

Functional gastrointestinal disorders (FGIDs) are highly prevalent worldwide and are thought to result from the interplay of multiple factors that can vary from region to region. Nationwide studies can help understand the regional epidemiology and the pathogenesis of FGIDs. The objectives of this study were to determine the prevalence of FGIDs in school-children of Colombia and assess associated factors.
MethodsA cross-sectional study was carried out at twelve private and public schools in ten cities distributed through the four main geographic regions of Colombia. School-children completed a validated questionnaire to assess functional gastrointestinal disorders according to Rome III criteria. Demographic information and past medical and family history was obtained from the parents.
ResultsA total of 4394/5062 (86.8%) children participated in the study, with ages ranging from 8-18 years (mean = 11.9, SD = 2.3). The percentage of children with al least on FGID was 23.7%. Disorders of defecation were the most common category FGID (11.7%) followed by abdominal pain related-functional gastrointestinal disorders (10.4%). Children have increased odds of FGIDs if they have separated parents (OR 1.22, P=0.007), attend private school (OR 1.54, P<0.001), or have nausea (OR 3.16, P<0.001).
ConclusionsThis large epidemiological study of pediatric FGIDs is the first to evaluate a broad cross-section of children throughout a nation in the Americas. High prevalence of FGIDs and identified associations with their likelihood are relevant when providing medical care and when planning public health efforts.
Los desórdenes gastrointestinales funcionales (DGF) son altamente prevalentes a nivel mundial. Se postula que estos desórdenes resultan del interjuego de múltiples factores que pueden variar regionalmente. Estudios a nivel nacional pueden ayudar a comprender la epidemiología regional y la patogénesis de los DGFs. Los objetivos del estudio fueron determinar la prevalencia de DGFs en escolares en Colombia y establecer los factores asociados.
MétodosEstudio de corte transversal realizado en 12 escuelas privadas y públicas en 10 ciudades de las cuatro regiones principales de Colombia. Niños de edad escolar completaron un cuestionario validado para diagnosticar DGFs de acuerdo con los criterios de Roma III. Información demográfica e historia personal y familiar fue obtenida de los padres.
ResultadosUn total de 4394/5062 (86.8%) niños participaron en el estudio, rango de edad 8-18 años (promedio = 11.9, desviación estándar (DE) = 2.3). El 23.7% de los niños tuvieron al menos un DGF. Los desórdenes de la defecación fueron los más frecuentes (11.7%), seguidos por desórdenes funcionales de dolor (10.4%). Niños cuyos padres estaban separados (razón de momios (RM) 1.22, p= 0.007), cursaban en escuela privada (RM 1.54, p< 0.001) o reportaban náuseas (RM 3.16, p< 0.001) tuvieron mayor riesgo de DGFs.
ConclusionesEste estudio de DGF es el primero en evaluar un grupo numeroso de niños en diferentes regiones de un país americano. La alta prevalencia de DGFs y la identificación de asociaciones que aumentan el riesgo de desarrollar estos desórdenes son hallazgos relevantes para proveer cuidados médicos y planear estrategias de salud pública.
Thirty-eight percent of school-children report abdominal pain weekly,1but only 2-4% of children who report abdominal pain seek medical consultation.1,2 Despite this, abdominal pain is the most common cause of consultation to the pediatric gastroenterologist. Out of all children (> 4 years) who consulted pediatric gastroenterology in a tertiary care center in the US, 52% of them consulted for an abdominal pain associated-functional gastrointestinal disorder (AP-FGID).3The cost of care of children with AP-FGIDs is substantial. In the Netherlands, the costs of care for a child with AP-FGIDs exceeds €2500.4 The overall cost of care for AP-FGIDs in the US grew by 300% in a 12 year period5 and evaluation of a single child for an AP-FGIDs in the US is estimated > $6000.6 The cost of a single consultation for abdominal pain in Uruguay accounted for 3.8% of the per capita health care spending of one year.7Although, the economic impact of AP-FGIDs has not been studied in most countries, based on the high worldwide prevalence of FGIDs it is likely to be a global economic problem.
The magnitude of the problem calls for preventative measures and plans of care adapted to local needs. However, in order to establish what the local needs are, it is imperative to first obtain reliable data on the local epidemiology. Due to the low ratio of consultation for abdominal pain, studies performed at the doctor's office are prone to selection bias. Thus, only community studies provide the information needed. Conducting epidemiological studies in private and public schools allows obtaining data from children with different socio-economic statuses. There have been several school studies investigating the prevalence of FGIDs, however none of them were conducted in private and public schools in multiple cities throughout different regions of one country.
In addition to establishing the regional epidemiology, nationwide studies provide a unique opportunity to achieve a better understanding of the pathogenesis of FGIDs that is currently elusive. This information is key to establish prevention strategies and effective treatments. The most accepted model to explain FGIDs propose that these disorders result from the interaction of the child's genetic background, early life experiences, intestinal microbiota, psychological, and social influences. As these factors vary by region, establishing comparisons among regions could help advance the knowledge of the pathogenesis of FGIDs.
We conducted a large school-based study of FGIDs in multiple cities in Colombia using standardized methods, validated questionnaires adapted to the terms used by children, and the Rome III diagnostic criteria. The aims of this study were to evaluate prevalence of pediatric FGIDs throughout Colombia, determine if regional differences exist, and identify associated factors.
2MethodsThis is the largest study conducted by the Functional International Digestive Epidemiological Research Survey (FINDERS) group and the broadest national study in the Western Hemisphere on FGIDs in children. This cross-sectional study was carried out at 12 schools in 10 cities of Colombia. Colombia is the second most populated country in South-America with a population of approximately 50 million8 inhabitants. Most of the population is concentrated along the Caribbean coast and the Andean regions. In Colombia, 85% of primary care education students and 60% of the secondary-school level students attend public schools.9 To enhance racial, ethnic, and socioeconomic diversity and maximize the external validity of the data, we selected public and private schools as study sites. The study was purposefully designed to enroll a higher proportion of children from public than private schools to resemble the education system of the country. To better represent the population distribution of Colombia, we selected more cities with high population density than low. The cities of the study are distributed through the four main regions of Colombia, the Caribbean region (adjacent to the Caribbean Sea), Andean region (by the mountains), the Amazon region (tropical rainforest), and the Pacific region (neighboring the Pacific Ocean). Together these four regions hold 97.3% of the population in Colombia.
To ensure consistency and to allow comparison within multi-national cross-cultural studies, the study was conducted in a systematic manner following the same methods used in previous studies by the international consortium FINDERS.1,10–12The methods used by FINDERS were based on two school studies performed previously and a prior small study by FINDERS in Colombia. The first study was piloted in a single school in Pittsburgh13 followed by a larger study in Chicago to streamline methods.2 Planning of the current study in Colombia started by translating the English version of the QPGS-III questionnaire into Spanish and local language according to established standards. The self-report child version of the QPGS-III questionnaire (a validated instrument created to assess the full spectrum of FGIDs according to the Rome III criteria) was first translated into Spanish by a bilingual pediatric gastroenterologist and two bilingual medical students. This was followed by the reverse translation of the QPGS-III by another member of the research team. The resulting English version was then compared with the original English version of the QPGS-III by a native English speaker who was not part of the research team to ascertain fidelity. The finalized Spanish version of the QPGS-III was then presented to two focus groups of children in two different cities in Colombia (Cali and Pasto) to ensure terms were adequately understood. Once the Spanish version of the QPGS-III was tested in the focus groups, the methods and the Spanish version of the questionnaire were again tested in the first study by FINDERS in Pasto, Colombia.1The data obtained from this study using the Spanish version of the QPGS III were analyzed statistically for internal consistency using Cronbach's alpha analysis.14The study showed high internal consistency. In short, the methods used in the current study were the following: parents of children 8-18 years of age received a package with information on the study at home, a questionnaire on their child's past medical history and a consent form. Children who assented (and whose parents consented) to participate in the study underwent an informative session in class explaining the study and questionnaires. The participants then completed the data forms in class with a member of the research team available for questions. The data was entered into an electronic database. In order to ensure accuracy of data transfer, 10% of the questionnaires were reviewed and compared with the paper forms collected at the school level.
The study was approved by the principal of each of the schools and by the Institutional Review Board and Human Subjects Committee of Universidad del Valle of Cali, Colombia
Statistical analysis included calculation of odds ratios, 95% confidence intervals, and p values to describe the associations of interest (Stata 10 software, College Station, Texas). Fisher's exact test was used when appropriate. Two-sided p values <0.05 were considered statistically significant.
3ResultsA total of 5062 school-children's families were sent the information package and invited to participate in the study. 4394/5062 (86.8%) dyads (children/caretaker) assented/consented to participate. Participants ranged from 8 to 18 years of age (mean = 11.9, SD = 2.3). There were 2279 males (51.9%) and 2115 (48.1%) females; 2702 (61.5%) were children (8 to 12 years) and 1692 (38.5%) adolescents (13 to 18 years). Most children who participated in the study were from public schools 3546 (80.7%) and 848 (19.3%) were from private schools.
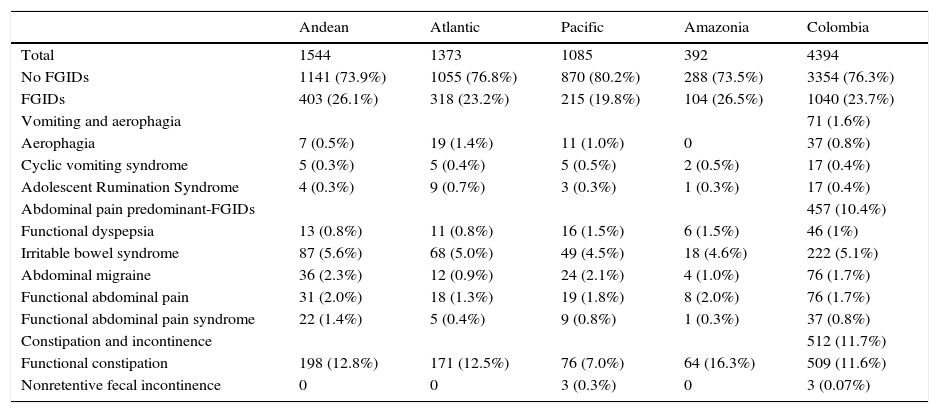
3.1FGID prevalenceIn the total sample, 23.7% of children had at least one FGID. The range of FGID per region varied between 19.8% (Pacific region) to 26.5% (Amazonia region). There was a significant difference in FGID prevalence between regions (p= 0.001). Additional analysis between regional FGID prevalence identified differences between Andean and Pacific regions (p < 0.001) and Amazonia and Pacific regions (p = 0.007). Disorders of defecation (functional constipation and non-retentive fecal incontinence) were the most common category of FGIDs (11.7%), followed by AP-FGIDs (10.4%) and vomiting/aerophagia (1.6%). Functional constipation accounted for nearly all disorders of defecation (n=509/512, 99.4%) and irritable bowel syndrome (IBS) was the most common AP-FGIDs (n=222/457, 48.6%) (Table 1).
Prevalence of Functional Gastrointestinal Disorders by Region.
| Andean | Atlantic | Pacific | Amazonia | Colombia | |
|---|---|---|---|---|---|
| Total | 1544 | 1373 | 1085 | 392 | 4394 |
| No FGIDs | 1141 (73.9%) | 1055 (76.8%) | 870 (80.2%) | 288 (73.5%) | 3354 (76.3%) |
| FGIDs | 403 (26.1%) | 318 (23.2%) | 215 (19.8%) | 104 (26.5%) | 1040 (23.7%) |
| Vomiting and aerophagia | 71 (1.6%) | ||||
| Aerophagia | 7 (0.5%) | 19 (1.4%) | 11 (1.0%) | 0 | 37 (0.8%) |
| Cyclic vomiting syndrome | 5 (0.3%) | 5 (0.4%) | 5 (0.5%) | 2 (0.5%) | 17 (0.4%) |
| Adolescent Rumination Syndrome | 4 (0.3%) | 9 (0.7%) | 3 (0.3%) | 1 (0.3%) | 17 (0.4%) |
| Abdominal pain predominant-FGIDs | 457 (10.4%) | ||||
| Functional dyspepsia | 13 (0.8%) | 11 (0.8%) | 16 (1.5%) | 6 (1.5%) | 46 (1%) |
| Irritable bowel syndrome | 87 (5.6%) | 68 (5.0%) | 49 (4.5%) | 18 (4.6%) | 222 (5.1%) |
| Abdominal migraine | 36 (2.3%) | 12 (0.9%) | 24 (2.1%) | 4 (1.0%) | 76 (1.7%) |
| Functional abdominal pain | 31 (2.0%) | 18 (1.3%) | 19 (1.8%) | 8 (2.0%) | 76 (1.7%) |
| Functional abdominal pain syndrome | 22 (1.4%) | 5 (0.4%) | 9 (0.8%) | 1 (0.3%) | 37 (0.8%) |
| Constipation and incontinence | 512 (11.7%) | ||||
| Functional constipation | 198 (12.8%) | 171 (12.5%) | 76 (7.0%) | 64 (16.3%) | 509 (11.6%) |
| Nonretentive fecal incontinence | 0 | 0 | 3 (0.3%) | 0 | 3 (0.07%) |
FGID, functional gastrointestinal disorder
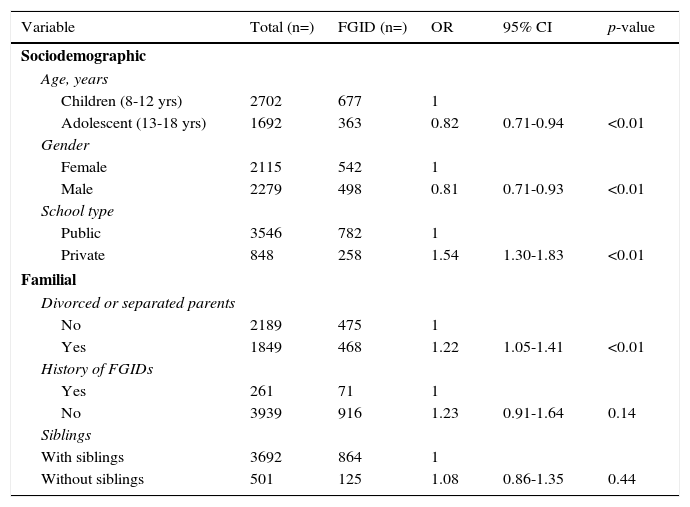
FGIDs were significantly less common in adolescents than children (21.5% vs. 25.1%, OR 0.82). Males had significantly fewer FGIDs than females (21.9% vs 25.6%, OR 0.81). There was higher prevalence of FGIDs among children whose parents were separated/divorced (25.3% vs. 21.7%, OR 1.22). Children from private schools had significantly more FGIDs than children from public schools (30.4% vs. 22.1%, OR 1.54). There was a greater frequency of FGIDs among children with parents who had FGIDs, but the difference was not significant (37.4% vs 23.3%, OR 1.23). There was no difference in prevalence of FGIDs between children with and without siblings (23.4% vs. 25.0%, OR 1.08) (Table 2).
Relationship between the presence of FGIDs and sociodemographic and familial variables in children in Colombia.
| Variable | Total (n=) | FGID (n=) | OR | 95% CI | p-value |
|---|---|---|---|---|---|
| Sociodemographic | |||||
| Age, years | |||||
| Children (8-12 yrs) | 2702 | 677 | 1 | ||
| Adolescent (13-18 yrs) | 1692 | 363 | 0.82 | 0.71-0.94 | <0.01 |
| Gender | |||||
| Female | 2115 | 542 | 1 | ||
| Male | 2279 | 498 | 0.81 | 0.71-0.93 | <0.01 |
| School type | |||||
| Public | 3546 | 782 | 1 | ||
| Private | 848 | 258 | 1.54 | 1.30-1.83 | <0.01 |
| Familial | |||||
| Divorced or separated parents | |||||
| No | 2189 | 475 | 1 | ||
| Yes | 1849 | 468 | 1.22 | 1.05-1.41 | <0.01 |
| History of FGIDs | |||||
| Yes | 261 | 71 | 1 | ||
| No | 3939 | 916 | 1.23 | 0.91-1.64 | 0.14 |
| Siblings | |||||
| With siblings | 3692 | 864 | 1 | ||
| Without siblings | 501 | 125 | 1.08 | 0.86-1.35 | 0.44 |
FGID, functional gastrointestinal disorder, OR, odds ratio, CI, confidence interval
Nausea was reported by 10.5% of all children. Nausea was significantly more common among children with FGIDs (OR 3.63; 95% CI 2.96-4.44; p < 0.001). There was an association of nausea with most FGIDs: IBS (OR 5.10; 95% CI 3.74-6.92; p < 0.001), functional abdominal pain (OR 4.71; 95% CI 2.18-9.71; p < 0.001), abdominal migraine (OR 4.62; 95% CI 2.73-7.66; p < 0.001), functional dyspepsia (OR 3.80; 95% CI 1.86-7.40; p < 0.001), and functional constipation (OR 1.42; 95% CI 1.06-1.87; p = 0.011). There was no significant association between nausea and aerophagia, rumination, cyclic vomiting syndrome, or non-retentive fecal incontinence.
4DiscussionThis is the largest epidemiological study conducted in the Western Hemisphere aimed at describing FGIDs in children using the Rome III criteria. The study included 4394 children from 12 public and private schools in 10 geographically dispersed cities in Colombia, providing a broad-based survey throughout a Latin American nation. The nationwide distribution of our sample and the high acceptance rate to participate in the study (86.8%) indicates the external validity of our data. We found that almost one in four children (23.7%) had a FGID according to the Rome III criteria. The prevalence of FGIDs found in this study was similar to that found in Quito (22.8%),12the capital of Ecuador which borders Colombia to the south. Similar to the results of this study (11.6%), functional constipation was the most common FGID in Ecuador (11.8%).
We found that 10.4% of children in Colombia had AP-FGIDs. This is again within close range to the prevalence of AP-FGIDs found in Ecuador (9.4%) using the same methods.12 A review of AP-FGIDs in children found that worldwide pooled prevalence of AP-FGIDs was higher than in our sample 13.5% (95% CI 11.8-15.3).15The study identified IBS as the most common AP-FGID, but at higher rates (8.8%, 95% CI 6.2-11.9) than in our study (5.1%). The study found a high range of AP-FGID prevalence across countries ranging from 1.6% to 41.2%. Prevalence of adult IBS is estimated to be 21-26% in Peru16 and 19.9% in Colombia, which are higher than in our study in children. The reasons for the differences in prevalence of AP-FGIDs between children and adults and among geographic regions remains unknown and should be studied with large international comparative studies using standardized methodology and subjects of different age groups.
FGIDs were more common in children from private than public schools and in children whose parents were separated. Another Latin-American study also found that children from divorced/separated families had a higher prevalence of FGIDs11 than children from intact families. Although the design of this study does not allow determination of causality, the results are in line with the biopsychosocial model that proposes psychological and social factors play a role in the pathogenesis of FGIDs. According to the biopsychosocial model, AP-FGID symptoms result from the interaction of gastrointestinal and central nervous system factors.17Stress has pathophysiological effects in the gastrointestinal tract. Higher stress levels can trigger or exacerbate abdominal pain through visceral hypersensitivity and changes in motility. Children with depressive or anxious symptoms are more likely to suffer from AP-FGIDs18 and studies in school-children found an association between anxiety and depression with abdominal pain.19Divorce is a major stressor20 and parental separation and divorce are associated with higher rates of depression.21Studies comparing early adolescents from divorced and intact families found that adolescents from divorced families had higher rate of anxiety and more depressed mood.22A higher prevalence of FGIDs in children from private schools was also found in other studies conducted in Latin-American countries such as El Salvador11 and Ecuador.12A study that interviewed more than 500 adolescents in Colombia found higher levels of anxiety among children of public schools.23However, the study was performed in a single town near Bogota and it is also known that the interrelation between the psychological factors involved in the pathogenesis of FGIDs is complex.24Moreover, other non-psychological factors could explain these findings. Future studies by FINDERS will specifically investigate these issues.
Despite previous studies in the United States showing that children of parents with IBS reported more gastrointestinal symptoms,25,26we did not find an association between FGIDs and family history. A family history of FGIDs also did not associate with higher prevalence of FGIDs in Salvadoran children.11The reason for this difference is unclear. Cultural differences in the way a FGID is conceptualized and differences in parenting and coping styles between the US and Latin-American societies may explain these differences.
We did not find gender predominance in FGIDs. These results are similar to those of pediatric studies in Mexico,27 Ecuador,12 Panama,10 and El Salvador.11 A meta-analysis by Lovell and Ford16 found a female predominance in adults with IBS. However, this difference was not found when South-American studies were analyzed as a whole.
Limitations of our study include the completion of questionnaires exclusively by children and not by parents. It can be argued that children know their symptoms better than their parents, and may be reluctant to share information regarding bowel movements with their parents, while having comfort reporting on an anonymous questionnaire. We cannot rule out the possibility that although our study included multiple cities in various regions, the results may not be generalized to all cities in Colombia. Additionally, concurrent medical diagnoses may be present in surveyed children with or without FGIDs and were not assessed in the study.
In conclusion, this study provides relevant information for public health planning, finding a high prevalence of FGIDs in children of Colombia. Children from private schools and from families whose parents have separated are at higher risk of FGIDs, and nausea is associated with increased rates of FGIDs in children.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
FundingThere was no external source of funding related to this research and no specific acknowledgements requested for inclusion.
Conflict of interestThe authors declare no conflict of interest.