


Background: In Mexico, prevalence of anemia in children <5 years of age (preschool) is high at all socioeconomic levels. We undertook this study to analyze the socioeconomic determinants of the prevalence of anemia in preschool children and to explore the reasons why the prevalence is high, even in wealthier households.
Methods: We used the National Survey of Health and Nutrition (ENSANUT) 2012 and calculated logistic regression models, considering as explanatory variables socioeconomic characteristics of children and mothers, among others. Models were estimated for all preschoolers and for each tercil of socioeconomic status.
Results: The national prevalence of anemia in preschool children is 23.3%; in the lowest tertile it is 26.4%, whereas in the highest tertile it is 20.2%. Variables related to increased risk of anemia in the highest tertile are male children (OR: 1.24), those <2 years of age (OR: 2.31), stunting (OR: 2.01), and mother as the head of the household (OR: 2.06).
Conclusions: Although anemia prevalence is higher at poorer socioeconomic levels, it remains high at all socioeconomic levels. Therefore, a general strategy is required to reduce the rate of childhood anemia rather than only the targeted efforts followed so far. Further research is needed.
1. Introduction
Mexico has a polarity in regard to malnutrition conditions. Although undernutrition is decreasing, it coexists with increasing overweight and obesity in the same populations. Childhood undernutrition is concentrated in the lower socioeconomic status (SES) except for anemia where it is observed in all SES, although with a higher incidence in the lower income groups.
Anemia is defined as a low level of hemoglobin in red blood cells. The major clinical symptom of anemia and iron deficiency is pallor. Its physical symptom is fatigue.1 According to UNICEF, anemia has an impact on the intellectual development of children; it reduces learning ability and growth and damages the immune system.2 This health condition also has important implications for the economy. In ten selected countries, Horton and Ross (2007) found that anemia in all age groups represents an average loss at present value of 0.81% of GDP (0.37% in Honduras and 1.86% en Bangladesh) due to loss of labor productivity and lifetime earnings associated with cognitive losses and low physical performance. For calculations, the authors reviewed several studies that found that iron deficiency anemia reduces IQ cognitive test performance by half a standard deviation.3,4
Several factors have been associated with childhood anemia such as SES, age and parents' education, among others. A study in India showed that anemia in children aged 6 to 59 months has a strong negative association with status of literacy and wealth of parents.5 Studies about which factors may explain the presence of anemia in higher SES were not found, as anemia is most often associated with low SES. In México, De la Cruz-Góngora et al. estimated a logistic regression model for preschool children using the National Survey of Health and Nutrition 2012 (ENSANUT 2012) including SES as a covariate.6 However, the authors omitted relevant variables such as child's stunting status, iron supplement intake, food insecurity and mother's level of education and employment; therefore, the estimated effects on anemia of the included variables may be biased. In addition, the authors did not provide an explanation about why anemia is high in upper SES levels in Mexico.
This paper analyzes the prevalence of anemia in preschoolage children according to SES and other socioeconomic factors and makes the argument that, in Mexico, anemia is a public health problem generalized in all SES; therefore, generalized actions should be taken, Anemia has so far been associated with low SES and therefore government actions have been targeted mostly to those groups.
The model's intent is to find the factors associated with the presence of anemia in the different SES related to childhood conditions including overweight and obesity, household and mother´s characteristics.
2. Methods
The analysis is carried out using information from the ENSANUT 2012, which is representative nationwide. This survey contains information about characteristics of the household and health status of different age groups in different databases.
The anemia database for preschool children contains 7,570 children aged 12 to 59 months (representing 8,956,044 children using an expansion factor). This database was matched with a database of women by household ID and mother's ID number in order to obtain the mother's characteristics. In addition, preschool database was matched with food insecurity database of the ENSANUT 2012 using the same household ID number.
2.1. Description and construction of variables
Most of the variables used in this analysis are precalculated in the ENSANUT databases such as anemia, low weight for age, low weight for height, low height for age, overweight and obesity, and household food insecurity. According to the National Results Report of the ENSANUT 2012, nutrition indicators were calculated using World Health Organization criteria. In children 12-59 months of age, anemia is present when hemoglobin is <110 g/L. Adjustment by altitude >1,000 m above sea level was carried out using the formula of Cohen and Hass. Low weight for height, low weight for age and low height for age are those with Z scores below -2. Food insecurity was measured using the Latin American and Caribbean Household Food Security Scale (ELCSA, acronym in Spanish), based on the perceptions and experiences of the household informant.7
For mother's characteristics, a database of women was used to retrieve the following variables: indigenous, working status, head of household, and educational level. Teenage mothers are those <18 years of age at childbirth.
Quintiles and tertiles of SES are also precalculated in ENSANUT 2012 where SES was obtained by principal components analysis based on housing characteristics and menage. Rural areas are those localities with <2,500 people.
Iron supplement intake was obtained from the Nutrition and Food Distribution Programs database. The survey gathered information about whether the child received iron supplement in the last year and which public institution provided it. This does not include iron intake provided through food supplements that might have iron, administered by other public programs such as Oportunidades. In addition, it is not possible to know whether the child actually took it and for how long. In addition, it is not possible to know if the child is taking iron supplement obtained by private means.
Finally, social security affiliation includes all major social security institutions: IMSS (for private sector workers), ISSSTE (for public sector workers), PEMEX (Mexican petroleum enterprise) and armed forces social security. Seguro Popular is a program whose purpose is to extend health insurance and regular and preventive medical care to uninsured Mexicans, ∼50 million persons.
2.2. Statistical analysis
Frequency tables were calculated for preschool malnutrition prevalence by socioeconomic quintiles: anemia, low weight for height, low height for age, low weight for age and overweight and obesity. Anemia was also calculated by age group and socioeconomic tertile. Logistic regression models were estimated to obtain the risk of preschool anemia due to the following covariates: socioeconomic tertiles, urban and rural areas, child age and mother's characteristics such as educational level and employment. In addition, childhood anemia prevalence is presented by main variables used in the logistic regression model. All statistical analyses were carried out using SPSS 16.0.
3. Results
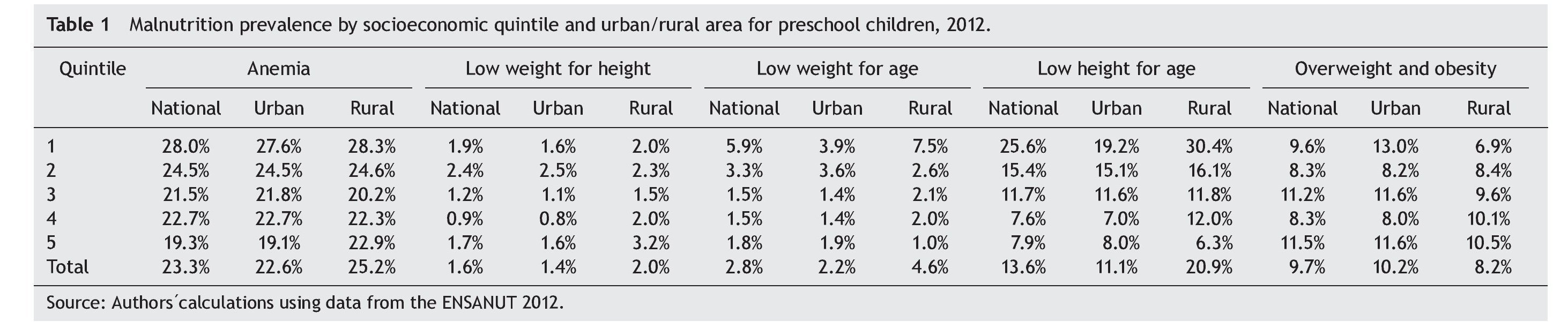
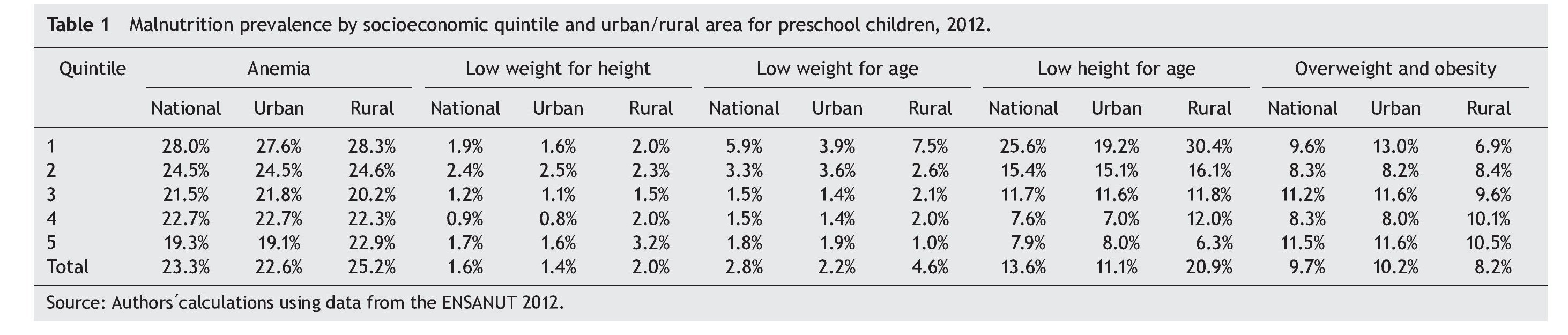
National prevalence of anemia in preschool-age children (1-5 years old) is 23.3%. Overall, undernutrition rates (measured by low weight for height, low height for age and low weight for age) are higher for rural areas, whereas overweight and obesity prevalence is higher in urban areas (Table 1). Undernutrition coexists with overweight and obesity in the same populations. Childhood undernutrition is concentrated in the lower SES except for anemia, where it is observed in all SES, although with a higher incidence in the lower SES groups. In quintile 1, anemia prevalence is 28.0%, whereas it is 19.3% in quintile 5, which means one in five children in the highest SES level has anemia.
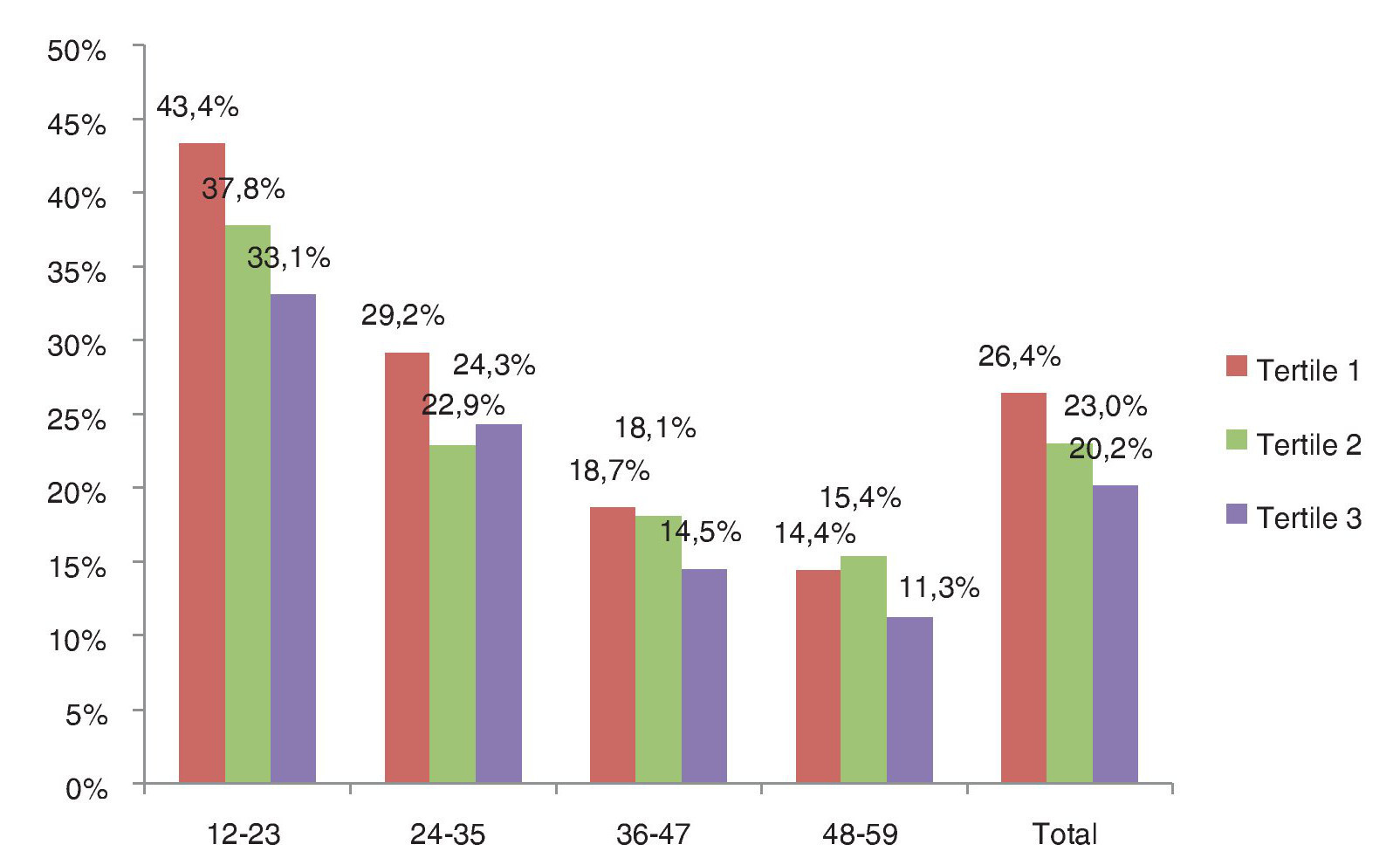
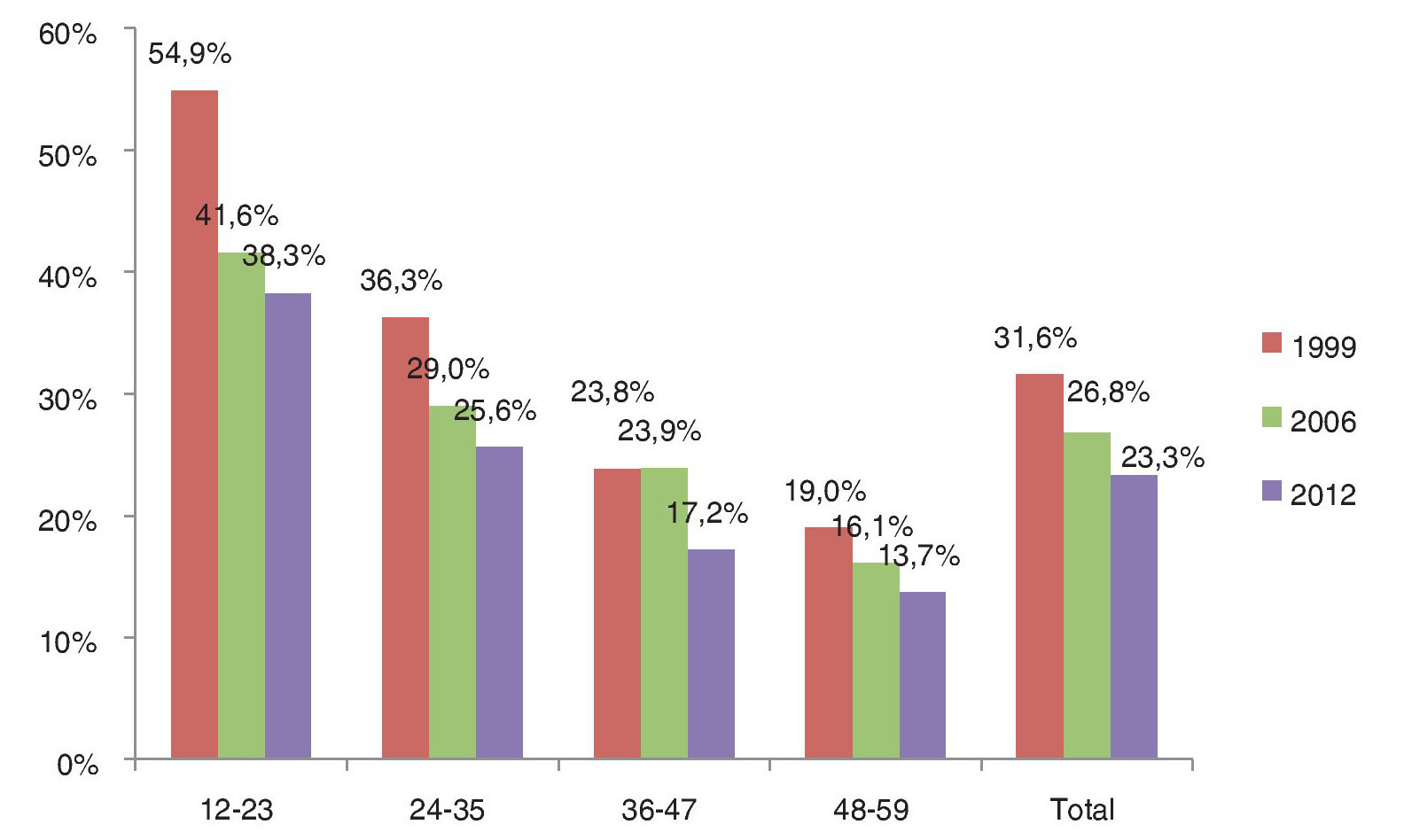
Anemia rate for children <5 years has decreased in the last 15 years, from 31.6% in 1999 to 26.8% in 2006 and 23.3% in 2012 (Fig. 1), although the rate is consistently higher in children <2 years regardless of SES tertile (Fig. 2). Anemia prevalence and the gap in this prevalence between the lower and higher SES decreases with age: for children between 12 and 23 months the gap between the higher and lower tertile is 11.3 pp, whereas for those 48 to 59 months it is 3.1 pp. Children <2 years of age have a higher risk of anemia due to an increased requirement of iron determined by growth. For this reason, we include a categorical variable for these children in the general model.
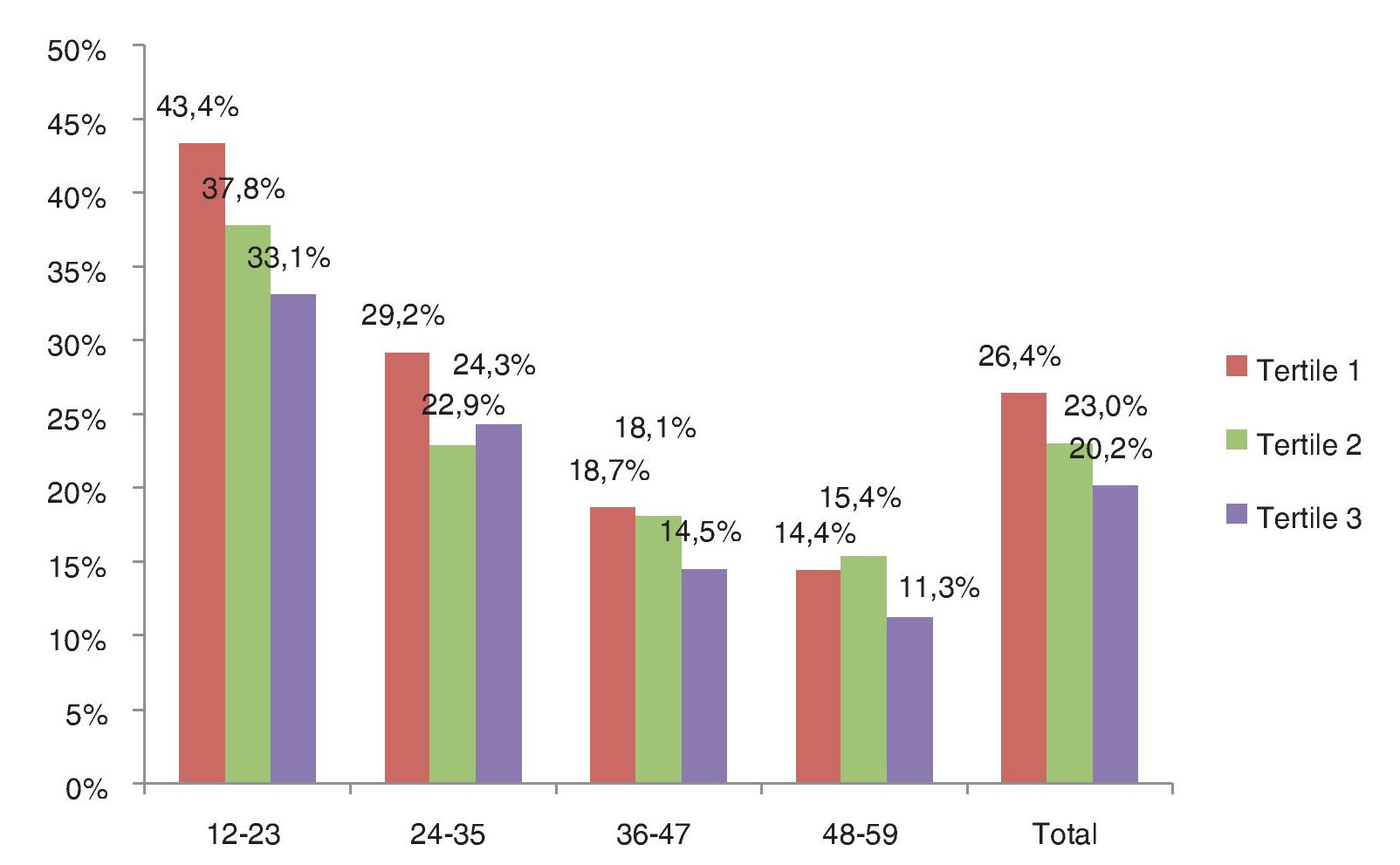
Figure 1 Anemia prevalence by age (in months), 1999, 2006 and 2012.
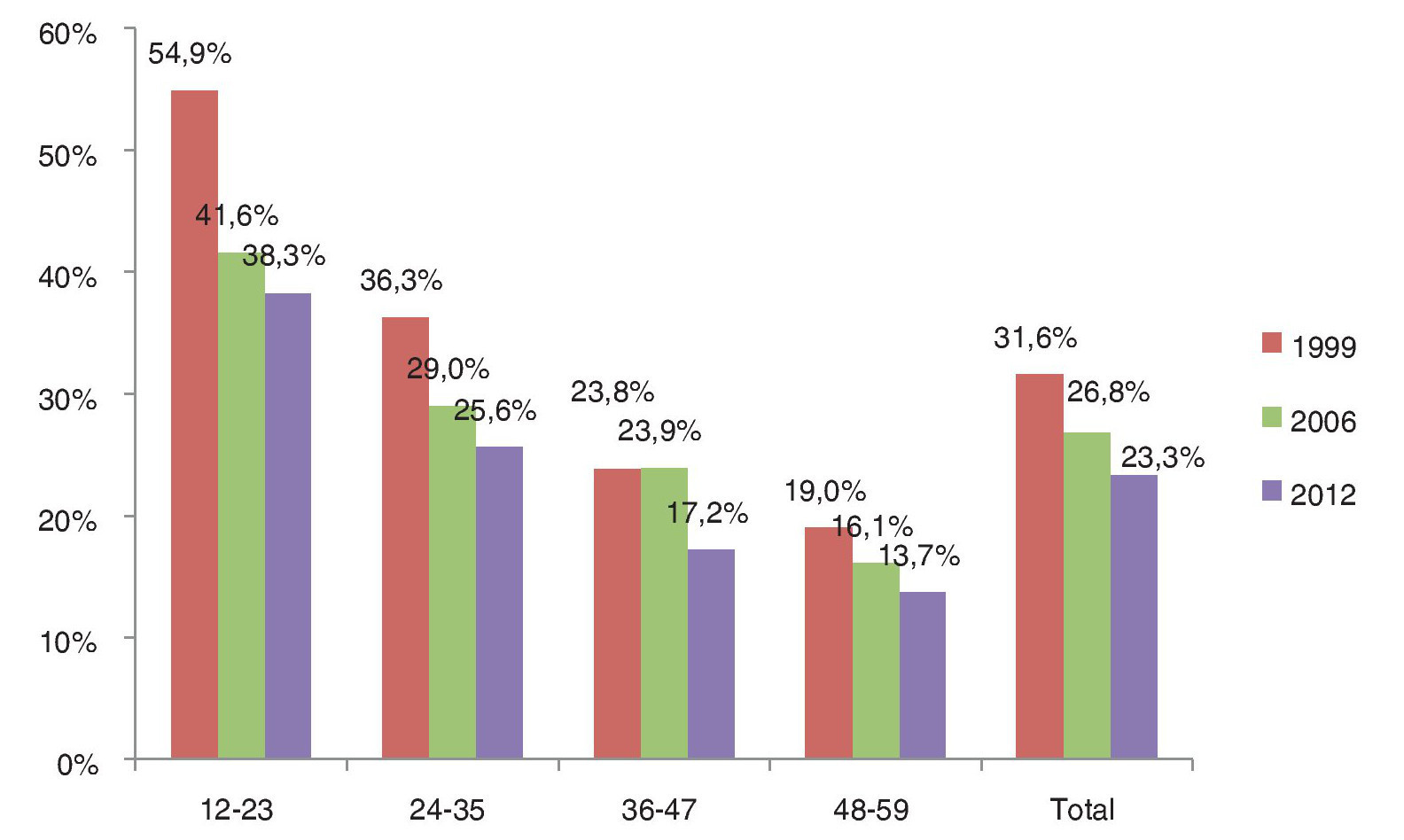
Figure 2 Anemia prevalence by age (in months) and socioeconomic tertile.
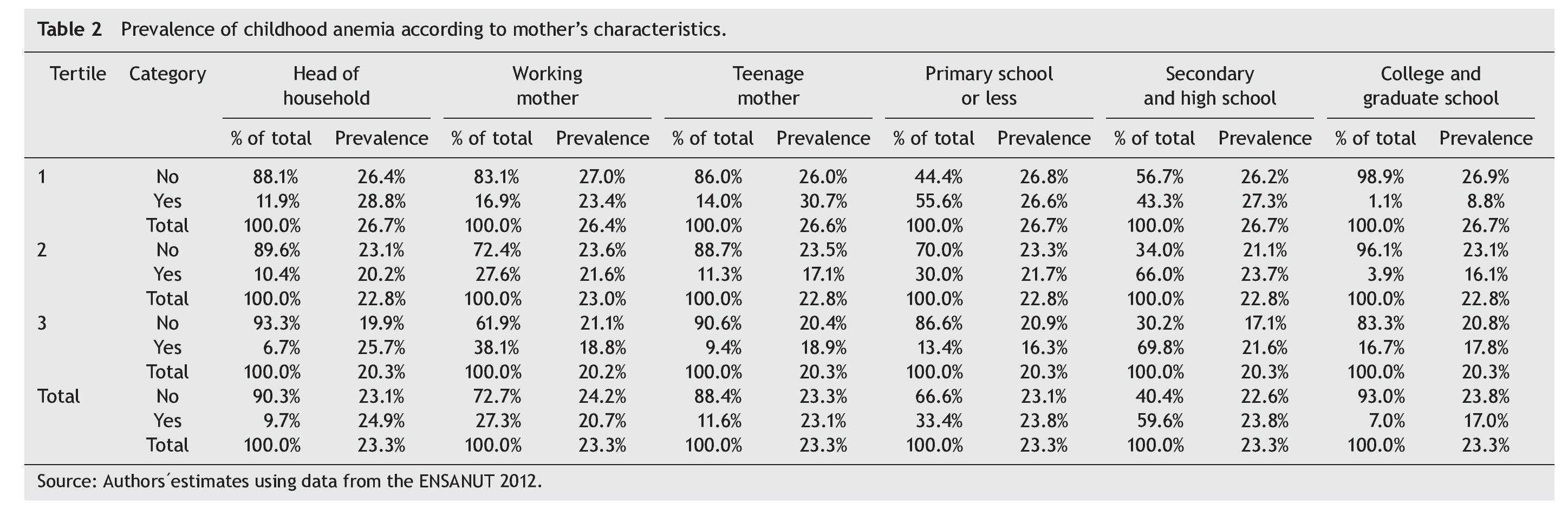
Mother's characteristics are important to explain childhood health conditions. Table 2 presents childhood anemia prevalence by the primary variables of the mother included in the logistic models. Nationwide, only 7.0% of mothers attended college or graduate school; this percentage is 1.1%, 3.9% and 16.7% for tertiles 1, 2 and 3, respectively. The prevalence of anemia is higher in children whose mothers have primary school or less compared to those whose mothers attended college or higher: 23.8% vs. 17.0%.
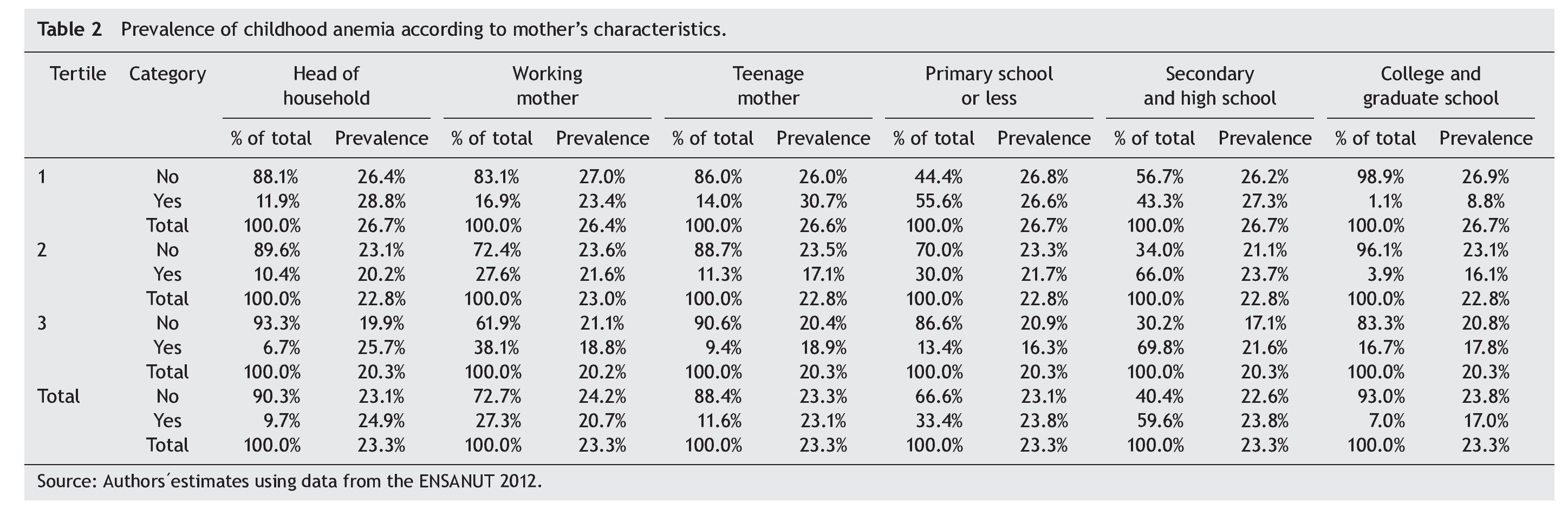
On the other hand, children of working mothers have a lower prevalence of childhood anemia regardless of SES tertile, probably due to their contribution to household income. However, women who are head of the household have higher rates of anemia (p value 0.000), which could be explained by the fact that they are less able to devote time to child care as they alone must support their family. In the logistic models, the heterogeneity of effects by working status and head of the household was tested with the aim of estimating the risk of childhood anemia where mothers are struggling with caring for and financially supporting their families without a partner. At a national level, children of teenage mothers have a similar prevalence of anemia than those of older mothers (23.1% vs. 23.3%); however, teenage mothers at the lowest SES tertile have a higher anemia rate (30.7%) than children of teenage mothers in tertiles 2 and 3 (17.1% and 18.9%, respectively).
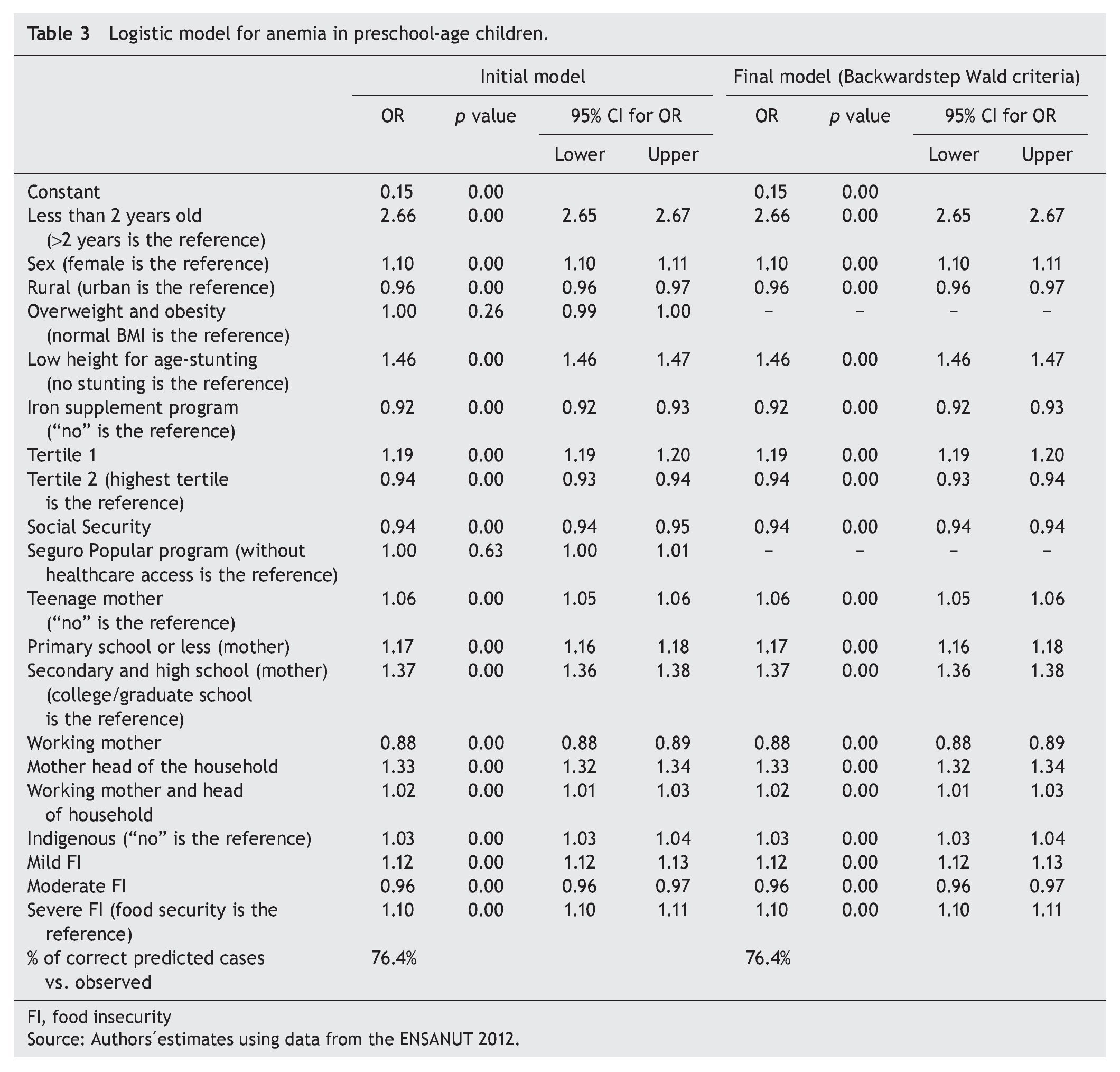
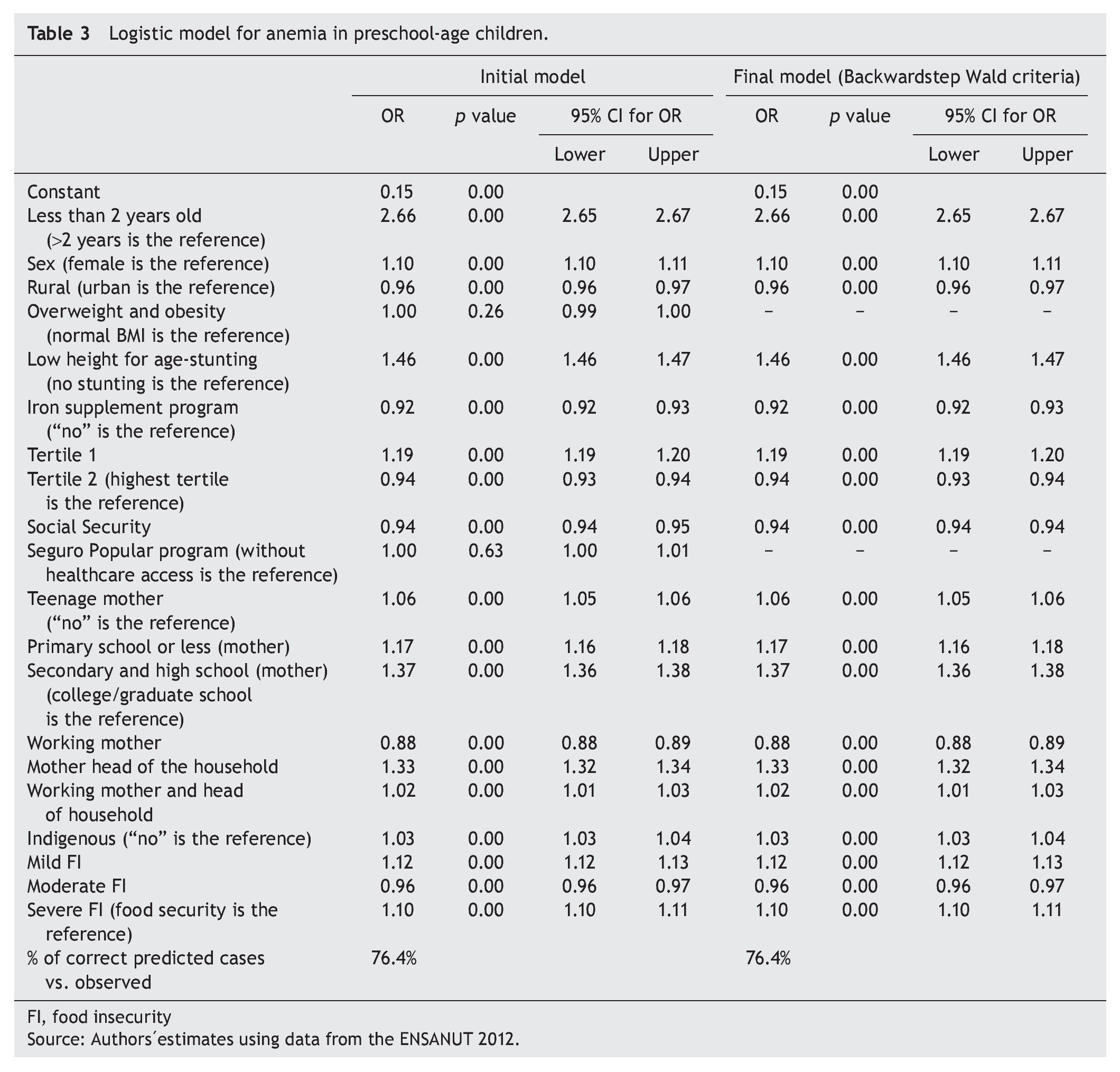
The general logistic regression model for all preschool children is presented in Table 3. Children <2 years have 2.66 times the risk of anemia compared to older preschool a higher risk of childhood anemia in households headed by women, as well as in those where women are at the same time working and head of the household. Children of indigenous mothers also have a higher risk, although the effect is small (3% higher risk than nonindigenous mothers). Mother's educational level is also important and has a negative relation with anemia. Children whose mothers have primary school or less have 17% more risk of anemia than those of mothers who attended college.
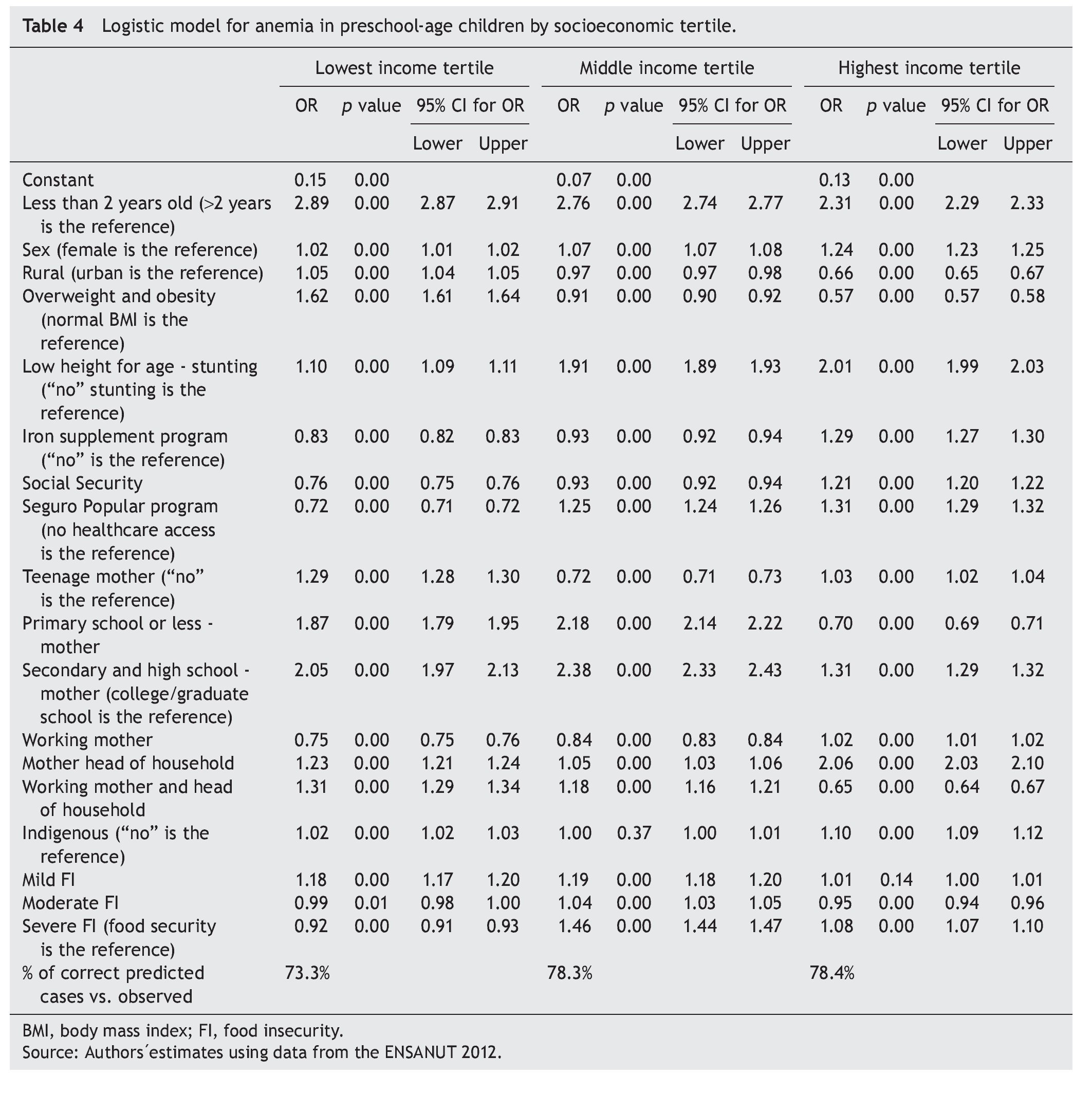
Children at the lowest SES tertile have more risk of anemia than the highest tertile as expected; however, it is noteworthy that middle tertile children have less risk than children at the top of the SES distribution. In order to assess differential effects of the covariates included in previous models on each SES tertile, we estimated a logistic regression model for each one. These models are presented in Table 4 and referred to as Model 1, Model 2 and Model 3 for the lowest, middle and highest SES tertile, respectively.
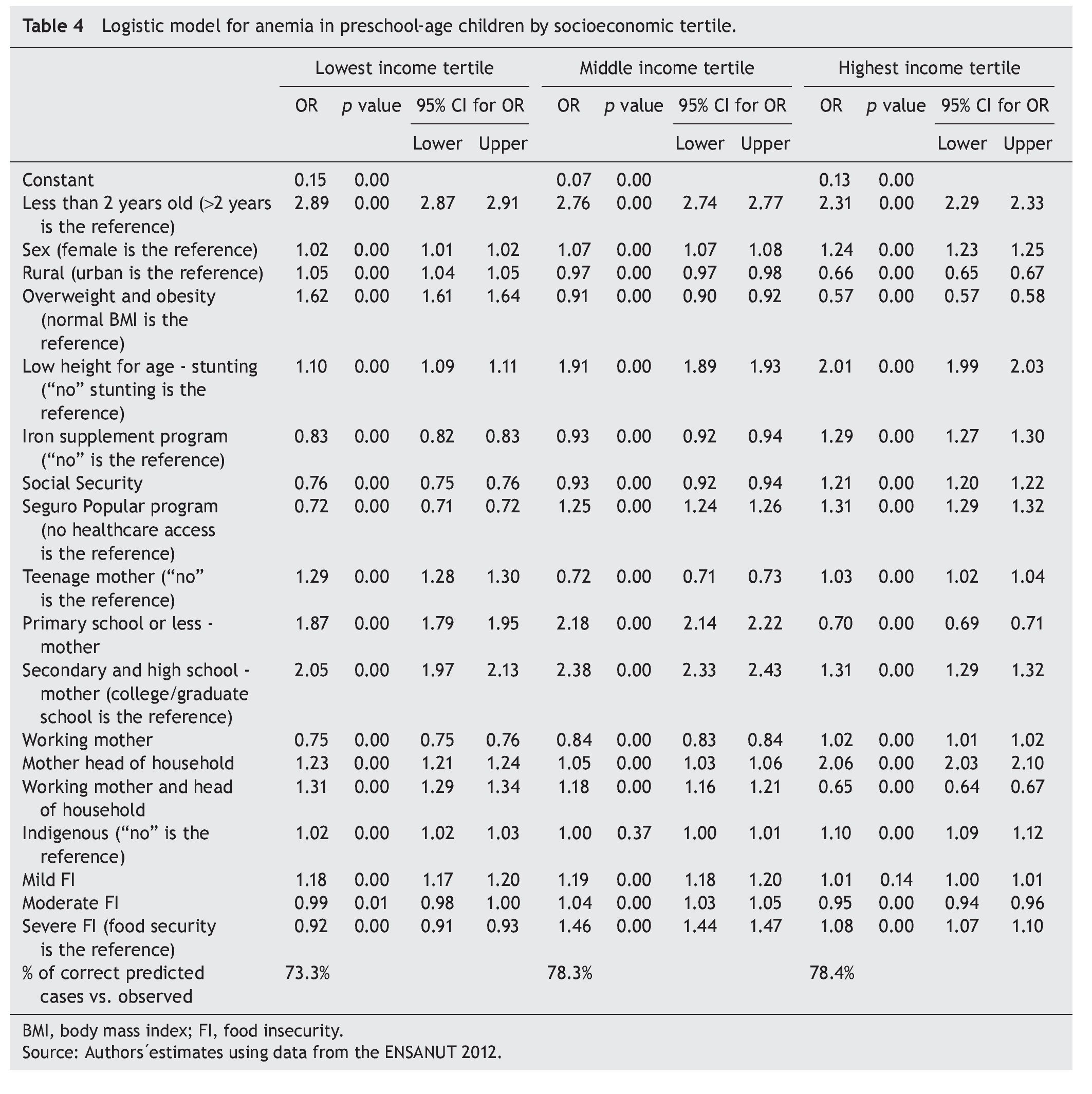
Some of the estimated effects for the lowest SES tertile are different from those for the middle and highest tertile, not only in magnitude but also with the opposite effect. Contrary to what was found in Model 2 and Model 3, in Model 1, living in rural areas is a factor risk for anemia (OR: 1.05, p value 0.00); as well as having a mother with a low educational level (OR: 1.87; p value 0.00). Being an overweight child is positively related to anemia in the lowest SES (OR: 1.62; p value: 0.00), whereas in other SES there is a negative relation between anemia and overweight because the OR is <1. One explanation for this result might be that poorer children have a diet with high caloric content but low in iron, whereas children in other SES could have high caloric intake as well as sufficient iron intake.
Other results for the poorer SES different from higher tertiles are as follows: i) iron supplement programs are a protection factor to anemia (OR: 0.83, p value 0.00); ii) affiliation to social security and Seguro Popular are negatively related to risk of anemia, which suggests that access to public health care is more relevant for poorer children than for children in higher SES; iii) working and head of household mother is a risk factor for anemia in poorer children.
On the other hand, it is important to mention the risk factors for anemia in the highest SES. A stunting child has twice the risk of anemia than a child of normal height for age. The positive relationship between anemia and the iron supplement programs can be explained by the fact that the child is provided with the iron supplement once diagnosed with anemia, not being the case for the poorest level, where provision of iron as a preventive measure is more widespread. Also children in households headed by mothers have a stronger risk for anemia for this SES (OR: 2.06, p value 0.00) than for those for lower SES (OR: 1.23 for the lowest and OR: 1.05 for the middle).
Finally, in the set of models by SES tertile, it is also important to mention the unexpected effects of food insecurity (FI). The expected results are OR >1 in all FI variables and increasing with severity of FI. However, according to Model 1, moderate and severe FI are negatively related with risk of anemia as OR are <1, whereas mild FI has an OR >1. In Model 2, all OR coefficients are >1, but moderate FI has less risk of anemia than mild FI. In Model 3, moderate FI has less risk of anemia than those children with children. Males have a higher risk of anemia than females. Odds ratio (OR) of rural areas is <1, which means that children in those regions have a protection factor compared to children in urban areas. This can be explained by the fact that government efforts have been concentrated on rural areas; indeed, 12.4% of rural and 9.2% of urban children received iron supplements by public institutions, according to ENSANUT. Furthermore, iron supplement programs have a negative relation to anemia because the OR is <1; this means that iron supplements are a protection factor against anemia. Social security affiliation is also a protection factor, whereas Seguro Popular program has no significant effect on anemia in preschool children.
Nationwide, overweight and obesity have no correlation with anemia prevalence, whereas there is a strong relation of anemia with stunting (low height for age); the risk of anemia is 46% higher for a child with stunting compared to a child of normal height.
The effects of mother's characteristics on anemia follow. Children of working mothers have less risk of anemia than nonworking women, probably due to their contribution to household income as previously mentioned. There is food security. These unexpected results are similar to those presented in Table 3 for the whole sample. One explanation might be the way FI is measured. Official results of FI using ENSANUT 2012 are different from those presented by Consejo Nacional de Evaluación de la Política de Desarrollo Social (CONEVAL), the official institution that measures poverty and inequality in Mexico, using the Socioeconomic Conditions Module from the National Survey of Households' Income and Expediture 2012 (MCS-ENIGH). ENSANUT and Coneval use different methodologies. For example, based on ENSANUT 2012, 70.0% of households experience FI, whereas using the MCS-ENIGH 2012 the proportion is 40.6%. A discussion of the differences is presented in Rodríguez and Pasillas.8
4. Conclusions
Anemia in preschool children is a public health problem present at all SES contrary to the generalized view that it is concentrated in lower income households. National prevalence of anemia in preschool children is 23.3%; in the lowest tertile it is 26.4%, whereas in the highest tertile it is 20.2%.
This paper presents some efforts to explain why anemia prevalence is high even in high SES. Logistic models were calculated for each SES tertile. Some of the estimated effects for the lowest SES tertile are different from those for the middle and highest tertile, not only in magnitude but also with opposite factors such as rural area and mother's educational level.
Another important result is that being an overweight child is positively related to anemia in the lowest SES, this not being the case in the upper SES. One explanation might be that poorer children have access to a diet with high caloric content but low in iron, except for those who are beneficiaries of Oportunidades and receive and take regularly food supplements, whereas children in other SES may have high caloric diet but with sufficient iron intake. Given the significant coverage and budget allocated to food programs targeted to the poor in Mexico, it would be important to evaluate whether they are contributing, positively or negatively, to this phenomenon.
Variables related to increased risk of anemia in the highest tertile are as follows: male children (OR: 1.24), those <2 years of age (OR: 2.31), stunting (OR: 2.01), and mother as head of the household (OR: 2.06).
A general strategy is required to reduce the rate of children with anemia rather than only the targeted efforts followed so far. In addition, there is a need for additional research to explain the high prevalence in wealthier households.
Funding
There was no financing for the realization of this study.
Conflict of interest
The authors declare no conflict of interest of any nature. ENSANUT 2012 is a survey of public use.
☆ The findings, interpretations and conclusions expressed in this paper are entirely those of the authors. They do not necessarily represent the view of the Hospital Infantil de México Federico Gómez.
Received 10 February 2014;
accepted 14 February 2014
* Corresponding author.
E-mail:evelyne_rodriguez@hotmail.com (E.E. Rodríguez-Ortega).