




Early childhood development (ECD) is the foundation of countries’ economic and social development and their ability to meet the Sustainable Development Goals (SDGs). Gestation and the first three years of life are critical for children to have adequate physical, psychosocial, emotional and cognitive development for the rest of their lives. Nurturing care and protection of children during gestation and early childhood are necessary for the development of trillions of neurons and synapses necessary for healthy development. ECD requires access to good nutrition and health services from gestation, responsive caregiving according to the child's developmental stage, social protection, child welfare, and early stimulation and learning opportunities. Six actions are recommended to improve national ECD programs: expand political will and funding; create a supportive, evidence-based policy environment; build capacity through inter-sectoral coordination; ensure fair and transparent governance of programs and services; increase support for multidisciplinary research, and promote the development of leaders. Mexico has made significant progress under the leadership of the Health Ministry but still faces major challenges. The recent creation of a national inter-sectoral framework to enable ECD with the support of international organizations and the participation of civil society organizations can help overcome these difficulties.
El desarrollo infantil temprano (DIT) es la base del desarrollo económico y social de los países y de su capacidad de cumplir con los Objetivos de Desarrollo Sostenible (ODS). La gestación y los primeros 3 años de vida son fundamentales para que los niños tengan un desarrollo físico, psicosocial, emocional y cognitivo adecuado para el resto de sus vidas. La crianza y el cuidado cariñoso y sensible a las necesidades de los niños durante la gestación y la primera infancia son esenciales para el desarrollo de los billones de neuronas y trillones de sinapsis necesarias. El DIT requiere de acceso a buena nutrición y servicios de salud desde la gestación, crianza sensible de acuerdo a la etapa de desarrollo del niño, protección social y del bienestar del niño, y oportunidades de estimulación y aprendizaje temprano. Para mejorar el DIT a nivel nacional se recomiendan seis acciones con fuerte participación de la sociedad civil: expandir la voluntad política y financiamiento, crear un entorno de políticas favorables basadas en evidencia, construir capacidad con coordinación intersectorial, asegurar una gobernanza justa y transparente de los programas y servicios, aumentar apoyo a la investigación multidisciplinaria y promover el desarrollo de líderes. México ha logrado avances importantes en DIT bajo el liderazgo del Sector Salud, pero enfrenta retos significativos para implementar estas recomendaciones. La reciente creación de un marco nacional intersectorial favorable al DIT con apoyo de los organismos internacionales y la participación de la sociedad civil pueden ayudar a sobreponer estos retos.
Human development, which is the basis of social capital and the economic development of countries, is based on a process where different skills are developed at different times, following a continuous sequence that builds on skills acquired from the beginning of life if the necessary conditions exist. These include the senses, motor, cognitive, linguistic, and socio-emotional skills; and self-regulation of behavior and emotions. That is why investing in improving child development is central to enable countries to meet the Sustainable Development Goals (SDGs).1 The healthy development of all girls and boys is necessary for countries to grow economically in an equitable and sustainable way. Returns on early childhood investments are very high and therefore are considered highly cost-effective.2 Unfortunately, an alarming 43% of children under five years old (249 million) in low- and middle- income countries are at risk of poor development due to the chronic poverty and malnutrition in which they live. This number increases if we also take into account other risk factors for poor early childhood development (ECD) such as the low level of maternal education and child abuse.3 There are differences in the distribution of poor ECD between and within countries, explained by the great inequality and social injustice. For this reason, international organizations have identified as a priority for the 21st century to improve ECD, paying particular attention to the most vulnerable. Therefore, a key question is what do we know about how ECD can be improved?
The recent publication of the new Lancet ECD Series offers a historic opportunity for governments to implement large - scale evidence - based programs. The core of this series is three articles that update the knowledge on progress in the neurosciences,3 evidence-based bundles of intervention,4 the implementation and cost of effective ECD large - scale programs5 and the cost to society of not investing in ECD.5 Here forward, we summarize the lessons learned from this new series and our country's progress and challenges towards building a comprehensive ECD policy.
2Advances in NeurosciencesBrain cells or neurons; begin to multiply rapidly from gestation. By four weeks of pregnancy, these cells multiply at a rate of 250,000 neurons per minute. At birth, the newborn has 100 billion neurons, equivalent to all the stars in the universe. During the third trimester of gestation, the brain begins to establish connections or synapses to facilitate communication between neurons and establish the neurological pathways, which are the basis of human development.
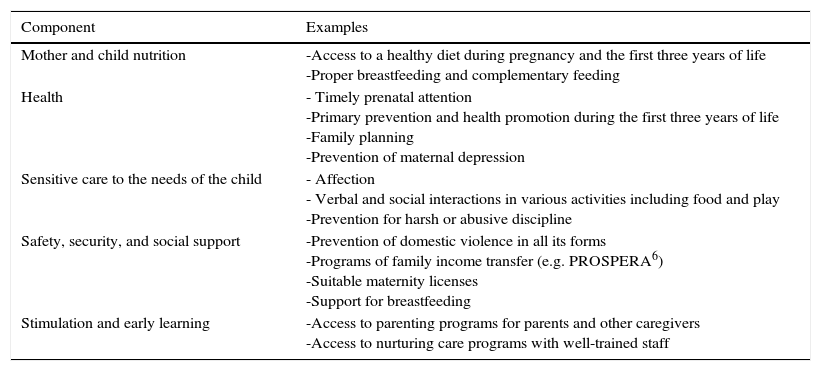
Specifically, the synapses are essential to develop the senses, learn, develop memories, feelings and healthy behaviors.3 Synapses develop extremely fast during the first three years of life, in the order of trillions, in response to loving and sensitive caring of the needs of children (nurturing care). Therefore, the first three years of life together with gestation are considered a highly sensitive period in human development.3 Nurturing care is based on proper nutrition, health, stimulation and opportunities for early learning, social protection and protection against all forms of violence against children (Table 1).3 In fact, it is estimated that under these conditions the synapses are formed at a rate of 1000 per second during the first years of life. During this stage of life, children's brains are like a sponge that absorbs all their experiences and interactions with their surrounding environment. The better the conditions for nurturing care, the more synapses will form, in the order of trillions. Unfortunately, when children do not have access to nurturing care, not enough synapses are established, or they are too weak to sustain an adequate development for the remaining life.3
Components of nurturing care.
| Component | Examples |
|---|---|
| Mother and child nutrition | -Access to a healthy diet during pregnancy and the first three years of life -Proper breastfeeding and complementary feeding |
| Health | - Timely prenatal attention -Primary prevention and health promotion during the first three years of life -Family planning -Prevention of maternal depression |
| Sensitive care to the needs of the child | - Affection - Verbal and social interactions in various activities including food and play -Prevention for harsh or abusive discipline |
| Safety, security, and social support | -Prevention of domestic violence in all its forms -Programs of family income transfer (e.g. PROSPERA6) -Suitable maternity licenses -Support for breastfeeding |
| Stimulation and early learning | -Access to parenting programs for parents and other caregivers -Access to nurturing care programs with well-trained staff |
* Adapted from Black et al. [Ref. 3].
In summary, advances in neuroscience clearly indicate that gestation and the first three years of life are critical to establishing the basis of human development, where newly acquired skills are built on previously solidified abilities. Therefore, substantial investments should be made in improving children's ECD from the moment they are conceived. Although science has also indicated that investments after the first three years of life can partially restore developmental loss - due to lack of nurturing care during early childhood - the evidence clearly shows that the earlier nurturing care starts, the better the results will be in the long term (Table 2).3
Progress in Neurosciences for Early Childhood Development: Main Messages.
| By four weeks of gestation, the neurons multiply at a rate of 250,000 neurons per minute |
| Under appropriate conditions, the newborn already has 100 billion neurons |
| Under appropriate parenting and child care conditions, synapses are formed at a rate of 1000 per second during the early years of life |
| The better the nurturing care in children is during the first three years of life, the more synapses will be formed, and they will be stronger |
| When children do not have access to nurturing care during early childhood, not enough synapses are established, or these are too weak to sustain an adequate development for the rest of life |
| The earlier we start in life by providing opportunities for nurturing care, the better long-term results will be obtained |
* Adapted from Black et al. [Ref. 3].
As indicated in the previous section, nurturing care during the first three years of life requires access to good nutrition, health, opportunities for early stimulation and learning, social protection and protection against all forms of violence against children. Because nurturing care is the basis for proper ECD, it is important to identify intervention bundles throughout the life course that can be delivered in an integrated manner.
There are highly effective ECD interventions covering adolescence, adulthood, pregnancy and the first three years of life.4 In the health and nutrition sector, these include; family planning and pre and peri-conception maternal nutrition, antenatal care and nutrition, evaluation and management of fetal growth and health, appropriate management of complications during pregnancy, management of labor, and delivery, birth complications, immediate newborn care, neonatal disease prevention and management, home-based nutritional care and support, promotion and support of recommended infant feeding patterns (including breastfeeding and healthy and nutritious complementary feeding), hygiene promotion (including hand washing), infectious disease prevention and detection and management of common childhood diseases.4 On social protection and education sectors, effective interventions to promote ECD include; parent education programs on parenting and nurturing care, promotion of mothers’ health and well-being (including mental health), conditional cash transfer programs (e.g. PROSPERA).6 Regarding other sectors, it is necessary to have access to safe drinking water and sanitation.4
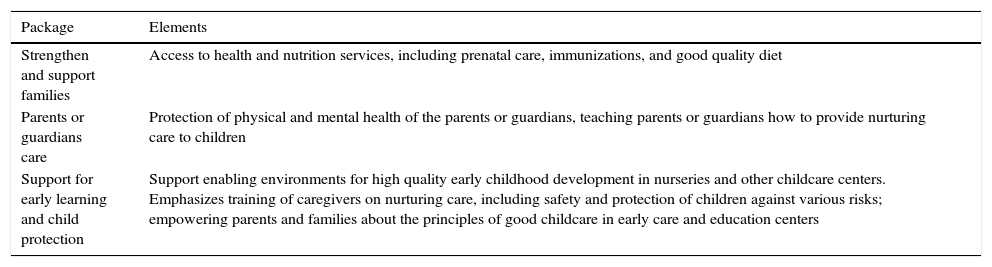
These series of specific life course interventions, including adolescence, adulthood, pregnancy, and the first three years of life, have been consolidated into bundles designed to strengthen and support families, care of parents, or guardians of children, early learning and child protection (Table 3).4
Packages that are integrated through effective early childhood development programs.
| Package | Elements |
|---|---|
| Strengthen and support families | Access to health and nutrition services, including prenatal care, immunizations, and good quality diet |
| Parents or guardians care | Protection of physical and mental health of the parents or guardians, teaching parents or guardians how to provide nurturing care to children |
| Support for early learning and child protection | Support enabling environments for high quality early childhood development in nurseries and other childcare centers. Emphasizes training of caregivers on nurturing care, including safety and protection of children against various risks; empowering parents and families about the principles of good childcare in early care and education centers |
* Adapted from Britto et al. [Ref. 4].
The experience on large scale implementation of integrated ECD programs has shown that to succeed, political will is paramount, as well as evidenced-based legislation and public policies, and the use of government financial resources and existing structures.5Chile Grows with You is an integrated ECD program, which is being emulated in other Latin American countries and other parts of the world.5,7
Chile Grows with You is a multisectoral evidence-based program that follows a life course approach, which has been implemented with political will at the highest level and the strong participation of civil society. Recognizing significant social inequities in ECD was a fundamental reason for the program to emerge from a national consensus. The program began to be implemented in 2007, and in 2009 the law and budget were approved to ensure the program would prevail regardless of the changes in the country's political administration. The program is funded by the government and coordinated by the Ministry of Social Development in conjunction with the Ministry of Health and the Ministry of Education, and in consultation with other relevant ministries to protect and promote ECD.5,7
Chile Grows with You integrates health, education, and empowerment of parents to support their children's development, stimulation and early education. Currently, the program covers a target population from gestation to four years of life, including evidence-based interventions addressed to parents or guardians nurturing care. The entry point to the program is prenatal care through the public health system, reaching 80% of the target population. The program offers universal benefits such as prenatal care and humanized labor and delivery, neonatal screening and timely care of the newborn, breastfeeding support, vaccines, high-quality ECD information for families and health care providers, and childcare through a radio program and website.5,7
Chile Grows with You also offers distinct benefits based on socioeconomic risks, family, and disabilities. Specifically, the program provides access to maternal and child health services, risk screening, and referrals of children with developmental delays or who are hospitalized. It also ensures that children under four years old who live in families with risk factors for their development have opportunities for early stimulation and learning from early childhood to preschool education. Families in poverty are referred to additional social protection services, like income transfer programs and home visits.5,7
In addition to its high coverage, process evaluations of Chile Grows with You have shown that the program has a clear and transparent governance regarding the distribution of resources and that there is a reasonably high degree of fidelity in delivering the various services included in the program. Although certain quality of services heterogeneity has been identified between communes and municipalities. These process evaluations have identified the following priorities for improving the program; developing written protocols to standardize implementation of program procedures and activities in all municipalities in the country, strengthening the monitoring and information management system to enable timely decisions at the local levels, strengthen human resources development capacity to address the various aspects of the ECD throughout the life course, expand the program beyond the first four years of life, and include aspects not previously considered as the childhood obesity epidemic in the country and its possible consequences for ECD. It is also important to strengthen the program ECD impact assessments and reduce social inequalities.5,7
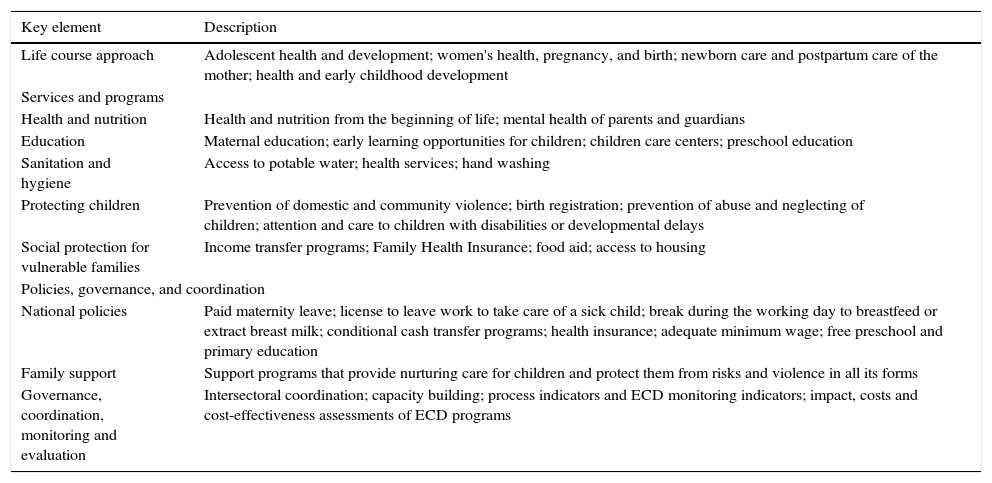
A comparison of integrated ECD multisectoral programs based on programs implemented in Bangladesh, Chile, India, and South Africa indicates that these programs arose out of political and social concerns about poverty, inequity and social exclusion. It also shows that their success is due to the fact that they are based on scientific and economic evidence, have a comprehensive vision of integrated services, are established with government statutes as state policy, are financed and led by the government, and have different entry points (although the most effective is through the health sector, starting from prenatal care).5,7 Successful large-scale ECD programs are anchored in frameworks consistent with socio-ecological models of health, emphasizing attention to social determinants of health throughout the life course (Table 4).
Key elements of ECD large scale integrated programs: Lessons from Bangladesh, Chile, India, and South Africa.
| Key element | Description |
|---|---|
| Life course approach | Adolescent health and development; women's health, pregnancy, and birth; newborn care and postpartum care of the mother; health and early childhood development |
| Services and programs | |
| Health and nutrition | Health and nutrition from the beginning of life; mental health of parents and guardians |
| Education | Maternal education; early learning opportunities for children; children care centers; preschool education |
| Sanitation and hygiene | Access to potable water; health services; hand washing |
| Protecting children | Prevention of domestic and community violence; birth registration; prevention of abuse and neglecting of children; attention and care to children with disabilities or developmental delays |
| Social protection for vulnerable families | Income transfer programs; Family Health Insurance; food aid; access to housing |
| Policies, governance, and coordination | |
| National policies | Paid maternity leave; license to leave work to take care of a sick child; break during the working day to breastfeed or extract breast milk; conditional cash transfer programs; health insurance; adequate minimum wage; free preschool and primary education |
| Family support | Support programs that provide nurturing care for children and protect them from risks and violence in all its forms |
| Governance, coordination, monitoring and evaluation | Intersectoral coordination; capacity building; process indicators and ECD monitoring indicators; impact, costs and cost-effectiveness assessments of ECD programs |
ECD: early childhood development.
Adapted from Richter et al. [Ref. 5, 7].
Comparison of these programs also indicates that there is no single route to coordinate effective large-scale ECD programs; each country must decide according to its reality and diverse social, economic, political and cultural contexts. In some cases, sectors can serve children and families independently, albeit under a structure with shared responsibilities at national and local levels. In other contexts, a single ministry can work in coordination with other sectors. In the case of Chile Grows with You and the Colombian De Cero a Siempre program coordination is done through a national council representing the ECD policy of the country.5,7
In recent years, substantial advances have been made in Mexico for the construction of public policy:
For the first time, in the National Development Plan of 2013-2018 the Government of the Republic, within the National Goal: Inclusive Mexico, objective 2.1, strategy 2.1.2, included the line of action: Promoting early childhood development actions.8 It is within the frame of this line of action that the Hospital Infantil de Mexico Federico Gómez developed for PROSPERA the PRADI model during 2013.9 This model includes two components, timely detection and attention of development problems. This is done using the child development evaluation test (EDI)10 designed and validated in Mexico,11–13 which is recommended for the assessment of child development in primary care facilities.14
On December 4th, 2014 the President of the Republic promulgated the “General Law for boys, girls, and adolescents” where children and youth are recognized as rights holders. Also, this law recognizes their superior interest and right of priority and mandates “creating and regulating the National Integrated Protection System of the Rights of Boys, Girls and Adolescents (SIPINNA)”.15
During the second ordinary session of SIPINNA in August 2016, proposed the “25 to 25: National Objectives for Rights of Boys, Girls and Adolescents” as a national public policy instrument to guarantee the rights of children and youth. Within the survival domain, it was established and objective number 4, the early child development.16 In addition to the above, SIPINNA also called for the creation of a Permanent Commission for Early Childhood Development, which called for the development of public policy for early childhood, by the end of 2016.
In summary, the accumulated experience of integrated ECD programs offers useful lessons that countries can use to translate the vast knowledge that is available in large-scale effective policies and programs. In this way, countries can build ECD state policies to meet one of the most important priorities at the global level, to meet the Sustainable Development Goals for the year 2030. In Mexico, there has been a significant advance in this area in recent years, although the process to translate it into a comprehensive public policy is still pending.
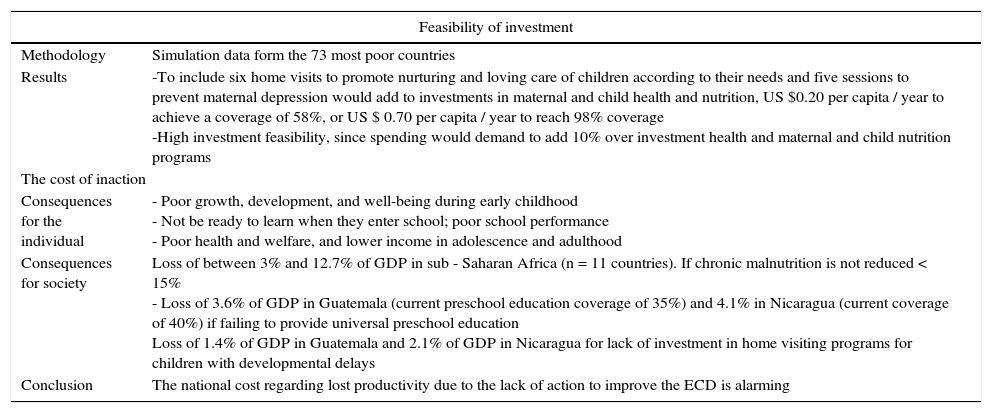
5The cost to society of not investing in ECDA feasibility of ECD programs simulation study based on cost was conducted with data from 73 extremely poor developing countries.5The results were very encouraging: they showed that including six home visits to promote the nurturing and caring of children according to their needs and five sessions to prevent maternal depression would add to investments in maternal and infant health and nutrition US $ 0.20 /capita/year in low-income countries or US $ 0.70 /capita/year in middle-income countries. This expenditure would represent adding 10% to what is already been invested in health, nutrition and education programs.5 The cost of not making these highly feasible investments, i.e. not acting despite the evidence, is enormous for society, as this affects the prevention of good growth and development during early childhood, the ability of children to be ready to learn once they enter school, school performance, cognitive level and overall well-being in adolescence and adulthood. In fact, long-term prospective studies in Guatemala and Jamaica showed that the lack of investments in health, nutrition, and nurturing translates into a loss of 25% of wages in adulthood relative to the national average and that the deficit in skills development is transferred from one generation to the next (Table 5).5
Feasibility of financing early childhood development programs on a large scale; and individual and social cost of not investing.
| Feasibility of investment | |
|---|---|
| Methodology | Simulation data form the 73 most poor countries |
| Results | -To include six home visits to promote nurturing and loving care of children according to their needs and five sessions to prevent maternal depression would add to investments in maternal and child health and nutrition, US $0.20 per capita / year to achieve a coverage of 58%, or US $ 0.70 per capita / year to reach 98% coverage -High investment feasibility, since spending would demand to add 10% over investment health and maternal and child nutrition programs |
| The cost of inaction | |
| Consequences for the individual | - Poor growth, development, and well-being during early childhood - Not be ready to learn when they enter school; poor school performance - Poor health and welfare, and lower income in adolescence and adulthood |
| Consequences for society | Loss of between 3% and 12.7% of GDP in sub - Saharan Africa (n = 11 countries). If chronic malnutrition is not reduced < 15% - Loss of 3.6% of GDP in Guatemala (current preschool education coverage of 35%) and 4.1% in Nicaragua (current coverage of 40%) if failing to provide universal preschool education Loss of 1.4% of GDP in Guatemala and 2.1% of GDP in Nicaragua for lack of investment in home visiting programs for children with developmental delays |
| Conclusion | The national cost regarding lost productivity due to the lack of action to improve the ECD is alarming |
GDP: GDP; ECD: early childhood development.
Adapted from Richter et al. [Ref. 5]
Analysis of data from 11 sub-Saharan African countries showed that not reducing chronic undernutrition (i.e. short stature for age) to a prevalence of at least 15% leads to a loss of between 3 and 12.7% of the Gross Domestic Product (GDP).5,7 Similarly, not offering universal preschool education was associated with a loss of 3.6% of GDP in Guatemala (current preschool education coverage of 35%) and 4.1% in Nicaragua (current coverage of 40%).5,7 Adding a loss of 1.4% of GDP in Guatemala and of 2.1% of GDP in Nicaragua due to a lack of investment in home visiting programs for children with developmental delays, the national cost regarding lost productivity due to the lack of actions to improve ECD is alarming.
In public policy, budget allocation is a priority indicator. Thus, knowing how much governments invest in early childhood is a clear indication of the level of priority given to this age group and the development of their capacities.
6Investments in early infancy in Mexico.The scientific evidence reviewed in this and other works by prominent economists, such as the Nobel laureate James Heckman, has demonstrated that investing in the full development of early childhood is a measure of clear economic and technical rationality. For each Mexican peso invested, great returns are obtained throughout the life cycle thanks to the effects that a better development of capacities generates in the short, medium and long term: a better self-care of health, better school performance and greater schooling level, greater productivity, sociability and fewer propensities for criminal activities. Heckman estimates that the amount of this return ranges from 7 to 10% per year.
However, how much does Mexico invest in early childhood? There are several studies that have sought to answer this question. One of them was the analysis carried out by Mexicanos Primero in 2014 based on data published by the Organization for Economic Cooperation and Development (OECD), in the book “The Invisibles.” According to these data, public spending on the care and education of children aged 0-5 in 2009 was approximately 0.6% of GDP. Under the same criteria, it was possible to establish that other countries in the region invest more in this age group. Mexico ranked 18th out of 39 countries, slightly below the 0.7% average. Latvia, Lithuania, Australia and Spain have a similar investment.17
The Inter-American Development Bank (IDB), in its book “The First Years: Child Welfare and the Role of Public Policies”, estimated that in 2012 Mexico invested about 0.6% of GDP in its population under 5, and about 1.4% of the population between 6 and 12.18 As it can be seen, investment in early childhood was only half that in late childhood.
The last study recently published by UNESCO and UNICEF, under a maximalist approach which considered not only direct costs in early childhood but also a large type of indirect expenses, in addition to investments made from gestation and up to eight years old estimated that Mexico invested 0.77% of GDP in early childhood in 2013.
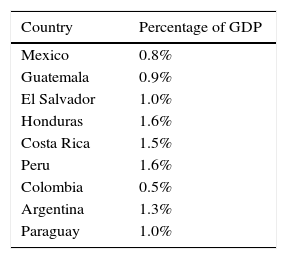
Although this latter estimate is slightly higher than that reported by the IDB or Mexicanos Primero, under the same criteria, Mexico continues to be a country that invests relatively little in early childhood. Countries such as Honduras and Costa Rica allocate the double of investment: 1.6% and 1.5% of GDP, respectively. Table 6 reproduces the percentage of GDP invested in early childhood by nine countries in the region according to the study “Investing in early childhood in Latin America”.19
The same study indicates that the investment that Mexico makes in its children from 0 to 8 years old represents a minimum part of its total public expenditure (GPT): only 4%. Countries like Peru allocate up to 9.1% of their GPT in early childhood.
Under this maximalist methodology, Mexico invested 124,559.3 millions of pesos in 2013, but only 27.9% were specifically spent in early childhood; that is, only 34,751.76 millions of pesos. This amount is much lower than the one destined by the Federal Government to subsidize the prices of the electric tariffs, which in the Federal Expenditures Project of 2017 was estimated at 43,114 million. Various economic analyses confirm that subsidies of this nature are highly regressive, as they greatly benefit the wealthiest deciles of the population.
A study that specifically shows the investment in ECD in Mexico is the one done to determine the investment made in the detection and timely attention to development problems in the population of the Health component of the PROSPERA Social Inclusion Program. Within the framework of this program, since 2010, increasing resources have been allocated for a total amount of almost 600 million Mexican pesos (approximately 30,000,000 USD) for the implementation of ECD oriented interventions and research. The annual per capita investment in the period 2012-2015 has risen from 11.66 to 247 pesos (0.61 to 12.99 USD),20 resulting in a higher percentage of children who were evaluated and received interventions to improve their development level.
7The health care system's role and advances in ECD public policy in MexicoECD represents a significant challenge for the health care system, whose responsibility is to ensure an effective response that includes equity in care and financial protection for the full potential of child development. To do so, it requires compliance with its essential functions: governance, financing, resource generation and service provision.21
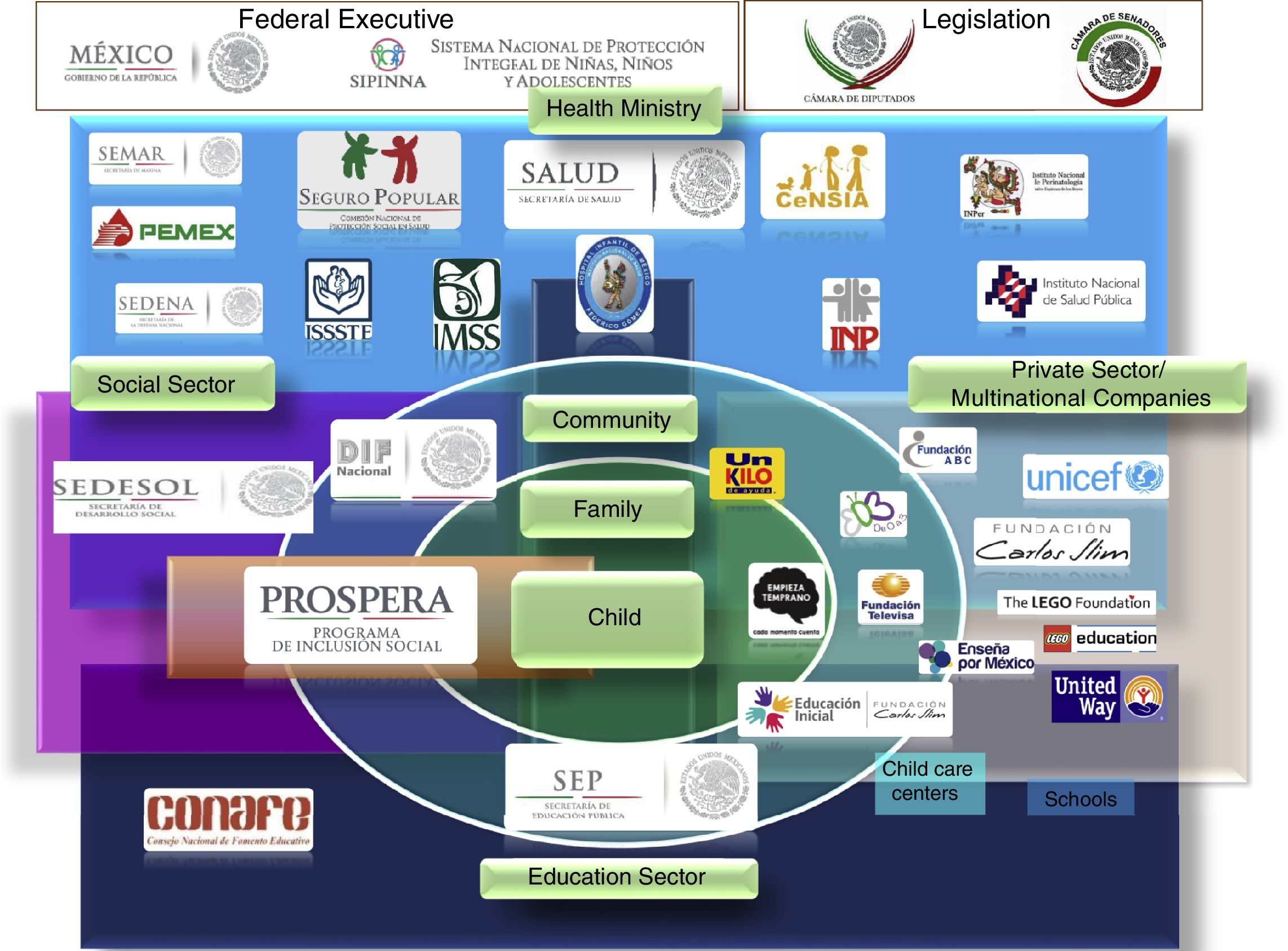
Under the concept of governance as a decision-making system aimed at the implementation of authority through the joint commitment of social and economic actors, and to promote the development and implementation of policies,22 Mexico's health care system is facing significant challenges. In principle, the coordination for intersectoral action, which includes both the public and private sectors and the population itself to promote the ECD with strategies that, allow communication, trust, understanding and commitment. Also, the inclusion of the ECD as a human right, a global public good and a component of welfare and equity, which means social justice. To do this, it must incorporate into the policies and programs of ECD the value of scientific evidence and its function as a consolidated institution to exercise its leadership. Figure 1 shows an outline of the results of the joint work of the health sector with the three most important sectors in this area: social, educational and private, who have contributed to different programs and strategies to strengthen the focus to ECD through their corresponding institutions.

Regarding financing, the sustainability of the programs is fundamental to achieve the expected impact and, in the case of ECD, as an investment whose social return is assured. To fulfill this responsibility, the Health System must promote the implementation of cost-effective interventions focused on the prevention and reduction of the risks for alterations in neurodevelopment, as well as its diagnosis and early intervention.
Human resources are the center of the Health Sector and of progress in improving the health conditions of the population. There is strong evidence that the coverage and quality of the care provided by health services is associated with the survival of the population, particularly maternal and child survival23 The above means that the joint coordination with the Education Sector to ensure that the training of human resources is oriented to the coverage and quality of professionals with the necessary profile for their incorporation into the ECD services. By 2015, the Health Component of PROSPERA had hired almost 400 psychologists for the screening and early care of children with developmental disabilities and had trained health professionals (doctors and nurses) in nearly 80% of all the Ministry of Health medical units.20
The integration of governance functions, financing, and human resources has formed the basis for the transformation of the ECD delivery function service from a curative model, segmented and with insufficiently trained health personnel, to the model of Health Promotion and Child Development Care (PRADI) of the PROSPERA Social Inclusion Program. This model includes the family and the community as part of a multidisciplinary framework with health services centered in ECD. The sustainability of the implemented model will depend on the capacity of the Health Sector to break institutional barriers to bring real reform, aimed at improving children's present and future quality of life accompanied by transgenerational social investment returns.
8Civil society participation for ECD in MexicoThe full development of early childhood requires a coordinated effort from the public, private and civil society sectors. While governments have the responsibility of ensuring early childhood rights by scaling powerful universal and focused policies, civil society organizations and the private sector have the ability to design and implement innovative interventions and programs that generate evidence on cost-effective measures to ensure the full development of capacities in the early years of life.
An example of contribution by this third sector is the work that Un Kilo de Ayuda has carried out in collaboration with Mexicans First, the Child Development Center at Harvard and the Accelerator of Innovations for Early Childhood. Thanks to the funding and technical support received, Un Kilo de Ayuda is testing a home intervention aimed at improving the interactions and childcare routines of the mother by incorporating play into everyday family activities.
This intervention is an innovation within an integrated model operated by the organization, which since 2008 teaches workshops on nutrition, health, and timely stimulation and assesses the growth and neurological development of about 50,000 children throughout the country. Recently, in collaboration with the Hospital Infantil de Mexico Federico Gómez, Un Kilo de Ayuda included the Child Development Assessment as a tool to monitor the development of children. Also it is currently working on developing a new curriculum that distinguishes developmental needs across age groups to achieve adequate performance in all dimensions of child development.
Similarly, civil society has the responsibility to advocate continually for the prioritization of early childhood. The democratic model involves a continuous change in priorities within the purview of government. Civil society organizations must ensure that early childhood development does not lose its relevance with changes of administrations and legislatures. By contrast, they must ensure that each new administration acquires a deep and genuine commitment with early childhood.
There are more than enough technical and economic arguments for investing and prioritization of early childhood. Beyond that, there is an inescapable ethical and legal mandate: it is the State's responsibility to guarantee the full exercise of rights of its population. This will only be fulfilled if we start from early childhood.
9ConclusionsAdvances in behavioral and neurosciences, as in maternal and child health and nutrition show that, as new skills are built on previous ones, there must be appropriate developmental conditions before and during pregnancy, the first three years of life, and throughout the life course.
The period of gestation and the first three years of life represent a window of opportunity that in the long term is extremely sensitive to the physical, social, emotional and cognitive development of individuals. Investing in ECD from the beginning of life and early childhood has a high return rate. Although interventions that begin after three years of life have benefits, they may only partially benefit children who did not receive a sensitive and loving care during pregnancy and their first three years of life.24 These benefits are relatively small compared to the benefits obtained when appropriate conditions and child development programs are offered earlier.2
National integrated ECD programs with good intersectoral coordination must be grounded on a socio-ecological model, where the ability of parents or guardians and caregivers to provide loving care to children depends on the family and community environment, and the availability of services, intersectoral programs and public policies that promote and protect children's development from the beginning of life (Figure 2).

Scientific studies have identified some interventions that are efficient in providing sensitive care to the needs of children during their early childhood. These interventions include nutrition and maternal and child health programs to teach parents how to be sensitive to the needs of their young children, prevention of domestic violence and child abuse in all its forms, and the prevention and management of maternal depression. There have also been identified key policies that facilitate the ability of families to provide nurturing care to their children. These include adequate maternity permissions to leave work to care for sick children or other relatives, breaks during working hours to breastfeed or extract milk, social protection programs through conditional income transfer (e.g. PROSPERA6). In the last decade, much has been learned about the essential elements for effective national ECD programs.
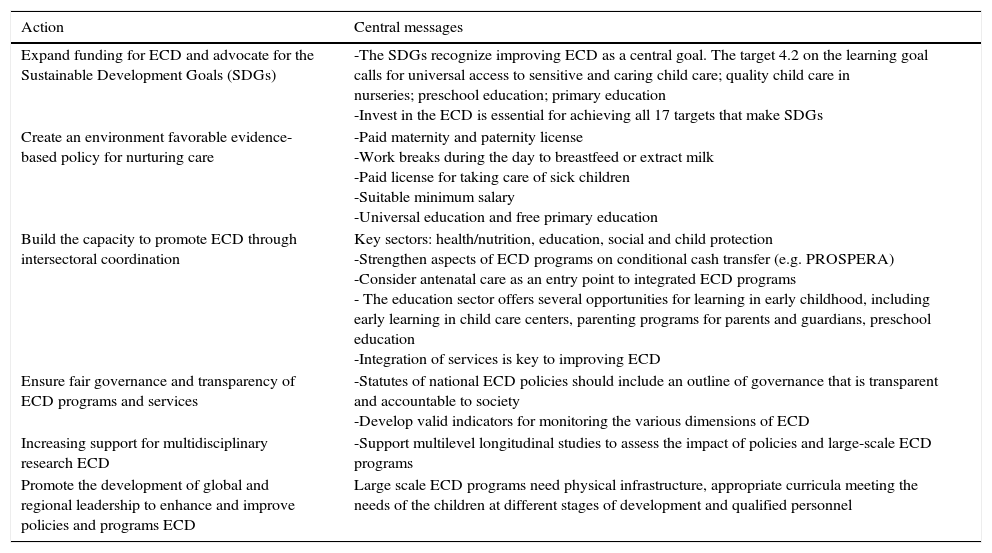
It is important to recognize that, despite all existing knowledge to develop and implement large-scale programs and policies, two-thirds of the world's countries do not have yet a national unified multisectoral framework and well-coordinated efforts to protect, promote and support ECD.5 The cost of this lack of intersectoral coordination is enormous for individuals, families, societies and the world because of the great loss of human and social capital resulting from this situation. Therefore, it is important that civil society gets involved in evidence-based advocacy efforts to improve ECD in their countries. Specifically, it is recommended that six actions are implemented to improve the level of investment in ECD5 (Table 7).
Recommended actions for advancing the cause of early childhood development.
| Action | Central messages |
|---|---|
| Expand funding for ECD and advocate for the Sustainable Development Goals (SDGs) | -The SDGs recognize improving ECD as a central goal. The target 4.2 on the learning goal calls for universal access to sensitive and caring child care; quality child care in nurseries; preschool education; primary education -Invest in the ECD is essential for achieving all 17 targets that make SDGs |
| Create an environment favorable evidence-based policy for nurturing care | -Paid maternity and paternity license -Work breaks during the day to breastfeed or extract milk -Paid license for taking care of sick children -Suitable minimum salary -Universal education and free primary education |
| Build the capacity to promote ECD through intersectoral coordination | Key sectors: health/nutrition, education, social and child protection -Strengthen aspects of ECD programs on conditional cash transfer (e.g. PROSPERA) -Consider antenatal care as an entry point to integrated ECD programs - The education sector offers several opportunities for learning in early childhood, including early learning in child care centers, parenting programs for parents and guardians, preschool education -Integration of services is key to improving ECD |
| Ensure fair governance and transparency of ECD programs and services | -Statutes of national ECD policies should include an outline of governance that is transparent and accountable to society -Develop valid indicators for monitoring the various dimensions of ECD |
| Increasing support for multidisciplinary research ECD | -Support multilevel longitudinal studies to assess the impact of policies and large-scale ECD programs |
| Promote the development of global and regional leadership to enhance and improve policies and programs ECD | Large scale ECD programs need physical infrastructure, appropriate curricula meeting the needs of the children at different stages of development and qualified personnel |
ECD: early childhood development;
SDGs: Sustainable Development Goals [Ref. 24].
Adapted from Richter et al. [Ref. 5, 7].
Complying with these actions is critical, since investment in ECD is extremely cost-effective and is the fundamental basis of the Sustainable Development Goals, which collectively seek to achieve economic growth and equitable and sustainable national development in all the countries of the world.1 In Mexico, there have been significant advances in recent years, although it is necessary to invest more in inter-sectoral policies with a monitoring/evaluation system and with a specific budget allocation that allows effective access to the entire population under five years in the country.
FundingNone.
Conflict of interestThe authors do not have conflicts of interest to declare.
The first author of this article (RPE) was a member of the executive committee that produced the 2016 Lancet ECD Series, which he also coauthored.
This article is dedicated to all Mexican children, especially those to whom our society has not offered the opportunity to have nurturing care.
Please cite this article as: Pérez-Escamilla R, Rizzoli CA, Alonso CA, Reyes MH. Avances en el desarrollo infantil temprano: desde neuronas hasta programas a gran escala. Bol Med Hosp Infant Mex. 2017;74:86–97.