



Introducción: Con la actual epidemia de obesidad infantil se ha vuelto cada vez más impor- tante conocer los factores de riesgo y de protección contra la misma. La alimentación con leche materna se considera un factor protector contra la obesidad infantil; sin embargo, se desconoce el mecanismo responsable de este efecto. Una de las teorías actuales analiza el papel de hormonas que contiene la leche materna, de las cuales la principal es la adiponec- tina. Con base en esta teoría, se compararon los niveles de adiponectina en leche materna de madres con sobrepeso/obesidad y con peso normal, además de correlacionar estos niveles con la ganancia ponderal de sus infantes.
Métodos: Mediante ELISA se analizaron los niveles de adiponectina en 40 muestras de leche materna, 20 de mujeres con sobrepeso/obesidad y 20 de mujeres con peso normal.
Resultados: Los niveles de adiponectina en la leche materna de madres con sobrepeso/obesidad son menores que en la leche materna de madres con peso normal (p < 0.05). Al comparar la ganancia ponderal de los lactantes que consumían leche materna rica en adiponectina con la de aquellos que consumían leche materna baja en esta hormona, los primeros presentaron una menor ganancia ponderal que los segundos (p < 0.05).
Conclusiones: Existe una relación entre el índice de masa corporal (IMC) materno y los niveles de adiponectina en la leche materna, siendo estos más altos en las madres con un menor IMC. Existe una relación entre los niveles de adiponectina y la ganancia ponderal de los lactantes que la consumen: los lactantes que consumen leche materna con más adiponectina tienen una ganancia ponderal menor.
Background: Given the current epidemic of childhood obesity, it has become increasingly important to understand the risks and protective factors associated with this disease. Breastfeeding has been identified as a protective factor; however, the mechanism responsible has not been elucidated. One of the current theories analyzes the role of hormones in breast milk, with special emphasis on adiponectin. This study aims to compare adiponectin levels in breast milk of normal-weight mothers with those in breast milk of overweight/obese mothers as well as to correlate these levels with the infant’s weight gain.
Methods: Forty samples of breast milk were analyzed for adiponectin levels using ELISA, 20 from mothers with normal weight and 20 from overweight/obese mothers.
Results: Adiponectin levels were lower in breast milk obtained from overweight/obese mothers than in breast milk from normal-weight mothers (p <0.05). When comparing infant weight gain, those fed with breast milk containing higher concentrations of adiponectin had a lower weight gain than those fed with breast milk containing low levels of this hormone (p <0.05).
Conclusions: There is a strong negative correlation between mothers’ BMI and adiponectin levels in breast milk. Mothers with a higher BMI had lower adiponectin levels in their breast milk. There is also a negative relationship between adiponectin levels in breast milk and weight gain of breastfed infants. Infants breastfed with adiponectin-rich breast milk had a lower weight gain.
1. Introduction
The current epidemic in childhood obesity highlights the importance of determining the risk factors that lead to the disease as well as the preventive factors. Breastfeeding during infancy is considered to be a protective factor against childhood obesity. For this reason, current recommendations from the American Academy of Pediatrics (AAP)1 regarding feeding with breast milk emphasize that it should be exclusive during the first 6 months of life and that it should be subsequently supplemented with other foods until the child reaches 1 year of age. Breastfeeding is not indicated after 1 year of age although it may continue if the mother so desires. This recommendation is based on the fact that it has been demonstrated that feeding with breast milk not only provides the fundamental nutrients for growth and development of the infant, but that it also provides protection against various diseases such as obesity. Breastfeeding has been studied as a protective factor against obesity, both during the breastfeeding period per se as well as during childhood and adulthood.
The role of breastfeeding as a protective factor against obesity has been reported since 1981 when M.S. Kramer analyzed the relationship between maternal breastfeeding and the delay in weaning with obesity.2 In this study, a lower risk was observed for this disease in adolescents who had been fed breast milk during their first months of life and that the risk was inversely proportional to the length of time of lactation. After the Kramer publication, other groups continued with this line of investigation and, in 2007, the WHO published a series of meta-analyses of the evidence up to that time.3 Those publications, which included 33 studies published between 1981 and 2007, analyzed the effect of maternal breastfeeding on blood pressure, development of diabetes and associated indicators including overweight and obesity. The findings generated in regard to overweight and obesity determined that feeding with breast milk confers a protective effect against the development of these conditions in advanced ages even when results are adjusted detracting factors such as socioeconomic status.
Despite the extensive documentation of the protective role breastfeeding plays against the development of obesity, the mechanism responsible has not yet been determined. In recent years, the theory of a phenomenon called “nutritional programming”4 has been proposed, indicating that breast-feeding provides the newborn with behavioral, neurological, caloric and hormonal stimuli that allow the development of protective mechanisms against adult obesity. In regard to hormonal stimuli, it posits that breast milk, in addition to containing nutrients, is comprised of hormones involved in the regulation of caloric balance in the newborn. In the long term, this generates a hormonal stimulus that programs the manner in which the calories consumed will be used during the remainder of the person’s life. Among the hormones previously mentioned, it is believed that those with the greatest impact in nutritional programming are called adipokines5, a group of hormones secreted by adipocytes and include leptin, ghrelin, resistin, obestatin and adiponectin. The latter has been identified as the adipokine with the highest concentration, both in the serum as well as in the breast milk and is believed to have the greatest influence in this process.
Adiponectin was discovered by Scherer et al. in 1995. Since then, multiple functional and physiological effects have been demonstrated.6 Currently, its effect on the regulation of lipid and glucose metabolism, its role in fetal development and its anti-inflammatory and anti-teratogenic properties stand out. Serum concentrations of this hormone are found inversely related to the degree of adiposity and directly associated with insulin sensitivity.7 Therefore, the serum concentration in adults and adolescents8 with obesity and T2DM is decreased. On the other hand, it has been observed that adiponectin levels in umbilical cord blood are much higher than those found in the serum of adolescents and adults. These concentrations have been directly associated with birth weight9 and with the newborn’s adiposity10 and inversely with weight gain in the first 6 months of life and with the degree of adiposity at 3 years of life.11
Prior investigations have shown that maternal adiposity has a positive association with adiponectin levels, which decrease with the time of breastfeeding. A possible explanation for this finding is the existing relationship between adiponectin, prolactin and adiposity. Adiponectin is negatively regulated by prolactin, but it has been observed that secretion of prolactin is decreased in obese women.12 The consequent decrease in negative regulation in these women could increase the concentration of adiponectin produced locally by breast adipose tissue and then secreted in the maternal milk.13
In the study published by Newburg et al. in 2010, a directly proportional relationship was found between adiponectin levels in breast milk and adiponectin levels in serum of infants.14 This finding indicated that adiponectin is absorbed by the AdipoR1 and AdipoR2 receptors present in the human intestine. Likewise, an inversely proportional relationship was found between adiponectin levels in breast milk and adiposity (weight/height ratio) of the infant. These infants were subsequently evaluated in 2012 by Woo et al. who found that the weight gain during the second year of life was positively associated with the exposure to adiponectin in maternal milk, independent of the birth weight or weight gain in the first 6 months of life.15 This tendency was also tested by Weyerman et al. in 2007.16
Studies by both Woo et al. and Weyermann et al. suggest that the adiponectin present in breast milk could have different effects during and after the period of active breast-feeding. One possible explanation is that adiponectin levels in breast milk appear to be directly related with maternal BMI, although these results have not been consistent and more information is needed in this regard. Taking this into account, it is possible to state that the exposure to high levels of adiponectin during breastfeeding is equivalent to being the child of an obese mother, which can indirectly affect weight gain in this child. Another alternative could be that the adiponectin contained in mother’s milk exercises its protective metabolic effects against obesity during active breastfeeding, but when consumption is stopped, the metabolic effect is not preserved. A third proposal is that the weight gain observed in children exposed to high adiponectin levels in maternal milk is not pathological but adaptive (due to the lower weight gain during the first 6 months of life) because previous studies found that weight gain during this period of life takes place at the expense of fatty tissue and then lean tissue.17 Considering the above, it is possible that a lower weight gain in infants exposed to high levels of adiponectin indicates a lower accumulation of fatty tissue.
In the present study it was determined whether there was a relationship between maternal BMI and adiponectin levels present in breast milk, as well as the type of relationship that exists between adiponectin levels in breast milk with infant weight gain.
2. Methods
To achieve the aforementioned objective, after review and acceptance by the Ethics Committee of the School of Medicine of the Institute of Technology and Higher Studies of Monterrey, Campus Monterrey, and the Ethics Committee of the High Specialty Maternal/Infant Regional Hospital, a group of lactating mothers was recruited. Mothers were recruited from the outpatient area of the High Specialty Maternal/Infant Regional Hospital and in the Urban Health Center San Angel in the state of Nuevo Leon and whose infants were between 4 and 8 weeks of age. The following formula was used for estimating the difference of the median in the two groups:

where n = size of the sample; Zα = level of significance (level of significance of 95% was used, Zα = 1.96); σ = amplitude or standard deviation (obtained using the values described by Weyerman et al. where σ1 = 10.4 y σ2 = 12.1); d = interval of amplitude or absolute precision.
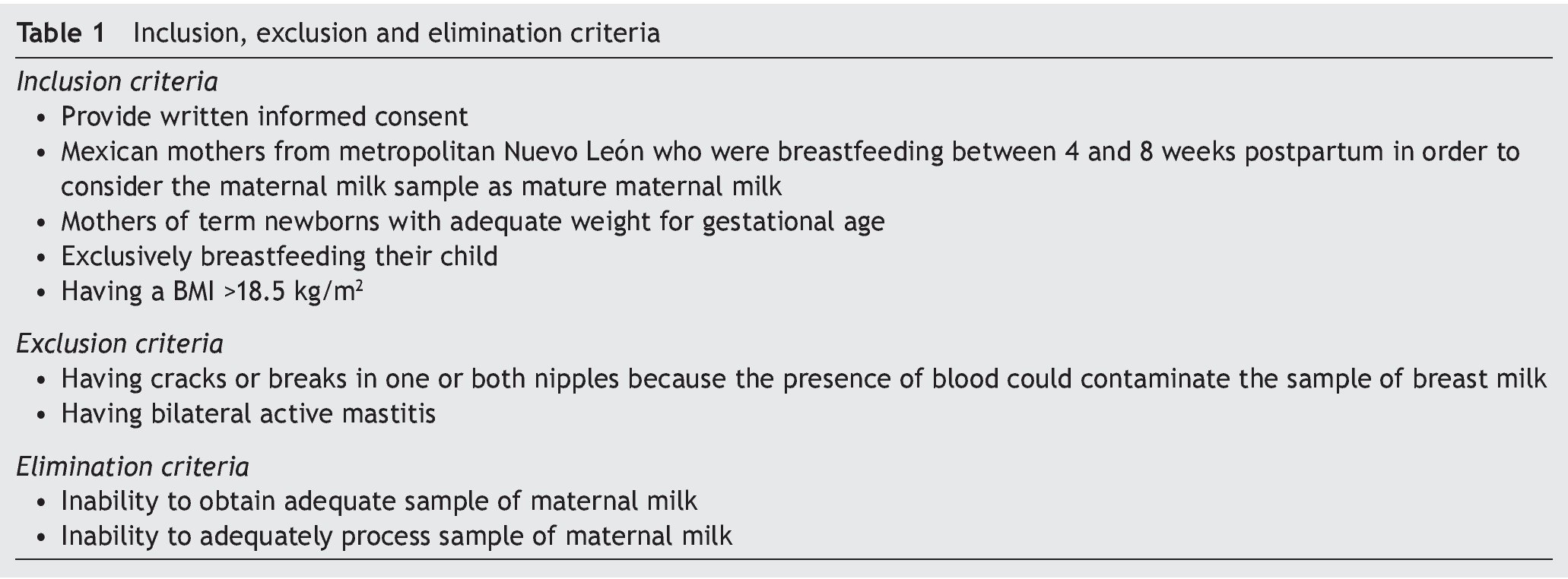
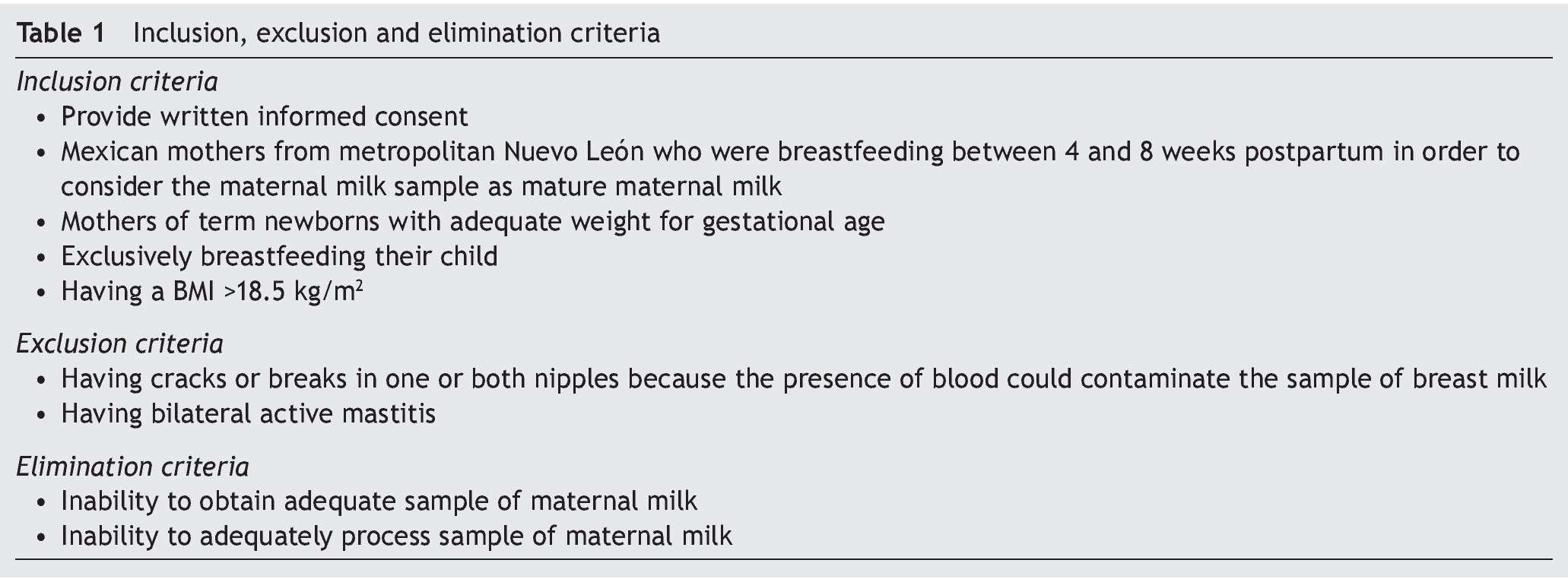
In total there were 40 subjects included and separated into two groups. The first group included 20 normal-weight mothers. The second group included 20 mothers with over-weight/obesity. Inclusion and exclusion criteria are shown in Table 1.
Once selected, an interview was held with each participant and each was asked to sign an informed consent. During this interview, information was gathered relevant to the mother’s and infant’s history. The required anthropomorphic measurements for the mother and the child were carried out. A sample of breast milk was obtained by manual expression at the start of the expression and at least 2 h after the last feeding from the maternal breast. Sample taking was done between 10 a.m. and 12 p.m. Samples were classified according to the mother’s body mass index (BMI) in accordance with the WHO criteria for evaluation of nutritional status. Those with BMI <25 kg/m2 were classified as “normal weight” and those with BMI >25 kg/m2 as “over-weight/obese”.
All samples were processed using the ELISA kit for adiponectin (Cat. DRP300 Quantikine® Human Total Adiponectin Immunoassay, R&D Systems, Minneapolis, MN) to obtain levels of adiponectin. Once the values were obtained they were recorded in a database in the IBM® SPSS Statistics® program to carry out statistical analysis. Hypothesis testing method was carried out based on the differences between means and expressed through specific mean difference with 95% confidence intervals. Once the two groups were formed, Shapiro-Wilks normality test was applied for each of the variables. For non-normally distributed variables, Mann-Whitney U non-parametric test was used and for those with normal distribution, Student t test was used. After these tests were applied, the null hypothesis was accepted for those with a value of p >0.05 and for the case with a p <0.05, the proposed null hypothesis was rejected. Descriptive statistics were evaluated using the IBM® SPSS Statistics® program.
3. Results
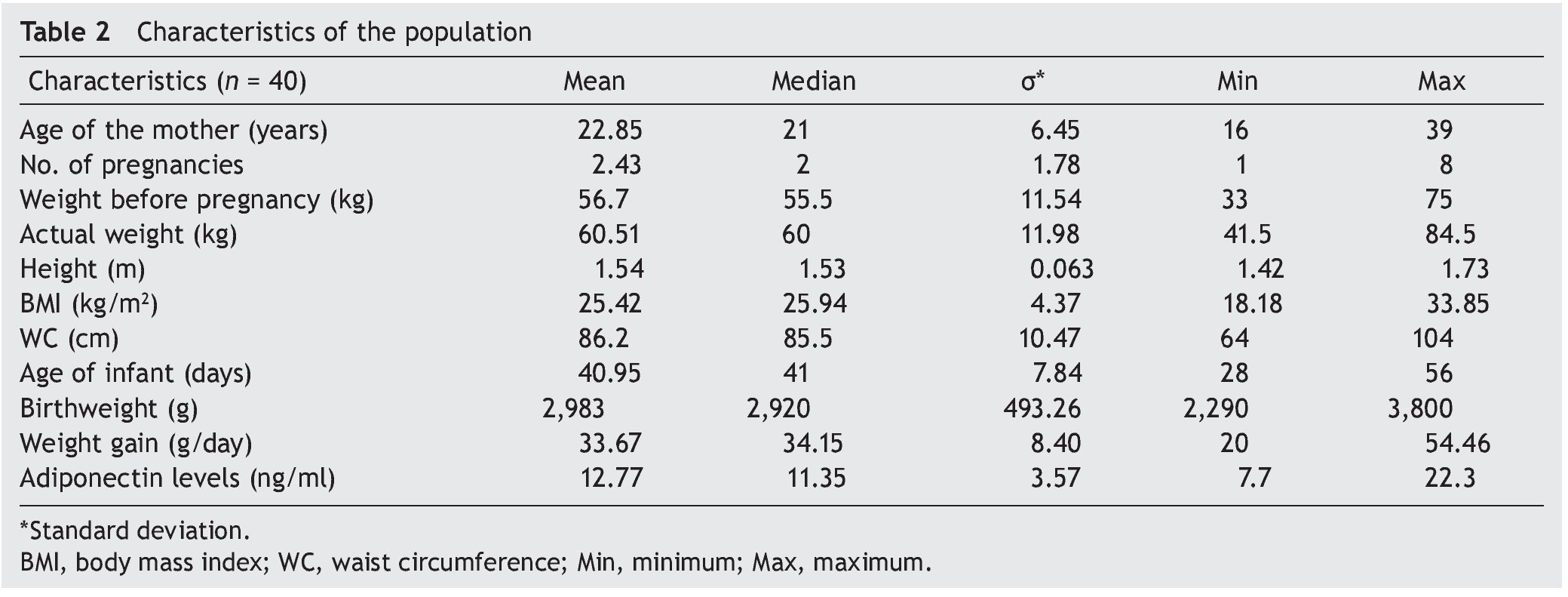
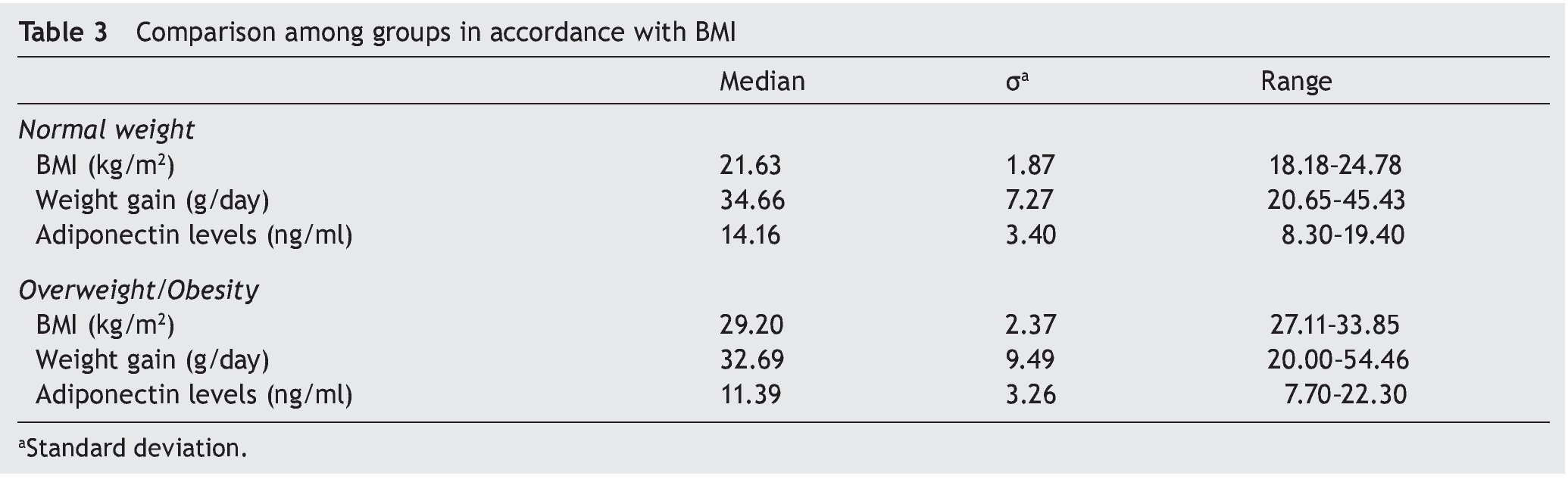
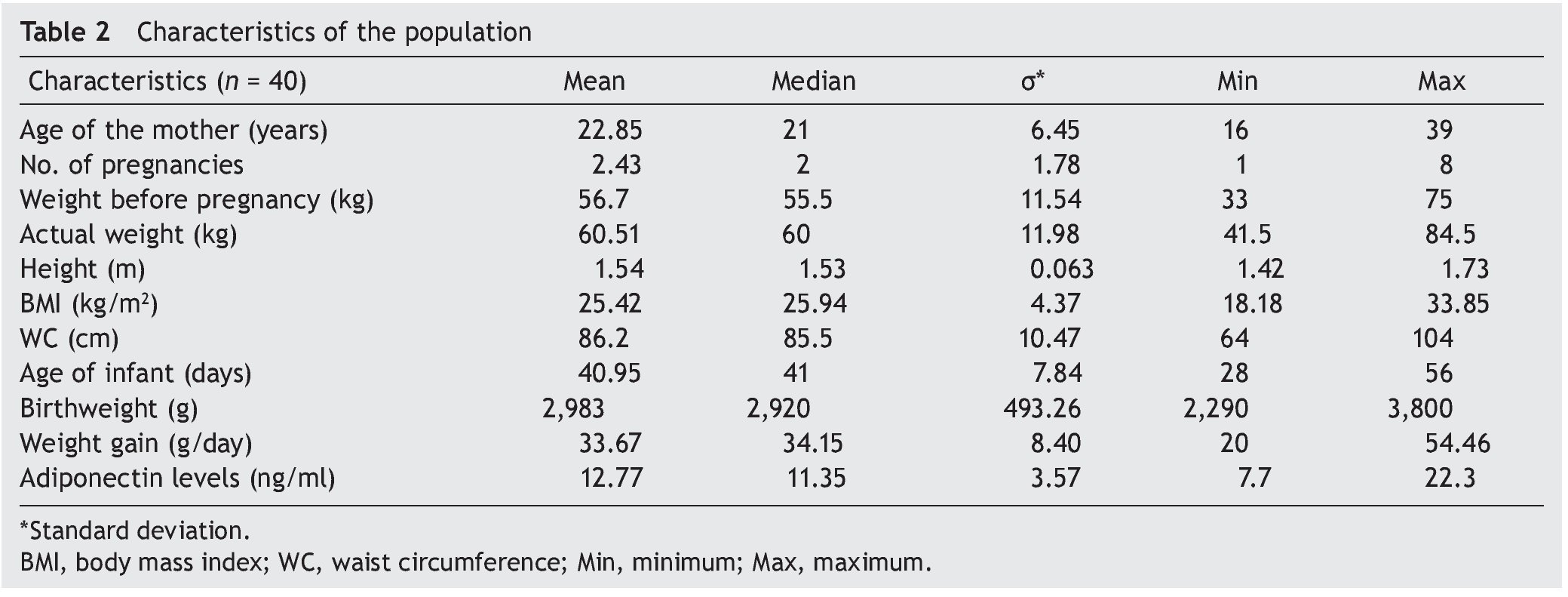
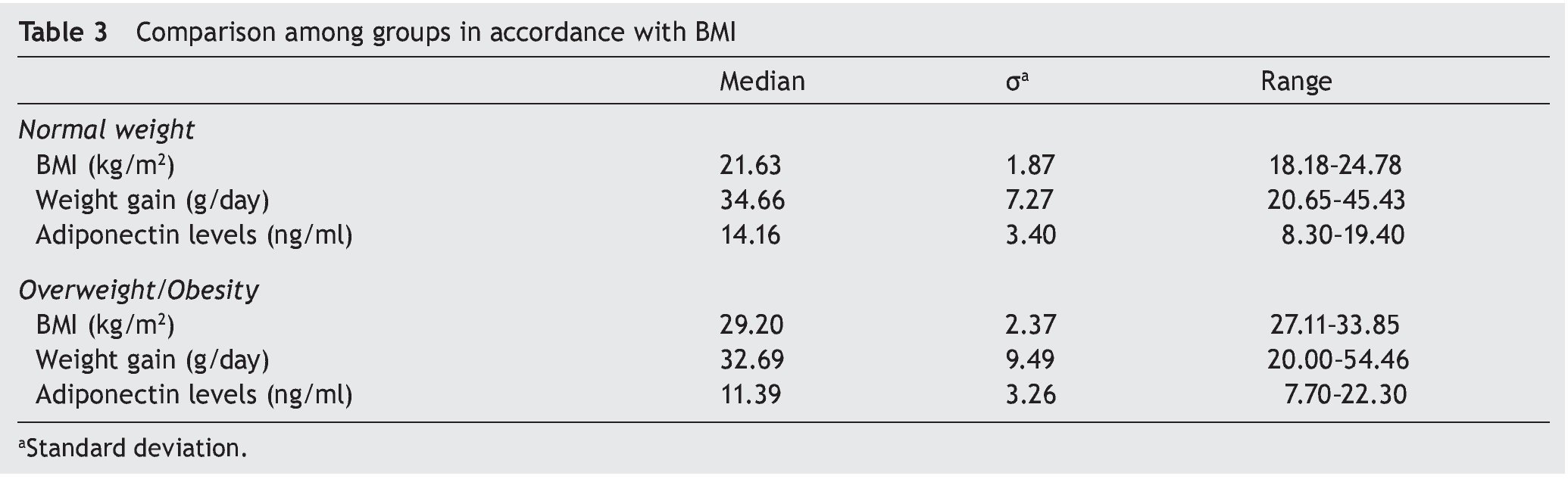
A total of 40 samples of breast milk were analyzed. Certain maternal and infant factors were analyzed to determine the characteristics of the population (Table 2). On comparing the groups, which were defined as overweight/obese (BMI >25 kg/m2) and normal weight (BMI <25 kg/m2), the results shown in Table 3 were obtained. It can be observed that children of mothers with an elevated BMI have higher birth-weight than children of mothers with normal BMI. However, weight gain of children of mothers with normal BMI is higher than that of children of mothers with elevated BMI. Adiponectin levels are higher in the maternal milk of mothers with normal BMI than in the maternal milk of mothers with high BMI.
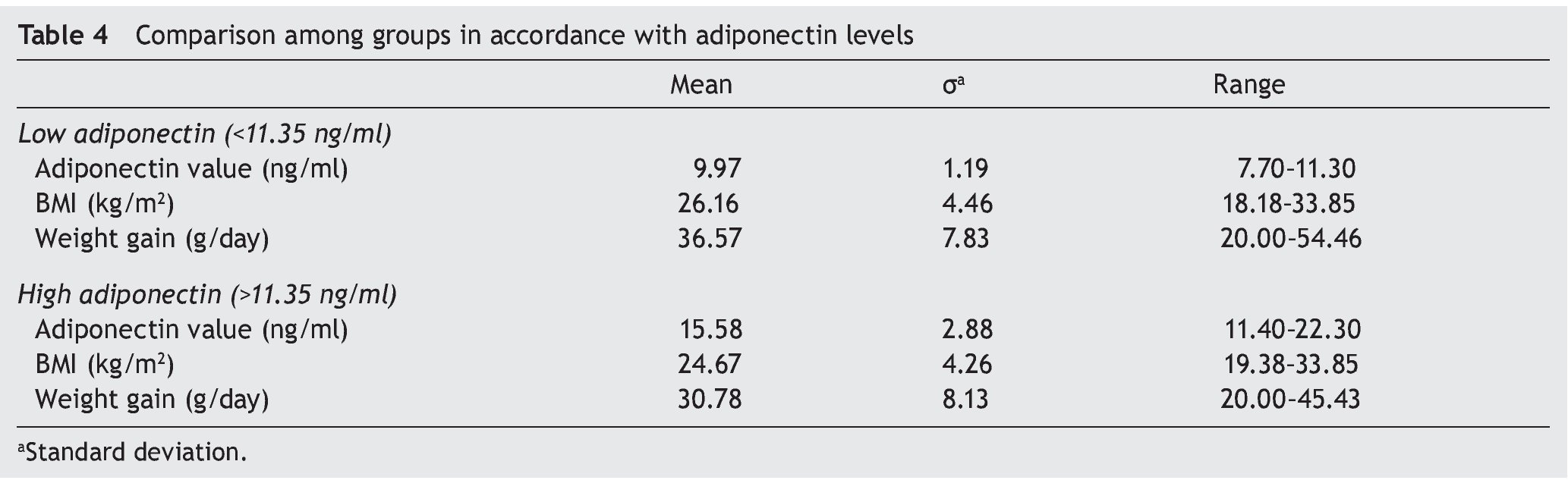
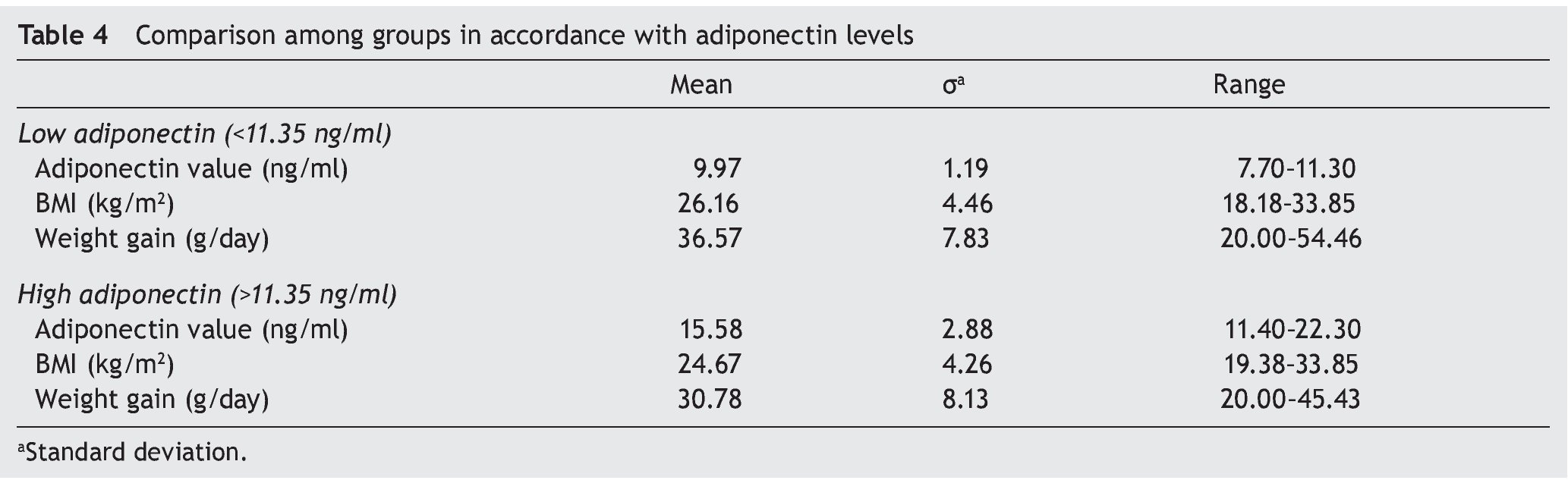
Using the same data, the groups were divided according to the levels of adiponectin: a group of “high adiponectin” and another group of “low adiponectin” without taking into account the BMI. The cut-off value for the separation of these groups was the median of the adiponectin values found in the 40 samples (Table 4). It can be seen that adiponectin levels in maternal milk differ significantly. Maternal milk of the group with low adiponectin levels have a mean concentration of 9.97 ng/ml, and maternal milk from the group with high adiponectin a mean of 15.57 ng/ml. In spite of this, differences in BMI are discrete between groups, taking into account both the BMI before and after pregnancy. Mean levels of adiponectin in both groups were below the cut-off for obesity. What can be seen in this concentrate is that infants who are consuming breast milk with high adiponectin levels have as background a weight greater than those who are consuming breast milk with low levels of adiponectin. However, weight gain of infants who consume breast milk with high adiponectin levels is less than those who consume breast milk with low adiponectin levels.
4. Discussion
The results obtained are in opposition to what has been reported in previous investigations.15,16 In these studies it has been observed that there is a direct proportional relationship between maternal BMI and adiponectin levels in breast milk. However, results of the present study report that adiponectin levels are higher in breast milk of mothers with a lower BMI. It is important to mention that the studies referenced were not designed for correlating BMI with levels of adiponectin in breast milk. This relationship is only mentioned in the population analysis, but it is not made clear if these differences were statistically significant.15,16 There are studies in which it has been noted that adiponectin levels are decreased in obese patients and increased in patients with adequate BMI7, thus it can be assumed that serum levels would correlate with the levels in breast milk. Because serum levels of adiponectin were not measured in this case, it can only be assumed that patients with higher levels of adiponectin in breast milk also have higher serum levels.
It is noteworthy that on performing this analysis a higher weight gain is observed in infants of mothers in the normal-weight group and who therefore had higher levels of adiponectin. Despite this, it was concluded that there was no significant difference between the averages of the two groups. The expectation was that infants fed breast milk with higher adiponectin content would have a lower weight gain. In previous studies it was found that weight gain in the first 6 months of life is at the expense of fatty tissue and subsequently to lean tissue.17
For these reasons, it was decided to analyze the population with respect to adiponectin levels. Two groups were formed called “high adiponectin” and “low adiponectin.” The median of the values obtained from the analysis of the 40 samples was taken to carry out this division, which resulted in 11.35 ng/ml (Table 2). From this concentration, the lower values were determined as “low adiponectin” and higher values as “high adiponectin” without taking into account the maternal BMI (Table 4). With the use of descriptive statistics it was shown that adiponectin levels in breast milk differed considerably. Breast milk of the “low adiponectin” group had a mean of 9.97 ng/ml and breast milk from the group with “high adiponectin” had a mean of 15.57 ng/ml. Differences in BMI were not as wide in these groups. The means were found below the cut-off point for obesity: 26.15 kg/m2 for the “low adiponectin” group and 24.67 kg/m2 for the “high adiponectin” group. Infants who consumed breast milk with high adiponectin levels had a history of having a higher birth weight (mean 3087 g) than those who consumed breast milk with low adiponectin levels (mean 2879 g). However, differences in mean birth weights were not significant.
The calculated weight gain was lower in infants who consumed breast milk with high adiponectin levels than in those who consumed breast milk with low levels of adiponectin, with respective means of 30.78 g/day and 36.56 g/day. These differences had a value of p <0.05, thus proving that the difference in the means in weight gain were significant. These results are in agreement with Kotani et al. who observed that newborns with higher levels of adiponectin in the umbilical cord blood had a higher weight at birth.9 Adiponectin levels in umbilical cord blood were not determined in the present study, but it can be assumed that mothers who produce breast milk with higher amounts of adiponectin would have a higher serum adiponectin. Therefore, their children had a higher birth weight. However, difference in birth weights was not significant after performing statistical analysis.
In terms of weight gain, the results obtained are consistent with what was observed in previous studies.14 The group of infants consuming breast milk with higher levels of adiponectin had less weight gain. This could be due to the modulation of the infant’s metabolism by the adiponectin present in the breast milk related, in turn, with the protection against obesity provided by feeding with breast milk.
One the main limitations of this study is the short follow-up period provided to the patient because the weight gain was only obtained from the period of 4 to 8 weeks of life. However, because the database is available, one could provide follow-up to these 40 children and see the behavior of the weight through the years. Future follow-up would allow evaluating if there is agreement with what has been reported in other investigations such as Weyerman in 2007 or Woo in 2012 in which it was found that at 2 years of life the children exposed to breast milk with higher adiponectin had a greater weight gain.
In light of the results obtained in this study, it would be interesting to measure serum adiponectin levels in the mother (to evaluate if there is a correlation with the levels in secreted breast milk) as well as to measure serum adiponectin levels in infants who consume this milk (to see if their levels are positively related). It would also be important to determine these levels in different populations. In the present study the sample was limited to the metropolitan area of Monterrey and to patients who received public medical care. It would be of great interest to see if socioeconomic status, nutrition and other factors affect the levels of this hormone.
Analysis of the results obtained in this work allowed for formulating three concrete conclusions as follows:
• There is a relationship between maternal BMI and adiponectin levels in breast milk, which are higher in mothers with a lower BMI.
• A relationship exists between adiponectin levels and weight gain of the infants, with a lower weight gain in those infants who consume breast milk with higher levels of adiponectin.
• Follow-up is necessary in these children to determine their behavior with regard to nutritional status during their development.
Ethical disclosure
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Conflict of interest
The authors declare no conflict of interest.
Received 3 June 2015;
accepted 28 July 2015
* Corresponding author.
E-mail:dr.abegalindo@gmail.com (A. Galindo Gómez).