able to observe, in precordial V1, a tight qS pattern with the T wave that is also in accordance with a dextro rotated heart with right ventricular systolic overcharge. In aVR, there was also a smeared R wave that is in accordance with a His bundle right branch blockade. Nevertheless, this blockade was not observed in V1 probably because of the presence of a qS pattern that might be a consequence of a stroke or a non activating zone that might be masking the blockade in the His bundle.
The reported case is exceptional for its apical origin and its association to midline abdominal anomalies. Keeping track of these patients is cause of controversy and concern among authors. Little is known about the behavior of the diverticulum when it is present in the right ventricle. Therefore the indication of treatment in these patients must be standardized, being this it is surgical correction or only expectant management when presented with a complex congenital heart disease, as is the case of our patient. Patients with an isolated right ventricular diverticulum or in association with a simple heart disease, a surgical resection of it with total correction of the associated heart disease is possible. This should motivate to learn more about the behavior in terms of clinical presentation and outcome of these patients in order to obtain better results in the mid and long term.