


Primary congenital anomalies of the coronary arteries are rather rare with an incidence of 0.3–1.6%.1 Anomalous origin of the left circumflex (LCX) coronary artery from the right sinus of Valsalva is the most common congenital coronary variant, with prevalence at coronary angiography of 0.18–0.67%.2,3 Percutaneous coronary intervention (PCI) for an anomalous coronary artery is a technically challenging and complicated procedure. We report a very unusual case of an anomalous origin of a chronically occluded LCX artery arising directly from the right sinus of Valsalva that was successfully performed by transradial (TR) antegrade approach.
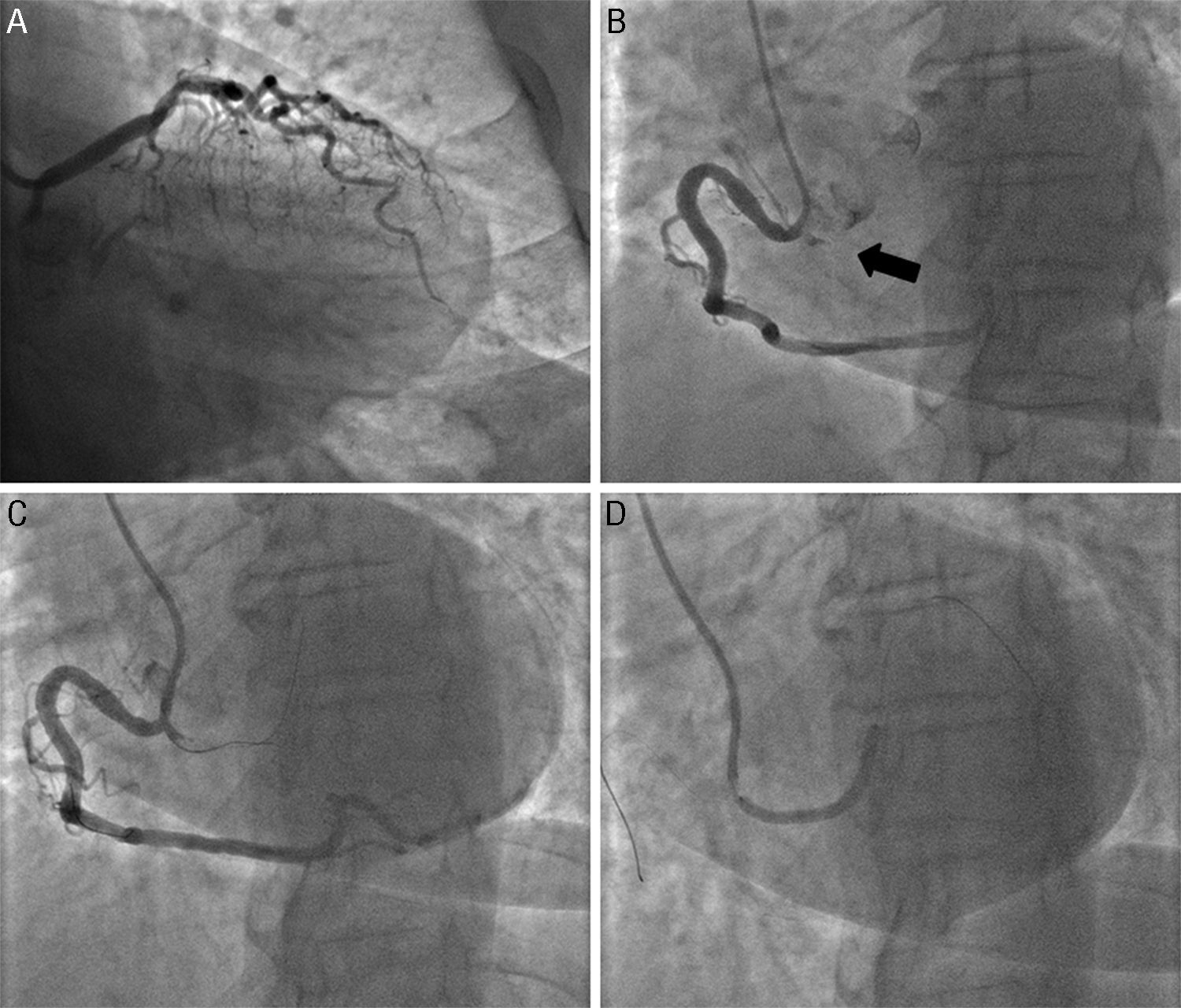
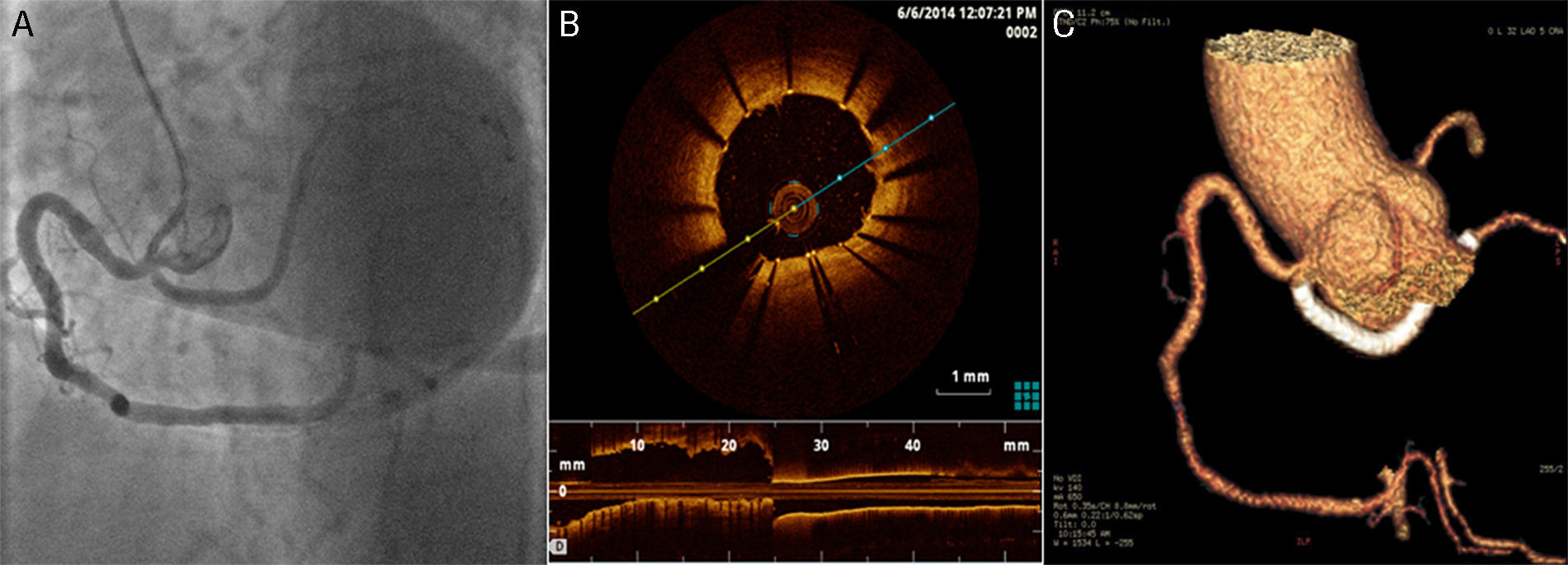
A 66-year-old female with a past medical history of hypertension presented with an 8-month history of exertional chest pain. An echocardiogram showed normal heart wall movement with normal left ventricular ejection fraction. She exercised for 8min on the standard Bruce protocol and experienced chest pain, and was found to have a 2-mm ST-segment depression in the inferolateral leads at the end of exercise. After obtaining an informed consent, coronary angiography revealed absence of the left main coronary artery, accompanied with the left anterior descending coronary artery without significant obstructive atherosclerotic lesions (Fig. 1A) and an anomalous origin of a proximal chronically occluded LCX artery from right sinus of Valsalva with a retro-aortic course with the right coronary artery (RCA) and the LCX sharing a common ostium (Fig. 1B). It was a tapered chronic total occlusion (CTO) in the proximal portion of the anomalous LCX with bending >45 degrees detected within the CTO segment and >20mm occlusion length (JCTO score=2).4 The CTO revascularization was performed from the right radial artery. Before the procedure, the patient was taking clopidogrel (75mg/day) and aspirin (100mg/day) and during the procedure, received anticoagulation with unfractionated heparin (70UI/kg) to achieve an activated clotting time of 250–300s. With a 6 Fr Amplatz right (AR) 1 guiding catheter we made a double-wire antegrade technique, involving placement of a separate Sion® wire (Asahi Intecc, Japan) into the RCA to anchor the guide, followed by wiring of the anomalous LCX with a Pilot® 150 wire (Abbott Vascular, Santa Clara, CA, USA) supported by a 1.0×10mm Falcon® CTO balloon (Invatec, Roncadelle, Italy). Next, we proceeded with the parallel wire technique with the use of a Pilot® 200 wire. This wire punctured the proximal cap at a different position and was easily advanced to the distal true lumen (Fig. 1C). The occlusion was predilated with a 2.0×20mm Emerge® semi-compliant balloon (Boston Scientific, Natick, MA,USA) restoring coronary blood flow. Finally, a 2.75×38mm Synergy® (Boston Scientific, Natick, MA, USA) bioabsorbable polymer drug-eluting stent was deployed (Fig. 1D) with a good angiographic result (Fig. 2A), which was confirmed by optical coherence tomography (Fig. 2B) and coronary computed tomography angiogram study after angioplasty (Fig. 2C).
 Baseline coronary angiography. The arrow indicates the anomalous origin of a chronically occluded left circumflex artery. (C) Percutaneous coronary intervention with the chronic total occlusion successfully crossed. (D) Synergy® stent implanted.")
 Final angiographic result. (B) Optical coherence tomography image showing good stent apposition. (C) Coronary computed tomography angiogram after angioplasty.")
To the best of our knowledge this is the first case presented of successful recanalization of a CTO in an anomalously arising LCX performed by TR antegrade approach. Anomalies of the origin and course of the LCX coronary artery are amongst the most frequently encountered. The anomalous LCX originates from the right coronary cusp, either directly, or as a branch from the RCA and courses behind the aorta to the left part of the atrioventricular sulcus, where it resumes its usual configuration. This anomaly is classified as benign since it is not known to predispose individuals to sudden cardiac death. However, some studies have proposed a higher incidence of atherosclerosis and myocardial infarction in the presence of this anomaly.5 Anomalies of the LCX artery pose several potential challenges to the interventional cardiologist. Selection of the appropriate equipment (guiding catheter/wire) assumes greater importance, ranging from successfully engaging the ostium of the anomalous coronary artery with adequate support to advance interventional devices and ultimately, concluding the procedure with minimal exposure to contrast agents and radiation. PCI on anomalous LCX vessels is technically feasible, with a high procedural success rate when performed by experienced operators.6 CTOs successful recanalization in patients with viable myocardium has been shown to reduce symptoms like angina decrease the need for surgery and improve survival.7 According to the standard practice of the majority of CTO-dedicated centers and operators, PCI on CTO are attempted using large guiding catheters and trans-femoral approach. The TR approach is a valuable alternative to trans-femoral approach, which has been shown to reduce vascular complications and possibly be associated to a better clinical outcome.8
Anomalous coronary arteries are rare and clinically significant. PCI for an anomalous coronary artery is a technically challenging and complicated procedure. We would like to emphasize the feasibility of a TR approach even for complex lesions such as the one in this patient.
FundingNone.
Conflict of interestsThe authors declare that there is no conflict of interests regarding the publication of this paper.