


Currently, there is a spreading worldwide tendency to characterize health issues and to propose alternative solutions via the creation of computerized databases. The aim of this study was to present the results in a computerized database of pediatric cardiac surgeries developed under the auspices of the Mexican Association of Specialists in Congenital Heart Diseases (Asociación Mexicana de Especialistas en Cardiopatías Congénitas A.C) and coordinated by the collegiate group of Pediatric Cardiology and Surgery as petitioned by the National Institutes of Health and High Specialty Hospitals Coordinating Commission.
MethodsWe analyzed all cases registered in the database during a 1-year observation period (August 1, 2011 to July 31, 2012) by all major Health Ministry-dependent institutes and hospitals offering surgical services related to pediatric cardiopathies to the non-insured population.
ResultsSeven institutions participated voluntarily in completing the database. During the analyzed period, 943 surgeries in 880 patients with 7% reoperations (n=63) were registered. Thirty-eight percent of the surgeries were performed in children <1 year of age. The five most common cardiopathies were patent ductus arteriosus (n=96), ventricular septal defect (n=86), tetralogy of Fallot (n=72), atrial septal defect (n=68), and aortic coarctation (n=54). Ninety percent of surgeries were elective and extracorporeal circulation was used in 62% of surgeries. Global mortality rate was 7.5% with the following distribution in the RACHS-1 score categories: 1 (n=4, 2%), 2 (n=19, 6%), 3 (n=22, 8%), 4 (n=12, 19%), 5 (n=1, 25%), 6 (n=6, 44%), and non-classifiable (n=2, 9%).
ConclusionsThis analysis provides a representative view of the surgical practices in cardiovascular diseases in the pediatric population at the national non-insured population level. However, incorporating other health institutions to the national registry database will render a more accurate panorama of the national reality in surgical practices in the population <18 years of age.
Congenital heart diseases constitute the most important group of congenital malformations. They are a relatively common problem with an incidence of 6/1000 newborns. Approximately 25% of these children suffer from critical congenital heart diseases that require surgery or therapeutic catheterization during the first year of life. Congenital heart diseases contribute to 3% of infant mortality and to 46% of deaths caused by congenital malformations, with most deaths occurring within the first year of life. Worldwide, it is estimated that only 2–15% of patients suffering from congenital heart diseases are subject to curative surgical or interventional procedures.1–8
Amidst this panorama, in 2007, the World Society for Pediatric and Congenital Heart Surgery (WSPCHS) was formed with the aim of promoting efforts destined to optimize care given to patients suffering from congenital heart diseases worldwide. To achieve the aforementioned goal, one primary strategy implemented was the creation of a series of registries that could reflect the global situation in terms of surgical treatment for patients with congenital heart diseases.
In 2008, the Mexican Association of Specialists in Congenital Heart Diseases (Asociación Mexicana de Especialistas en Cardiopatías Congénitas, AMECC, A.C.) was created as an affiliate of the WSPCHS. Furthermore, the collegiate group of pediatric cardiology and cardiac surgery, as a dependence of the National Institutes of Health and High Specialty Hospitals Coordinating Commission (CCINSAHE), was formed and these groups have designed and undertaken several actions in the field of congenital heart diseases. The first action was to implement a regionalization process that would serve as a theoretical framework for the upcoming steps. As a second measure, a census on human and technological resources for patients with congenital heart diseases in the country was performed. The third, and final measure, was the creation of a database, the Pediatric Cardiovascular Surgical Database Registry (PCSDR)/Registro Nacional de Cirugía Cardiaca Pediátrica (RENACCAPE), which uses international nomenclature to enable users to obtain information about health practices in the country's various health centers and serves as a reference point to recognize and quantify the successes of the initiative.4,9–11 The Health Ministry, via the National Institutes of Health and High Specialty Hospitals Coordinating Commission, shares various interests in common with the AMECC A.C., which has fomented synergy in this project.
Given the heterogeneous nature of the institutions that comprise the health care system and the lack of communication among these institutions, one of the main obstacles to the development of pediatric cardiac surgery in Mexico has been a lack of information on the number and type of congenital heart diseases, type of surgical procedures performed and complexity, morbidity and mortality, among others. The aim of the present article is to present the information obtained from the RENACCAPE, 1 year after its creation.
2MethodsWith the support of the CCINSHAE, all institutions that serve the pediatric population in which cardiac surgery is performed were summoned to participate voluntarily in the RENACCAPE. The institutions that were willing to participate were given an access code to introduce cardiovascular surgical data performed on patients <18 years of age from August 1, 2011 until July 31, 2012. Variables analyzed were age, gender, birth place, category of congenital heart disease, type of surgery (elective or emergency), use of extracorporeal circulation, surgical risk classification (RACHS-1), morbidity and mortality. Statistical analysis was performed using SPSS v. 11.5. Categorical variables are presented as numbers and percentages in relation to the studied population. Continuous variables are presented as averages and percentages.
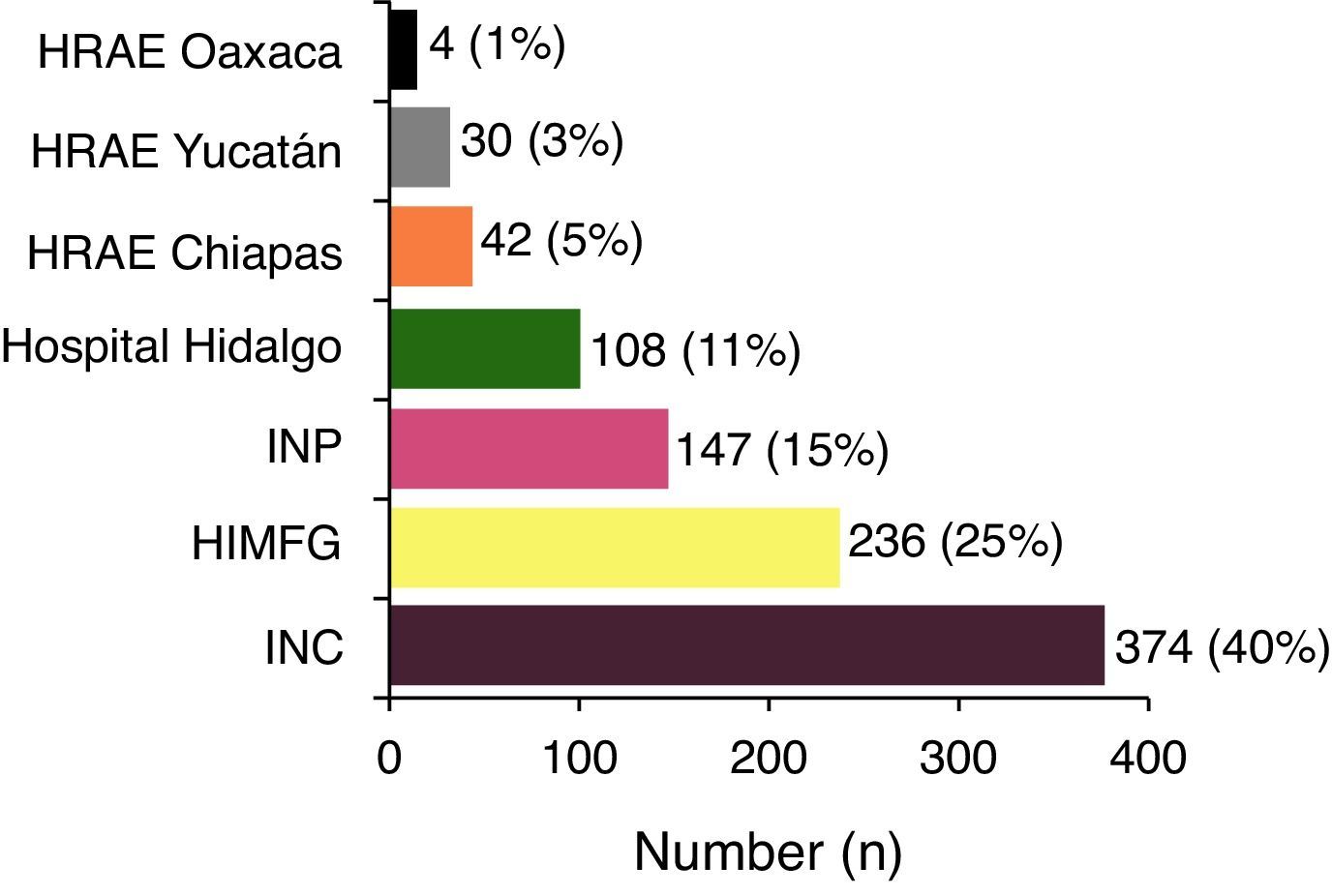
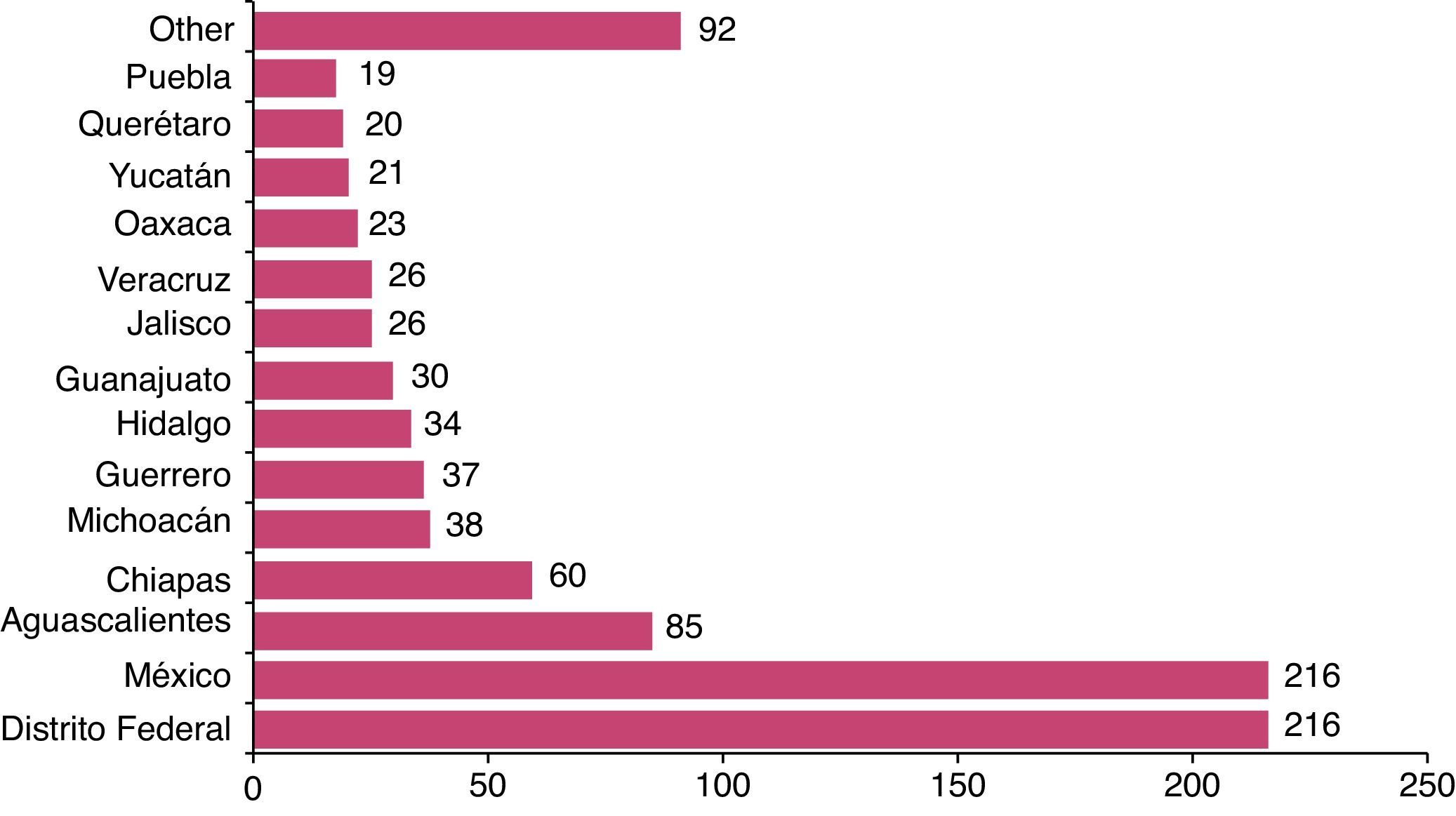
3ResultsDuring the studied period, seven hospitals provided the CCINSHAE and RENACCAPE with the necessary information for the present analysis: Instituto Nacional de Cardiología Dr. Ignacio Chávez, Instituto Nacional de Pediatría, Hospital Infantil de México Federico Gómez, Hospital Miguel Hidalgo de Aguascalientes, Hospital Regional de Alta Especialidad de la Península de Yucatán, Hospital Regional de Alta Especialidad de Chiapas and Hospital Regional de Alta Especialidad de Oaxaca. Of the participating hospitals, three are located in the country's capital and four are located in other states. Fig. 1 shows the number of patients treated at each hospital. Fig. 2 shows the different birthplaces of patients where the Federal District (DF), State of México, Aguascalientes and Chiapas stand out.


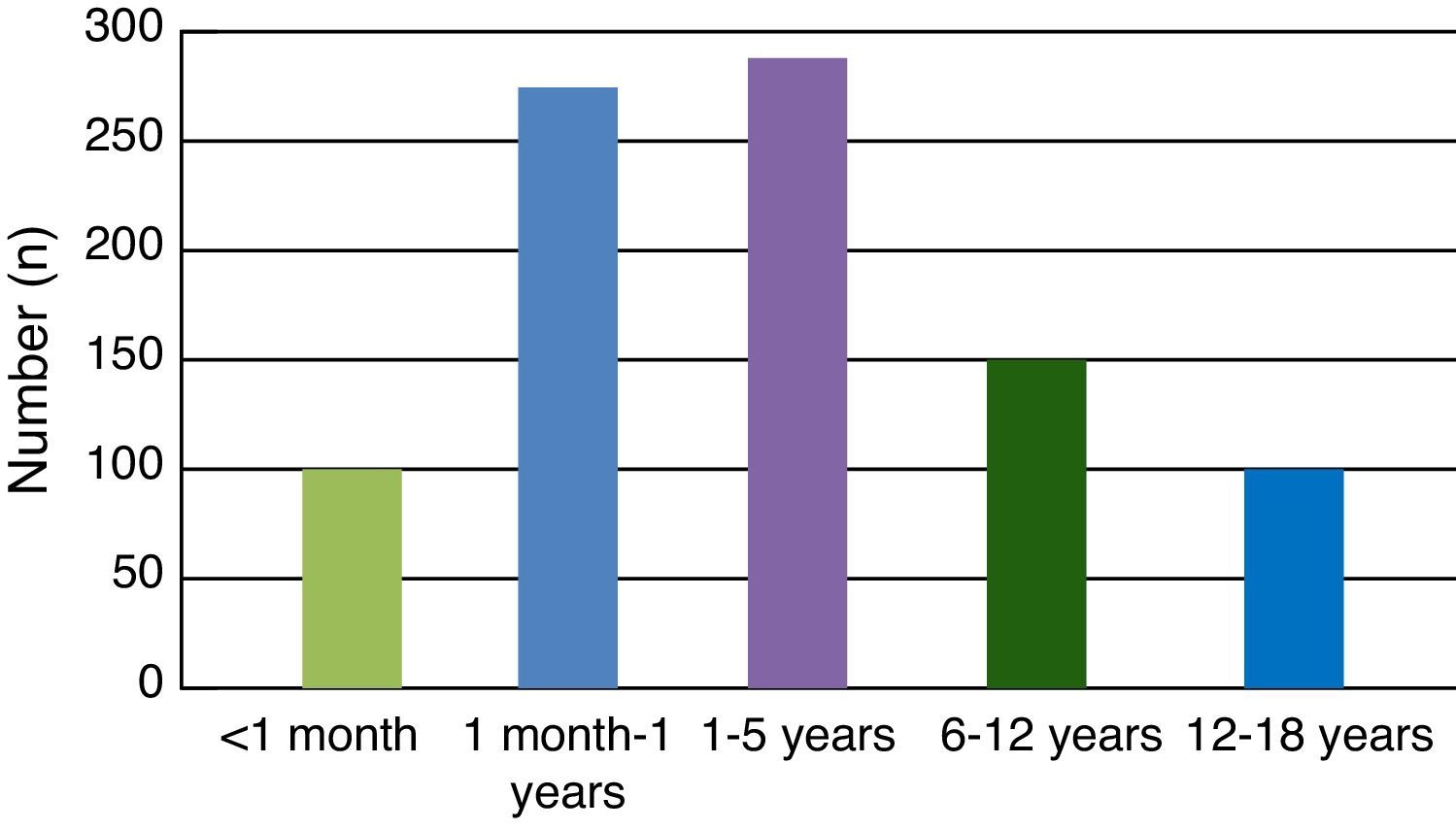
During the analyzed period, 943 procedures were performed on 880 patients; 7% of these were re-operated, which corresponds to 63 patients (Fig. 3). Fifty three percent (504 patients) of the procedures were performed on males. Age at the time of surgery was <1 month in 102 patients, representing 11% of the total group of patients. A total of 271 patients were aged 1 month to 1 year, which considered alongside the newborns constitute 42% of the analyzed sample. On the other hand, 281 patients were between the ages of 1 and 5 years old, which constitute 31% of the studied population. There were 158 patients between 6 and 11 years of age constituting 18% of the sample and 131 patients between the ages of 12 and 18 years, which represented 14% of the sample (Fig. 4).


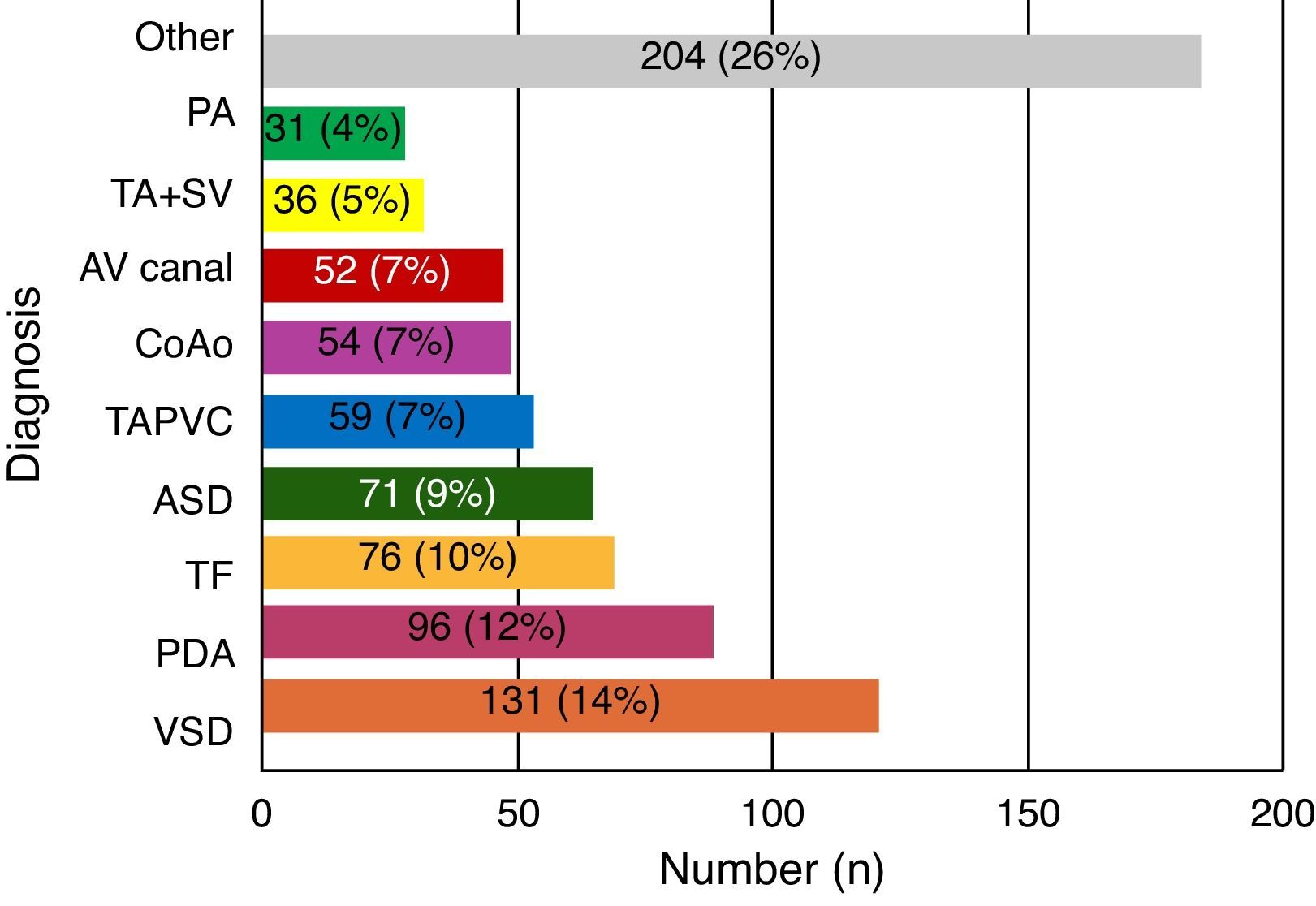
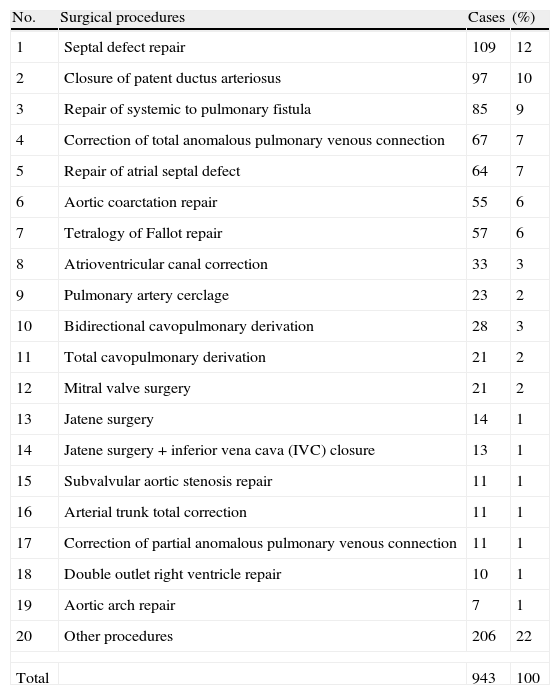
The most common surgically treated congenital heart diseases were ventricular septal defects (131 cases); patent ductus arteriosus (96 patients); tetralogy of Fallot (72 patients); atrial septal defect (69 patients); different variants of total anomalous pulmonary venous connection (59 cases), and coarctation of the aorta (54 cases). These six congenital malformations represented 54% of all reported patients (Fig. 5). In terms of surgery, 88.9% of cases were elective, which represents 838 patients. Extracorporeal circulation was required in 583 patients (61.9%). Table 1 shows all congenital heart disease surgical procedures reported to the CCINSAHAE and the RENACCAPE.

Diagnoses for patients included in the RENACCAPE. VSD: ventricular septal defects; PDA: patent ductus arteriosus; TF: tetralogy of Fallot; ASD: atrial septal defect; TAPVC: different variants of total anomalous pulmonary venous connection; CoAo: coarctation of the aorta; AV canal: atrioventricular canal correction; TA+SV: tricuspid atresia+single ventricle; PA: pulmonary artery.
Surgical procedures performed from August 1, 2011 to July 31, 2012.
| No. | Surgical procedures | Cases | (%) |
| 1 | Septal defect repair | 109 | 12 |
| 2 | Closure of patent ductus arteriosus | 97 | 10 |
| 3 | Repair of systemic to pulmonary fistula | 85 | 9 |
| 4 | Correction of total anomalous pulmonary venous connection | 67 | 7 |
| 5 | Repair of atrial septal defect | 64 | 7 |
| 6 | Aortic coarctation repair | 55 | 6 |
| 7 | Tetralogy of Fallot repair | 57 | 6 |
| 8 | Atrioventricular canal correction | 33 | 3 |
| 9 | Pulmonary artery cerclage | 23 | 2 |
| 10 | Bidirectional cavopulmonary derivation | 28 | 3 |
| 11 | Total cavopulmonary derivation | 21 | 2 |
| 12 | Mitral valve surgery | 21 | 2 |
| 13 | Jatene surgery | 14 | 1 |
| 14 | Jatene surgery+inferior vena cava (IVC) closure | 13 | 1 |
| 15 | Subvalvular aortic stenosis repair | 11 | 1 |
| 16 | Arterial trunk total correction | 11 | 1 |
| 17 | Correction of partial anomalous pulmonary venous connection | 11 | 1 |
| 18 | Double outlet right ventricle repair | 10 | 1 |
| 19 | Aortic arch repair | 7 | 1 |
| 20 | Other procedures | 206 | 22 |
| Total | 943 | 100 | |
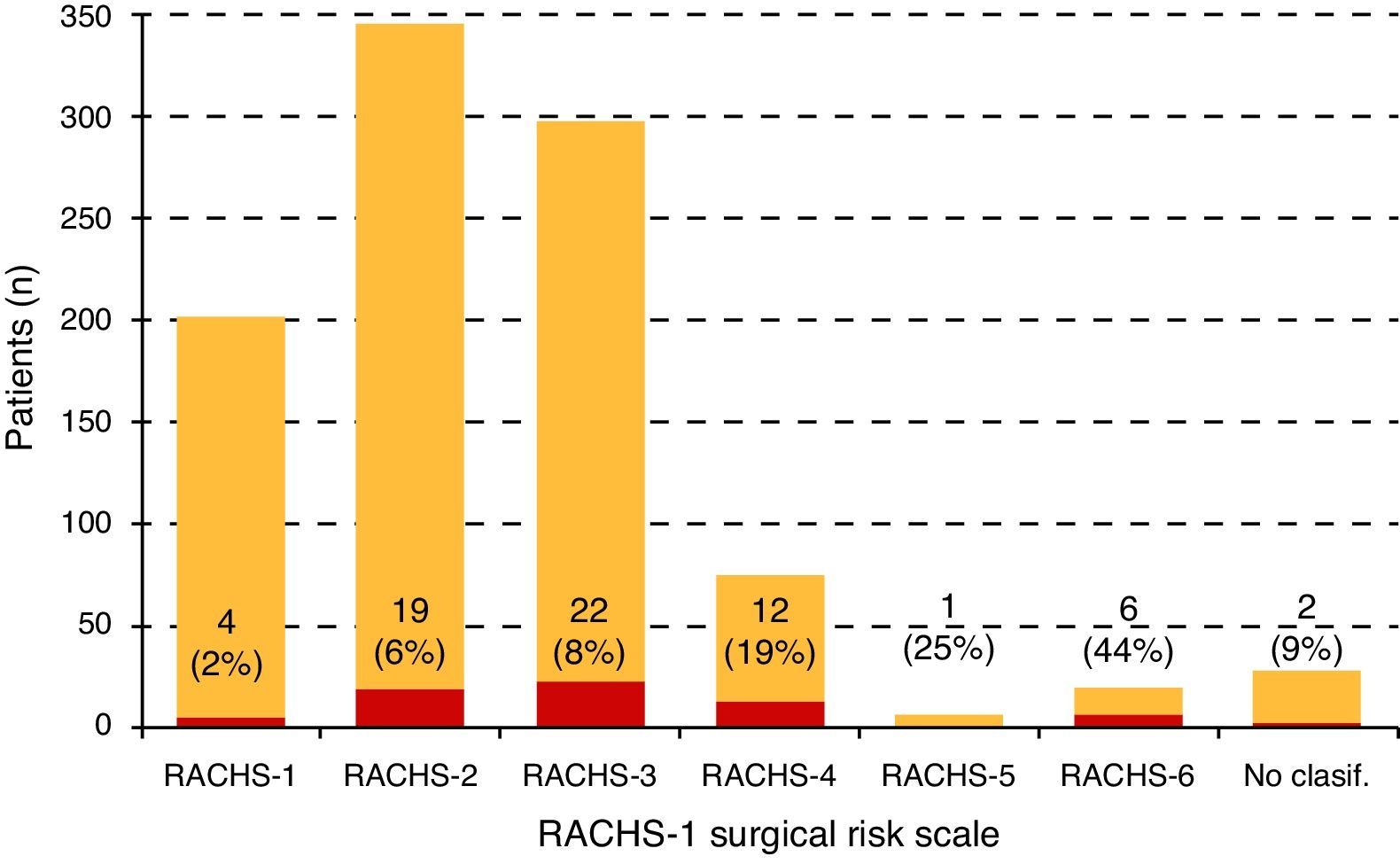
Surgical mortality was 7.5% and the main causes of death were cardiac arrest, multi-organ failure and hemorrhage, which together constitute 80% of deaths. According to the collected information and considering the surgical risk classification RACHS-1, 197 patients were reported as risk grade 1; 328 were classified as risk grade 2; 277 patients were considered risk grade 3; 62 patients were deemed risk grade 4; four patients as risk grade 5; and 13 cases were classified as risk grade 6; whereas 25 patients were recorded under the unclassifiable risk label. These details and mortality for each risk score are displayed in Fig. 6. After analyzing the causes of surgical morbidity, infectious processes stood out as the most common.
4Discussion
Since the creation of the AMECC, A.C. and the Collegiate Group of Pediatric Cardiology and Cardiac Surgery in 2008 and the simultaneous establishment of other similar associations in other nations and regions of the world, one of the primary objectives was the creation of a registry or database that allows a more accurate understanding of the problems linked to congenital heart diseases in Mexico. A more thorough understanding of congenital heart diseases is paramount to suggest alternative solutions in the surgical care of children suffering from heart disease. For this reason, the RENACCAPE was created with the primary objective to present the type of ailments and the surgical procedures performed on pediatric patients with congenital or acquired heart disease in the country. Although the project scope will ultimately be broader, its initial design beseeches participating centers to provide basic information about patients and surgical procedures to incorporate the database as a user-friendly and manageable tool. As the participating centers grow accustomed to the recollection and information-recording techniques we will proceed gradually to expand and improve the database incorporating the consensus from all participating centers with hopes of creating a trustworthy national registry with sufficient and detailed information that will shed light on the actual situation of pediatric cardiac surgery in Mexico.
The RENACCAPE database is elaborated with diagnostic and procedural codes that have been established by an international consensus. All procedures and diagnoses are classified using a unique code, which at any given moment can be utilized to perform multicenter studies including hospitals around the world that use the same codification.11–17 Another virtue of the database is that it is designed in such a fashion that while information may be recollected from all participating hospitals, information can be processed for each site individually, showing information specific to a particular institution. Therefore, the registry serves both as a national database/source of information and as a database for individual hospitals. Thus, information can be analyzed and compared for research purposes. Seeing as how practically no hospital in Mexico devoted to pediatric cardiovascular surgery possesses this tool, this additional benefit has been well received in the participating hospitals and we hope it serves as an instigator so that more hospitals join in the future. The primary challenge we faced while trying to implement the registry is the reluctance of hospitals to provide their data; therefore, we have commenced an arduous convincing process. We hope that, in the medium term, other hospitals will be willing to participate and acknowledge the utility of the obtained information.
The first report of the registry provides valuable information as data was collected from 880 patients <18 years old and 943 surgeries performed in seven participating hospitals and institutions. The most frequent heart diseases were, first, ventricular septal defects in different locations (perimembranous, subinfundibular, trabecular and inlet defects); second, ductus arteriosus and, third, tetralogy of Fallot followed by atrial septal defect, total anomalous pulmonary venous connection, and coarctation of the aorta. These six congenital malformations represent half (54%) of all reported cases. It is noteworthy that ductus arteriosus, atrial septal defect, and coarctation of the aorta are being treated more frequently by interventional catheterization. The high incidence of tetralogy of Fallot as well as total anomalous pulmonary venous connection is also noteworthy, although the former malformation is not as frequent in Anglo-Saxon countries.2,4,5,7–9
In terms of age at the time of surgery, the registry shows that 42% of patients (373) had to be operated on during the first year of life and in 10% surgery had to be performed within the first month (of life).
We consider that these numbers will increase in all likelihood in the upcoming years as a result of more timely heart disease detection and attention. Regarding the distribution according to surgical indication, in practical terms surgery was elective in 90% of cases and extracorporeal circulation was required in two-thirds (61.8%) of the studied population.
Overall operative mortality was 7.5%. Specific mortalities considering the surgical risk classification RACHS-1 are detailed in Fig. 6. Infectious processes stand out as the first cause of morbidity. Although the results in patients with risk level 5 (including repair of Ebstein anomaly in newborns and repair of truncus arteriosus with interrupted aortic arch) and risk level 6 (including first stage Norwood or Damus–Kaye–Stansel procedures for hypoplastic left heart syndrome) are acceptable (25% and 45%, respectively), these cardiopathies are still a major challenge in highly specialized institutions in Mexico. However, it is important to underscore that, in the proper perspective, these two risk groups represent only 1.9% of all patients treated in the analyzed period.10
The goal of this important project is to achieve the inclusion and participation of the majority of centers dedicated to the care of congenital heart diseases in Mexico. Another aim is to present information in a trustworthy manner and that such information can be audited to validate national statistics. The benefits that this information can signify for institutions in terms of evaluating needs and elaborating institutional policies are undeniable. Furthermore, there is a real possibility to engage specific lines of solution seeking actions at the Ministry/Secretary of Health. Therefore, the RENACCAPE is a tool that may become increasingly valuable as national participation is strengthened.
Moreover, this registry will be a source of valuable information to achieve regionalization of congenital heart disease surgical practices. Regionalization should be understood as the rational use of existing resources, considering primarily the 12 specialized health institutions with the aim of increasing the number of persons served and improving the quality of services.12–18
With the information obtained in the first report of the RENACCAPE as well as future reports and based on the population and existing resources in each state, the CCINSHAE and the health care sector will be able to intensify regionalization and the establishment of practices based on risk evaluation and stratification (RACHS-1) with periodic evaluations aimed at improving the program. The aforementioned point will provide benefits to our society as the number of cases handled may increase, quality of attention will improve, and existing resources will be exploited to their fullest capacity.
We can conclude that the results of the first report can be considered as a potential indicator of the usefulness of our database in shaping surgical practices in pediatric cardiovascular disease. We believe that two big challenges lie ahead: implementation of an auditing system to verify the information collected and the incorporation of a larger number of national centers to our project. However, it is of utmost relevance that the pediatric cardiovascular surgical database registry, which until a few years ago appeared as a utopian dream, has been transformed into a reality today and surely could not have been materialized without the invaluable support of the Collegiate Group of Pediatric Cardiology and Cardiac Surgery and the National Institutes of Health and High Specialty Hospitals Coordinating Commission.
Conflict of interestThe authors declare no conflict of interest.
This article was first published in Revista de Investigación Clínica: Cervantes-Salazar, et al. [Mexican registry of pediatric cardiac surgery]. Rev Inv Clin 2013;65:476–482.
Readers are encouraged to consult the original publication cited in the footnotes, with written authorization from the Editor in Chief of Revista de Investigación Clínica to verify the accuracy of the content reproduced in this issue of Boletín Médico del Hospital Infantil de México.