



The Hospital Infantil de México Federico Gómez is a tertiary level hospital with a neonatal intensive care unit (NICU), which is one of the most important units in the treatment of newborn's diseases in Mexico. In this unit, decisions are made based on some clinic parameters, such as respiratory rate, heart rate, arterial pressure, urinary output, and lactate levels. The functional echocardiography is a useful tool, which improves the hemodynamic evaluation and decisions in neonatal care. Data on its use NICU in Mexico is insufficient.
MethodsA prospective study was conducted in NICU patients during 3 months, from August to October 2015, at the Hospital Infantil de México Federico Gómez. Gestational age, birth weight, admission criteria, days of life at examination, indication for functional echocardiography and changes in treatment were evaluated. Finally, a new study 24hours later was performed. The echocardiographic evaluation included assessment of presence/hemodynamic significance of PDA; myocardial function: ejection fraction/shortening fraction, left ventricular output, right ventricular output, systemic blood flow; and signs of pulmonary hypertension.
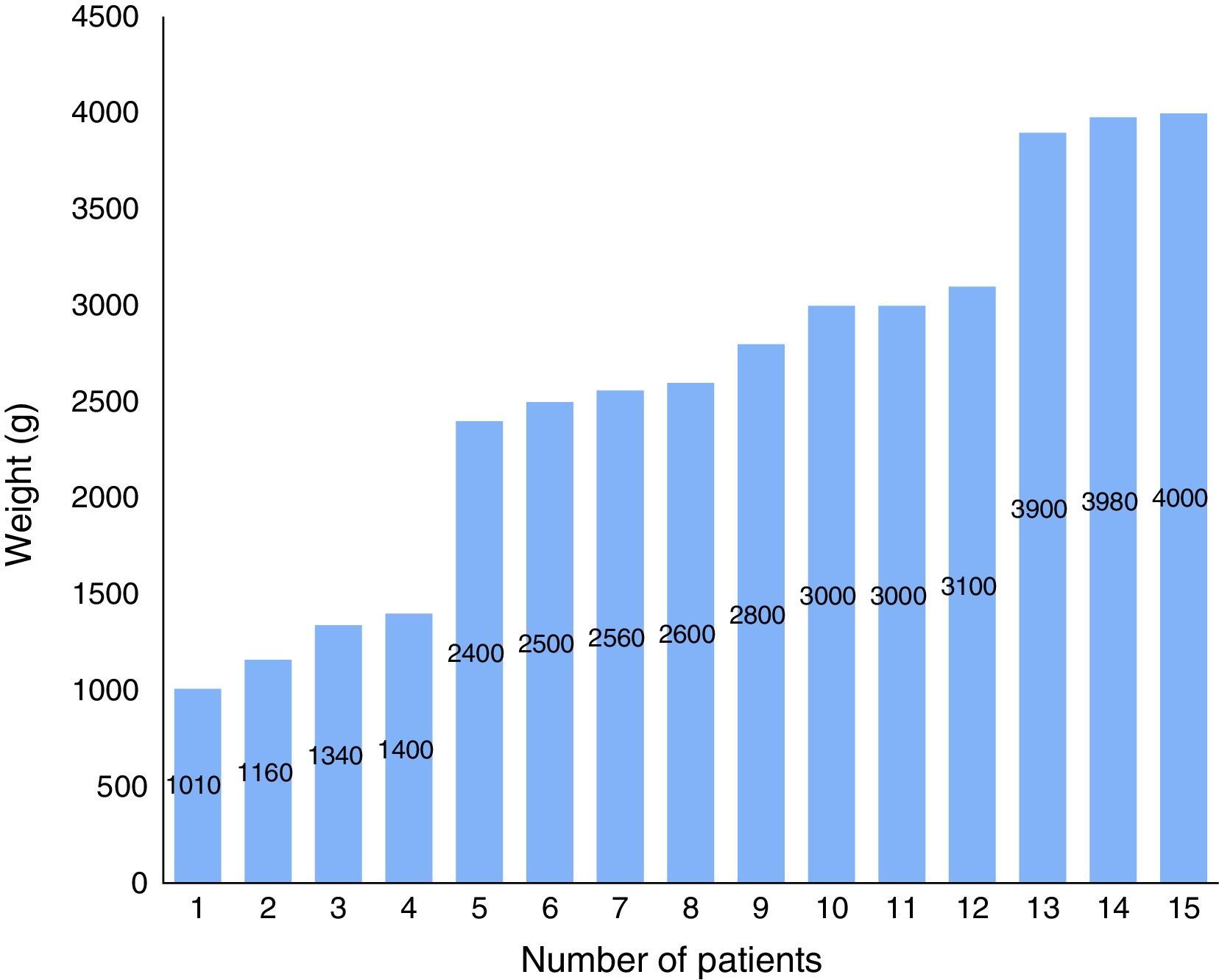
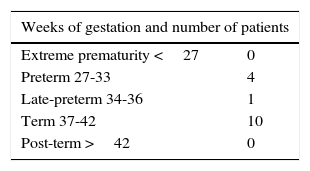
ResultsEchocardiographic studies (30) were performed in 15 patients. The average age was 9.6 days, the variability in gestational ages were 37 to 42 weeks; the average weight was 2583g. The most frequent diagnosis was respiratory distress, and the principal indications for echocardiography were hemodynamic instability and sepsis (53.3%). In 11 cases (73.3%), the treatment was modified after functional echocardiography and in 10 cases improvements were observed in the 24hours after control.
ConclusionsFunctional echocardiography is a useful tool in NICU, which may assist the clinical decision-making.
El Hospital Infantil de México es un hospital de tercer nivel y centro de referencia nacional que cuenta con una unidad de cuidados intensivos neonatales (UCIN), en la cual la toma de decisiones se realiza con base en parámetros clínicos y datos como la frecuencia respiratoria, frecuencia cardiaca, tensión arterial, gasto urinario y nivel de lactato. El ecocardiograma funcional (EcoF) es un estudio que permite complementar los datos hemodinámicos de estos pacientes, logrando una integración de parámetros clínicos y hemodinámicos con el objetivo de mejorar las decisiones terapéuticas y la evolución de los pacientes.
MetodologíaEstudio descriptivo prospectivo sobre la implementación del EcoF en pacientes de la UCIN durante el periodo de agosto a octubre del 2015 en el Hospital Infantil de México Federico Gómez. Las variables fueron la edad gestacional, los diagnósticos de ingreso, el peso, las indicaciones para realizar el estudio y los días de vida en el momento del estudio. En cada estudio se determinaron los parámetros ecocardiográficos que conforman el EcoF, se anotaron las modificaciones al tratamiento posterior al estudio y se realizó un nuevo control a las 24 horas para determinar la evolución del paciente.
ResultadosSe realizaron un total de 30 estudios en 15 pacientes durante el periodo previamente señalado. La media de edad a la que se realizó el estudio ecocardiográfico fue de 9.6 días de vida (2-28 días). En el 66%, el rango de semanas de gestación fue entre 37 y 42, con una media de peso de 2583g (1010-4000g). El diagnóstico más frecuente fue el síndrome de dificultad respiratoria y prematurez (26.6%). La indicación más frecuente para solicitar el estudio fue la inestabilidad hemodinámica y sepsis, representando el 53.3%.
En 11 pacientes (73.3%) hubo modificaciones al tratamiento posterior al EcoF, con mejoría en 10 casos en el control que se realizó a las 24 horas.
ConclusionesLa EcoF es una herramienta útil en UCIN, ya que aporta información complementaria que apoya las decisiones terapéuticas. Hace falta la diseminación de programas de formación y acreditación conforme a las recomendaciones existentes para asegurar un uso correcto y seguro de esta técnica.
One of the main limitations about care and decision-making in the neonatal intensive care unit (NICU) is the lack of cardiovascular function and hemodynamic parameters in comparison with those of adult intensive care. NICU principal hemodynamic parameters are the blood pressure (BP), heart rate (HR), capillary filling, urine output (UO), and hyperlactatemia. However, the use of these indirect measurements to assess tissue perfusion is very inaccurate, especially in pre-term patients due to the complex hemodynamic changes occur during the first days of life1.
BP is the most used indicator to assess hemodynamic status in the neonate. Osborn studied the accuracy of the mean arterial BP on gestational age to detect low systemic blood flow (SBF) based on the flow of the superior vena cava (SVC) in preterm neonates, and identified <30% of neonates in shock. Currently, evidence of a non-linear relationship between the BP and the SBF exists. The HR was considered a fixed value in neonates, and it was contemplated that cardiac output (CO) was entirely dependent on it. Nevertheless, some studies in which infants with and without hypotension were compared, no significant differences in HR were found, showing that no linear correlation between SBF and HR exists.
The UO is hard to assess in the early days of the extrauterine life since there is initially a low urine output phase (first 24hours) and a subsequent phase of temporary polyuria (2nd and 3rd day). Lactate synthesis increases when a critical level of hypoxia is reached and maximum oxygen extraction is insufficient for the metabolic demand. It is a poor prognosis parameter when serial measurements are made2.
Despite its poor accuracy, clinical assessment remains the most widely used hemodynamic monitoring method, meaning that only a small portion of infants with low SBF will be detected. The poor predictive values of individual clinical markers emphasize the need for alternative ways to have a reliable measure of neonatal cardiovascular function.
Echocardiography performed to a newborn by the cardiologist usually has the objective of ruling out heart disease and assessing cardiac function. About ten years ago, the term functional echocardiography (FEco) was introduced to describe the use of echocardiography as a support tool in the decision-making and monitoring hemodynamics in neonates at risk of cardiac dysfunction. In Australia, Dr. Evans was one of the pioneers in this technique. FEco shows qualitative and quantitative information by echocardiography conventional methods. It can determine the presence and impact of a ductus arteriosus, the pathophysiology on conditions of hemodynamic instability or high oxygen requirements, the assessment the myocardial function on both ventricles to rule out pulmonary hypertension and to determine the cardiac index. Currently, new groundbreaking methods are being implemented, such as the 3D echocardiography and color tissue Doppler velocity imaging3.
In 1996, Oliva et al. conducted a study in which they tried to standardize an assessment technique for the first time in Mexico, by studying 58 infants divided into two groups: one of healthy neonates and another of patients with a history of a perinatal disease. In both groups, systolic, diastolic and mean pulmonary pressure were determined with speed and gradient of the pulmonary artery. It was determined that the last group had pulmonary hypertension the first 15 days of life with a trend towards normalization at 30 days of life4.
As for worldwide experience, different publications have been reported. In Spain, a one-year experience in a NICU showed 168 studies performed in 50 patients with 36.9% of treatment modifications, in which it was concluded that FEco is a study frequently used in neonates with hemodynamic instability that helps to determine their management5.
In India, Anilkumar et al. described the experience and impact of FEco in a tertiary care center from February 2014 to January 2015, describing the frequency of use, patient characteristics and indications. The authors reported a total of 348 studies performed in 187 infants, of which the most frequent indication was patent ductus arteriosus (PDA)6.
This study aimed to describe the first experience of using the FEco in the NICU of a tertiary care hospital in Mexico over a period of three months.
2MethodsA descriptive prospective study on the implementation of the FEco in NICU patients was conducted from August 2015 to October 2015 at the Hospital Infantil de México Federico Gómez. The same physician at the pediatric echocardiography service performed all the studies. As per physicians responsible for the patients, all assessments and echocardiographic measurements were accomplished using the standard procedures described in Table 1.
Functional echocardiography parameters.
| Parameter evaluated | Mode |
|---|---|
| Assessment of the persistence of the ductus arteriosus | 2D/color doppler/pulsed wave doppler/M-mode |
| Diameter (narrowest dimension of duct) | |
| Ductal velocity | |
| Left atrial radius/aortic root | |
| Mitral E/a | |
| Left ventricle systolic and diastolic function | M-mode |
| Shortening fraction | |
| Ejection fraction | |
| Pulmonary pressure | Continuous wave doppler |
| Gradient of tricuspid insufficiency | |
| Interatrial communication | 2D/color doppler |
| Left ventricular cardiac index | 2D/M-mode/pulsed wave doppler |
| Left ventricular outflow tract diameter | |
| Velocity–time integral of PW in LV outflow tract | |
| Right ventricular cardiac index | 2D/M-mode/pulsed wave doppler |
| RV outflow tract diameter | |
| Velocity–time integral of PW in RV outflow tract | |
| Superior vena cava flow | M-mode/pulsed wave doppler |
| Systolic diameter | |
| Diastolic diameter | |
| Assessment of the right ventricle | M-mode |
| Tricuspid annular plane systolic excursion (TAPSE) |
The following general patient data were collected: gestational age, weight, age, body surface area, primary diagnosis, and study indication. The following clinical data were recorded at the time of completion of study: heart rate, respiratory rate, oxygen saturation, blood pressure, lactate blood levels (mmol/l) and the presence of oliguria (urine output <1ml/kg/h).
Data from echocardiographic studies included days of life at the time of the research and the study indication. The results were recorded in a special format added to the clinical record of each patient. After the study, the results were discussed with the responsible physicians to decide the appropriate treatment. Changes in the treatment after the study were determined as the following:
- 1
To increase fluid intake
- 2
To decrease fluid intake
- 3
To start or increase amine management
- 4
To initiate steroids
- 5
To suspend amine management
- 6
To increase ventilation parameters
- 7
To decrease ventilation parameters
- 8
No changes
Finally, a re-assessment was performed 24hours after the study, to determine if there were parameter improvements.
All studies were conducted with a SIEMENS Acuson X300 echocardiogram with a neonatal probe 5-8MHz. Echocardiographic assessment included the following aspects: PDA presence and consequences (diameter, shunt speed and direction, ratio of left atrium to aorta and mitral E/A); diastolic and systolic left ventricular (LV) function (ejection fraction, shortening fraction); pulmonary pressure (measured by the gradient of tricuspid insufficiency or ductus arteriosus gradient); interatrial communication presence; LV cardiac index (estimating the LV outflow tract [LVOT] diameter and the velocity–time integral [VTI]); right ventricle (RV) cardiac index (calculating the RV outflow tract [RVOT] diameter and the VTI); superior vena cava flow (diameter of the superior vena cava and VTI); assessment of RV function (TAPSE) and further changes the study and the subsequent evolution.
The qualitative variables are described as frequencies and the qualitative, as mean or median.
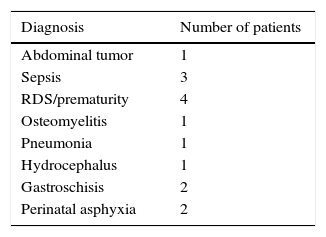
3ResultsA total of 30 scans were performed in 15 patients in a three-month period, with a mean of two studies by patient. The general characteristics of the patients were collected. The mean age was 9.6 days old (range between 2-28 days). Ten patients (66%) were in the range between 37 and 42 weeks of gestation, and 26.6% were <33 weeks of gestation (Table 2). The mean weight was 2583g (1010-4000g) (Figure 1). The most frequent diagnosis was neonatal respiratory distress syndrome and prematurity (26.6%). Other admission diagnoses were sepsis (20%), perinatal asphyxia (13.3%), and gastroschisis (13.3%) (Table 3). The most frequent FEco indications were hemodynamic instability and sepsis (53.3%), followed by the discard of a PDA (20%), history of perinatal asphyxia (20%), and the discard of pulmonary hypertension (6.6%). After the FEco, three patients with PDA were reported: one case with moderate PDA and two cases with severe PDA.

Concerning the impact of performing a FEco on the management of patients, it was observed that in 11 patients (73.3%) the treatment was modified after the FEco. In eight patients, modifications consisted in decreasing ventilation parameters; in three patients, fluid administration was decreased; this group included patients with PDA. In the treatment of the remaining four patients (27%), no further changes were made.
During the re-assessment, 24hours later, clinical improvement was reported in ten patients from the group with therapy modifications, which included pulmonary pressure reduction, improvement in sisto-diastolic function of the LV and cardiac indexes. Despite the treatment changes, the patient with severe PDA showed deterioration which led to a surgical intervention for closure. In the group of patients with no treatment changes, three patients with similar echocardiographic parameters showed no modifications in their evolution and one patient showed improvement.
4DiscussionTo the extent of our knowledge, this study describes for the first time the use of FEco in the NICU of a Mexican tertiary care hospital. It is demonstrated that this diagnostic tool was clinically useful as a complement of the hemodynamic assessment. Although there is no warrant that the results of FEco were the principal motives for the treatment modification, they supported the analysis and therapeutic action in a significant percentage of the cases.
Neonatologists confirmed their interest in FEco, promoting its acceptance and progressive implementation in the NICU. Ten years ago, in Australia and New Zealand, studies showed that 40% of the NICUs have at least one neonatologist trained in FEco. In 2010, this percentage increased to 90%7.
In the present study, the reasons why neonatologists requested the FEco are similar to those reports in Spain and India, where the most frequent indication was to discard the PDA, followed by hemodynamic instability5,6.
As for the percentage of post-FEco treatment modification, a high proportion (73.3%) was reported compared with 36.9% of the experience in Spain5, 42.5% in a tertiary care hospital in India6, and 41% reported by El-Kuffash et al. in Canada8. However, it should be considered that these previous studies are retrospective and include a greater number of cases ranging from one to four years. Furthermore, they recognized the need for prospective studies in their conclusions.
Despite the explicit advantage of this technique, there is still no evidence of a positive impact of FEco in the prognosis of patients in the NICU. In this study, 15 cases were analyzed, and despite the high percentage of treatment modification and improvement, it is not possible to assert a clear impact of FEco. However, the follow-up of these patients and the continuity of this project could show more evidence on the impact of FEco, as it has been shown by several retrospective studies and some clinical trials9–12.
The limitations of this study mainly derived from the few number of reported patients. No micro preemie patients (< 1000g) were included, and the neonatologist in charge of the patients decided on the treatment modifications and not only on data provided by the FEco, which could have significantly changed the perception of the influence of this technique on handling newborns.
In conclusion, FEco is a useful tool frequently used in the NICU, which provides additional information to aid the clinician in making treatment decisions. Therefore, its use is spreading in neonatology units, although clinical trials are needed to determine the impact of FEco on the prognosis of the patients. Structured training and accreditation programs under the existing recommendations are needed to ensure the correct and safe use of this technique.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestThe authors declare no conflicts of interest of any nature.
Please cite this article as: Hernández-Benítez R, Becerra-Becerra R. Ecocardiografía funcional en cuidados intensivos neonatales: experiencia en un hospital de tercer nivel. Bol Med Hosp Infant Mex. 2016;73:325–330.