


The word “re-laparotomy” defines the surgical procedure in which the abdominal cavity is re-explored to resolve the complications of the disease or initial surgery.
ObjectiveTo determine the prevalence of abdominal re-operations in patients undergoing elective and emergency surgery in the General Hospital of Matamoros.
Material and methodsA retrospective, observational, longitudinal study was conducted by reviewing the medical records of patients with a re-operation from January 2014 to January 2015, statistically analysing the variables: age, sex, type of surgery, complications, and postoperative course.
ResultsA total of 21 re-operated patients were found, the majority of whom were women (52.38%). The cases were more common in ages between 70 and 79 years old, in both sexes. Almost two-thirds (61.91%) of re-operations were after an emergency surgery. The residual abscess (23.8%) and evisceration (23.8%) were the most frequent indications for re-intervention. There were postoperative complications in 23.8%, with wound dehiscence (60%) being the most frequent. There was an 85.6% survival rate after the re-intervention.
ConclusionsThe study showed a low incidence of re-interventions and a low mortality. There is evidence of major occurrence of abdominal re-interventions in advanced ages, in female patients, and emergency surgery.
El término «relaparotomía» define el procedimiento quirúrgico en el cual la cavidad abdominal es reexplorada, con el objetivo de resolver las complicaciones de la enfermedad o cirugía inicial.
ObjetivoDeterminar la prevalencia de reintervenciones abdominales en pacientes intervenidos mediante cirugías electivas y de urgencia en el Hospital General de Matamoros.
Material y métodosSe realizó un estudio retrospectivo, observacional y longitudinal, revisando los expedientes clínicos de pacientes reintervenidos de enero de 2014 a enero de 2015, analizando estadísticamente las variables: edad, sexo, tipo de cirugía, complicaciones y evolución postoperatoria.
ResultadosLa población fue de 21 pacientes reintervenidos; la mayoría mujeres (52.38%), El grupo de edad con mayor número de reintervención fue el de los 70-79 años. El 61.91% fueron reintervenidos después de una cirugía de urgencia. La colección intraabdominal (23.8%) y la evisceración (23.8%) fueron las indicaciones para las reintervenciones más frecuentes. El 23.8% presentaron complicaciones postoperatorias; la más frecuente fue la dehiscencia de herida con un 60%. El 85.6% sobrevivió a la reintervención.
ConclusionesSe revela un porcentaje de reintervenciones y una mortalidad baja. Se observa mayor frecuencia en las reintervenciones abdominales en edades avanzadas, en el sexo femenino y en cirugías de urgencia.
The term “relaparotomy” defines the surgical procedure in which the abdominal cavity is re-explored in order to resolve complications of initial disease or surgery.1 This is a laparotomy performed in a patient who has been operated previously and has presented with a complication in the first 2 months postoperatively.2 Relaparotomies are performed for different reasons in surgery of the digestive system, both emergency and elective, as a consequence of complications.3
Abdominal reoperation usually follows a surgical procedure that might not have been satisfactory or when a problem is detected that could not be resolved initially because of the patient's haemodynamic or ventilatory condition4 or postsurgical complications due to intrinsic or extrinsic factors, such as: haemorrhage, infection, malnutrition or even shortcomings of the surgical technique itself.5
Abdominal reoperations are divided into 2 categories: emergency and scheduled. Emergency reoperations are performed immediately in the first 24h post-operatively; early reoperations take place during the same hospital stay and, less often, late reoperations are performed when the patient has already left hospital. They are due to foreseeable complications according to the patient's disease and the surgery performed, or they are unforeseeable, in patients who were expected to have satisfactory outcomes.6
There have been increasing numbers of publications over the past 30 years on abdominal reoperation, under different surgical circumstances and after various procedures. At the beginning of the 80s, the strategy of damage control surgery for trauma7 came into existence and common practice, with its implicit need to re-open the peritoneal cavity, which resulted in an increased frequency of relaparotomies. However, it was in the 90s that the strategy became popular when the results of the large series started a decade earlier were published.8–10
Despite the technological advances enabling strict monitoring of patients’ haemodynamic, ventilatory and nutritional variables, the morbidity and mortality of abdominal reoperations remains high.4 In the economically productive age group, it causes hospitalisation days, greater absenteeism from work and increased medical input costs for both patients and institutions. Hence the need to generate knowledge for the application of measures to optimise resources and promote better quality of care.5
There are few publications that refer to surgical reoperations in abdominal surgery, despite the problems in diagnosis and the indication for surgery in patients who have been operated previously.2
Material and methodsA retrospective, observational and longitudinal study was undertaken, with a review of clinical case records from 1 January 2014 to 1 January 2015 in the Hospital General Dr. Alfredo Pumarejo Lafaurie in the city of H. Matamoros (Tamaulipas).
We analysed the clinical case reports obtained from the outpatients’ archive of all the patients who underwent abdominal surgery in the General Surgery Department and who required abdominal reoperation. Clinical records were selected that contained the surgical datasheets and clinical histories for the first abdominal surgery and for the second attempt, and that came from emergency departments, outpatients or from the hospital ward. Patients were included that were discharged from the post-anaesthetic recovery room a minimum of 4h after the surgical event and with surgical wound closure by suture. The epidemiological variables of age and sex were evaluated as well as the variables of emergency surgery, elective surgery, reasons for abdominal reoperation, secondary morbidity and mortality. These data were entered into a file created for their analysis.
Reoperation was considered to be a secondary abdominal operation after closure of the surgical wound, and during a period of 30 days from the primary surgical event. Patients that died during the primary operation, those that underwent open abdominal management and those who were transferred to a different medical unit for specialist medical care was eliminated from the study.
The percentages method was used for statistical analysis of the data.
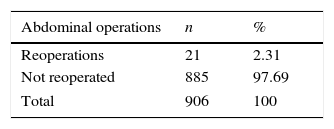
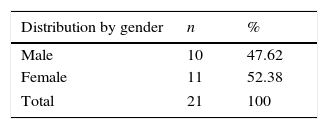
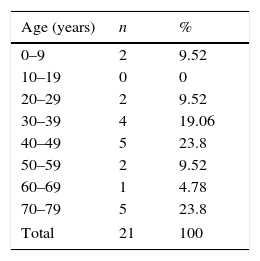
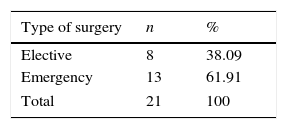
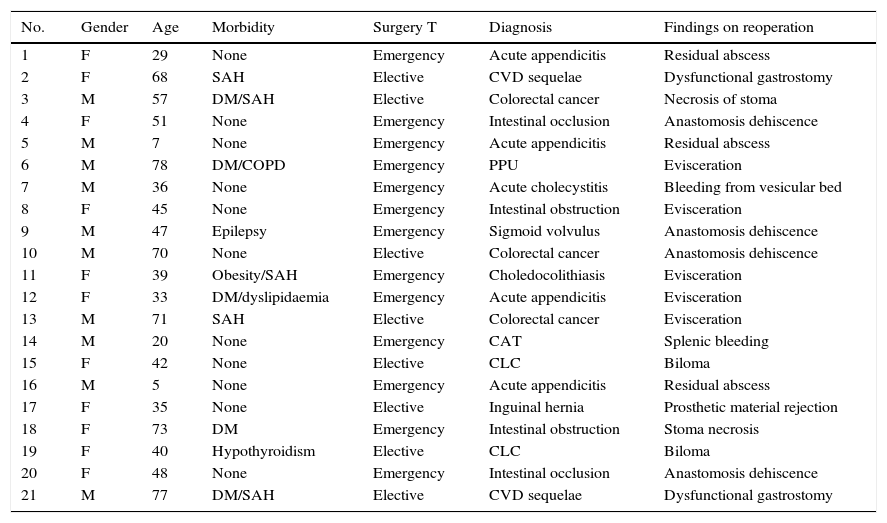
ResultsThe population comprised 906 patients who had undergone abdominal surgery of some type in the General Surgery Department during the aforementioned period. Clinical judgement predominated in deciding relaparotomy. In total 21 reoperated patients (2.31%) were found (Table 1). 52.38% were female (Table 2). In both genders most cases presented in the age range between 70 and 79 years (Table 3). From the total sample, 61.91% were reoperated after emergency surgery (Table 4). Diagnoses of intra-abdominal collection (23.8%) and evisceration (23.8%) were the most frequent medical indications for reoperation (Table 5). Of the patients reoperated due to abdominal collection, 3 were secondary to acute appendicitis due to residual abscess and, 2 due to biloma (Table 6). Evisceration was one of the most common causes for reoperation. It should be mentioned that in all cases the abdominal wall was sutured using absorbable multifilament material (polyglycolic acid 1), with continuous suture. The mean time between the primary intervention and abdominal reoperation was 19 days. 33.3% of the patients had a comorbidity, 23.8% presented postoperative complications, 85.6% survived the reoperation.
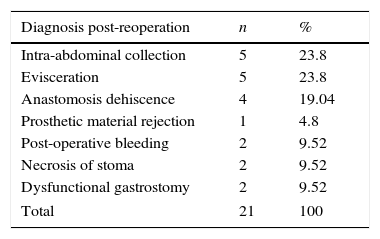
Post-surgical diagnoses post-reoperation.
| Diagnosis post-reoperation | n | % |
|---|---|---|
| Intra-abdominal collection | 5 | 23.8 |
| Evisceration | 5 | 23.8 |
| Anastomosis dehiscence | 4 | 19.04 |
| Prosthetic material rejection | 1 | 4.8 |
| Post-operative bleeding | 2 | 9.52 |
| Necrosis of stoma | 2 | 9.52 |
| Dysfunctional gastrostomy | 2 | 9.52 |
| Total | 21 | 100 |
Total reoperated patients with the most relevant characteristics, including findings during reoperation.
| No. | Gender | Age | Morbidity | Surgery T | Diagnosis | Findings on reoperation |
|---|---|---|---|---|---|---|
| 1 | F | 29 | None | Emergency | Acute appendicitis | Residual abscess |
| 2 | F | 68 | SAH | Elective | CVD sequelae | Dysfunctional gastrostomy |
| 3 | M | 57 | DM/SAH | Elective | Colorectal cancer | Necrosis of stoma |
| 4 | F | 51 | None | Emergency | Intestinal occlusion | Anastomosis dehiscence |
| 5 | M | 7 | None | Emergency | Acute appendicitis | Residual abscess |
| 6 | M | 78 | DM/COPD | Emergency | PPU | Evisceration |
| 7 | M | 36 | None | Emergency | Acute cholecystitis | Bleeding from vesicular bed |
| 8 | F | 45 | None | Emergency | Intestinal obstruction | Evisceration |
| 9 | M | 47 | Epilepsy | Emergency | Sigmoid volvulus | Anastomosis dehiscence |
| 10 | M | 70 | None | Elective | Colorectal cancer | Anastomosis dehiscence |
| 11 | F | 39 | Obesity/SAH | Emergency | Choledocolithiasis | Evisceration |
| 12 | F | 33 | DM/dyslipidaemia | Emergency | Acute appendicitis | Evisceration |
| 13 | M | 71 | SAH | Elective | Colorectal cancer | Evisceration |
| 14 | M | 20 | None | Emergency | CAT | Splenic bleeding |
| 15 | F | 42 | None | Elective | CLC | Biloma |
| 16 | M | 5 | None | Emergency | Acute appendicitis | Residual abscess |
| 17 | F | 35 | None | Elective | Inguinal hernia | Prosthetic material rejection |
| 18 | F | 73 | DM | Emergency | Intestinal obstruction | Stoma necrosis |
| 19 | F | 40 | Hypothyroidism | Elective | CLC | Biloma |
| 20 | F | 48 | None | Emergency | Intestinal occlusion | Anastomosis dehiscence |
| 21 | M | 77 | DM/SAH | Elective | CVD sequelae | Dysfunctional gastrostomy |
CLC: chronic lithiasic cholecystitis; DM: diabetes mellitus; COPD: chronic obstructive pulmonary disease; CVD: cerebrovascular disease; SAH: systemic arterial hypertension; T: type; CAT: closed abdominal trauma; PPU: perforated peptic ulcer.
Of the 21 reoperated patients, there were slightly more females (52.38%) than males (47.62%), which differs to a degree from studies such as those by Bannura et al.11, Morris et al.,12 García Vega et al.13 and Sah et al.14, and the major randomised, multi-centre study by van Ruler et al.15
With regard to age group, most reoperations were performed on patients between the 70 and 79-year age group and in the 40–49-year age group, at 23.8%. These findings are similar to those of Sah et al.,14 Bannura et al.,11 van Ruler et al.15 and Morris et al.12 However, it is important to highlight that by taking various age groups into account, most of the reoperated patients were aged between 20 and 59 years.
The percentage of abdominal reoperations found was 2.31% (21 patients), a lower number than those reported in the series of Hutchins et al.1 at 5.3%, Morris et al.12 at 5.8% and Bannura et al.11 at 6.4%. There are studies that report lower percentages of reoperation, such as that of Sah et al.14 at 2.19%. Other authors report higher percentages of reoperation in very heterogeneous groups of patients, such as that of García et al.13 at 10.6%, Doeksen et al.16 at 12.45%, in a specific group of patients treated by colorectal surgery, and Manrique et al.17 at 33.9% of reoperations in patients with organ transplants.
Most abdominal reoperations followed emergency abdominal surgery on admission of the patient at 61.91%. The results of the study by Hutchins et al.1 report 80% abdominal reoperation secondary to emergency surgery. The number is higher in the study by García et al.13 at 83.33% and Höer et al. obtain the lower figure of 62.5%.18
Intra-abdominal collection and evisceration (23.8%) was the most frequent indication for reoperation. The study by Hutchins et al.1 puts intra-abdominal collection as the primary indication, Chichom et al.19 report it at 50.8%, which is the greatest percentage as an indication for reoperation. Anastomosis dehiscence presented in 19.04% (in second place as an indication for reoperation), in contrast to Bannura et al.11 who place it first, at 36%.
There was a mean of 8 days between the first surgery and reoperation, with a maximum of 20 days and a minimum of one day. Most of the patients were operated in less than 6 days. The study by Bannura et al.11 reported a mean of 7.1 days, with a maximum of 25 and minimum of 1 day. Hutchins et al.1 report a mean of 6.94 days, Doeksen et al.16 4.2 days and García et al.13 report that the majority of their patients were reoperated within the first 7 days.
The majority of the reoperated patients (66.6%) had no personal history of disease. However, diabetes mellitus (n=6) and high blood pressure predominated in those that did; García et al.13 report a prevalence of the latter at 47.7%.
Postoperative complications presented in 23.8% of the reoperated patients. Surgical wound dehiscence was the most frequent at 60%. Chichom et al.19 reported 35% morbidity post reoperation, mostly due to infection of the wound site at 82.29%. This coincides with the 46% found by Bannura et al.11; however, in the study by Sah et al.,14 pleural effusion prevailed at 13%.
14.3% of the reoperated patients in our study died. This is a higher number than the 10% reported by Bannura et al.11 and contrasts with the 29.4% reported by Hutchins et al.,1 the 35.93% reported by Höer et al.,18 the 20% by García et al.,13 the 18.1% by Chichom et al.,19 and the 11.11% reported by Sah et al.14
ConclusionsOur study reports a percentage of abdominal reoperation slightly lower than that of most of the published series; reoperation predominated in patients of advanced age. Nonetheless, it continues to be seen in younger patients. There is no significant difference in terms of gender; there is a slightly higher tendency in females. Emergency surgery most frequently required reoperation, probably due to the technical difficulty of this type of surgery. Diagnoses of intra-abdominal collection and evisceration most frequently required abdominal reoperation. According to the authors reviewed, this might be due to many factors such as: the skill of the surgeon, the type of suture, the patient's comorbidities and diagnosis, amongst others. It should be mentioned that the frequency of these complications has remained practically unaltered over recent years. Most of the reoperated patients had no personal history of disease, however, the patients with comorbidities were of advanced age, with major complications and some even died. As far as is possible, therefore, special care should be taken in these patients to avoid abdominal reoperation of any type.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestsThe authors have no conflicts of interest to declare.
Please cite this article as: Pérez-Guerra JA, Vázquez-Hernández M, Ramírez-Moreno R, López-García FR. Reintervenciones abdominales: prevalencia en cirugías electivas y urgencias. Cir Cir. 2017;85:109–113.