



A gallstone colonic ileus is a very rare condition.
Clinical caseThe case is reported of an 87 year-old patient who came to the Emergency Department due to an intestinal obstruction of several days onset, which was caused by a gallstone affected sigmoid colon.
ConclusionColonic gallstone ileus is a rare disease that usually occurs in older patients due to the passage of large gallstone directly from the gallbladder to colon, through a cholecystocolonic fistula. It has a high morbidity and mortality.
La obstrucción intestinal en colon, como consecuencia de un cálculo biliar, es una enfermedad extremadamente rara, que suele desarrollarse en muy pocas ocasiones.
Caso clínicoPresentamos el caso de una paciente de 87 años, que acude al servicio de urgencias por cuadro compatible con obstrucción intestinal de varios días de evolución, como consecuencia de un cálculo impactado en colon sigmoide.
ConclusiónEl íleo biliar colónico es una enfermedad muy rara, que ocurre generalmente en pacientes de edad avanzada, como consecuencia del paso del cálculo de gran tamaño desde la vesícula al colon, a través de una fístula colecisto-cólica, siendo una enfermedad con una elevada morbimortalidad.
Intestinal obstruction caused by a gallstone trapped in the colon is an extremely rare entity,1 which usually occurs due to the passage of a large stone through a cholecystocolonic fistula.
ObjectiveWe present the case of a gallstone ileus at the level of the sigmoid colon.
Clinical caseAn 87-year-old woman with a history of systemic high blood pressure, osteoporosis, polyarthritis, and polymyalgia rheumatica attended the emergency department with abdominal pain associated with vomiting and constipation of 3 days onset.
On examination the patient was in an acceptable state of general health, afebrile and haemodynamically stable; with a distended abdomen tympanic on percussion, generally painful but with no signs of peritoneal irritation on palpation, no hernia defects were identified. A minimal amount of faeces was found on rectal examination.
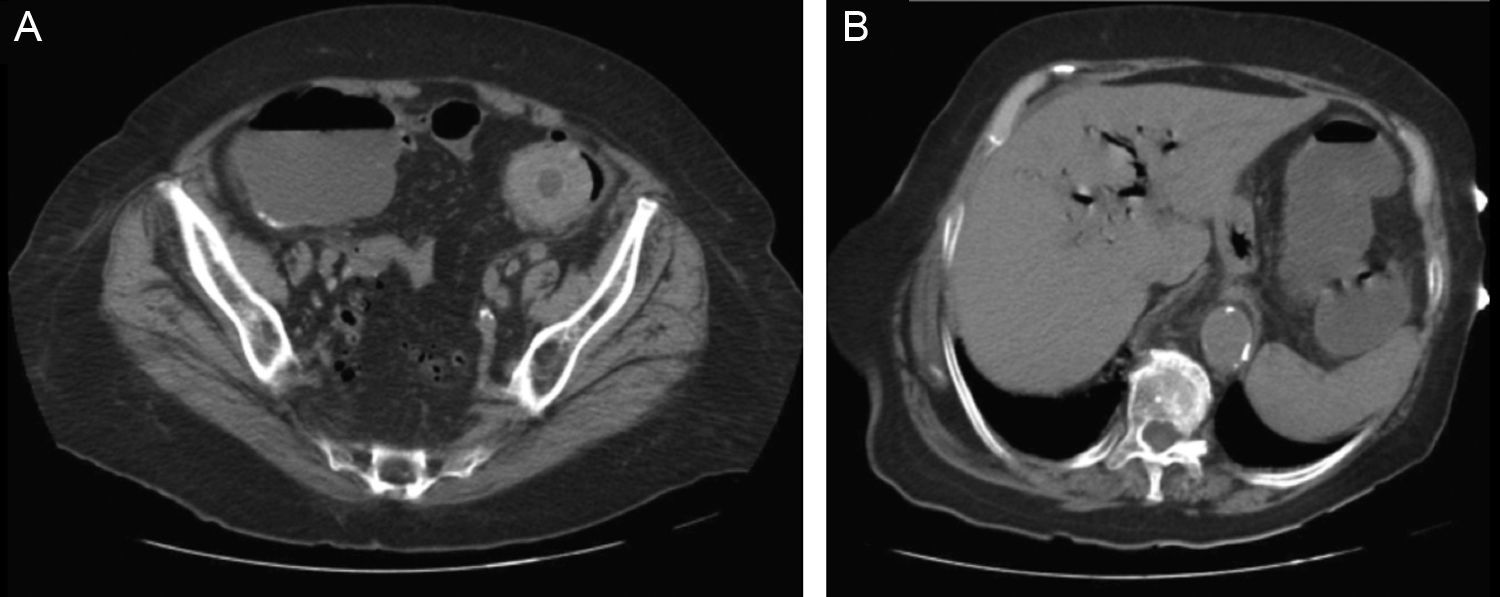
Laboratory tests were requested in the emergency department which revealed elevated C reactive protein, and all the other parameters were within normal limits. Plain abdominal X-ray showed signs compatible with intestinal obstruction at the level of the descending colon. Because a mechanical intestinal obstruction was suspected, computed axial tomography (CAT scan) was requested to confirm the cause of the obstruction, which revealed marked dilatation of the entire colon up to the sigmoid colon, and showing an image of 5cm entirely occupying the lumen. Likewise, aerobilia was identified predominating in the left liver lobe, gas in the cystic duct and the bile duct; a collapsed gallbladder with gas in its interior, adjacent to the hepatic flexure of the colon. All of which were findings compatible with gallstone ileus at the level of the sigmoid colon (Fig. 1A and B).
 CAT scan image with stone impacted in the sigmoid colon and aerobilia.")
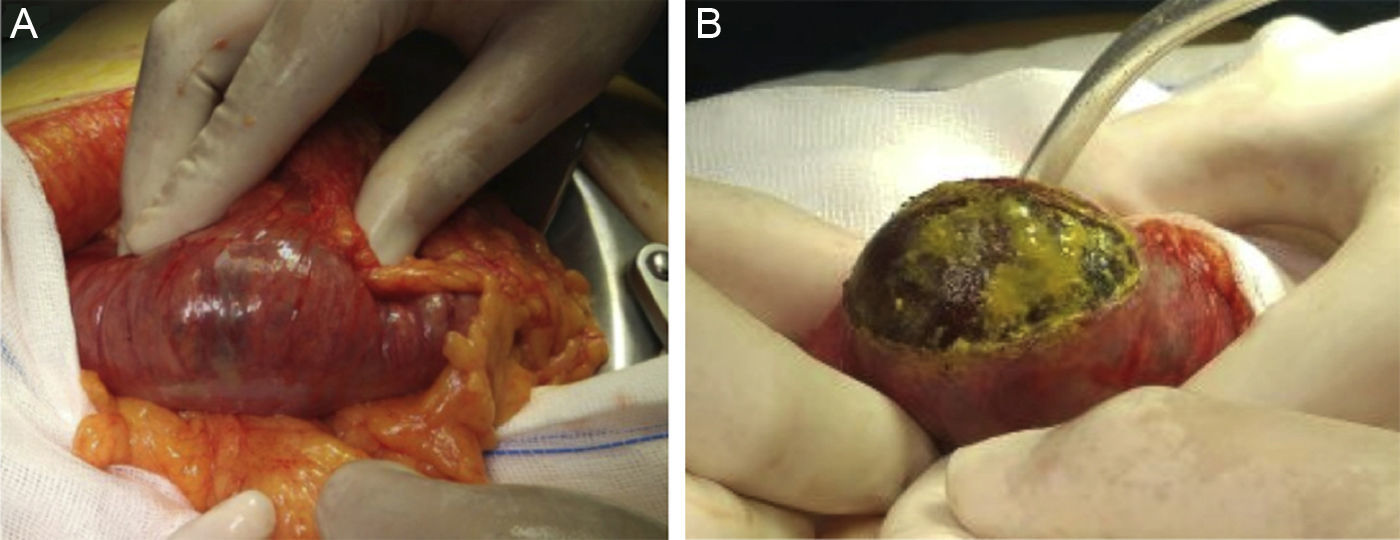
Due to the clinical picture and the progressive increase in laboratory study levels, and the clinical deterioration of the patient, with pain and abdominal distension increasing since her admission, emergency surgical intervention was decided. An exploratory laparotomy was performed which identified marked dilatation of the colic structure, with apparent calibre changes at the level of the sigmoid colon, where the impacted gallstone was palpated. The gallstone was disimpacted, and moved proximally towards the transverse colon, where a colotomy was performed, the gallstone was removed and then a simple closure of same was performed (Fig. 2A and B). No surgical manoeuvres were performed on the gallbladder or the cholecystocolonic fistula.
 Location of the stone. Colotomy for extracting the stone.")
The patient developed acute respiratory failure in the immediate postoperative period, which evolved favourably until diuresis and creatinine levels normalised, atrial fibrillation was identified with slow ventricular response, de novo, and acute confusional syndrome. The patient also presented a deep surgical wound infection which lengthened her stay in our department for daily dressings. She was discharged home on the 20th postoperative day.
DiscussionGallstone ileus is a very rare disease, which occurs as a complication of gallstones, and constitutes 1%–4% of the causes of mechanical intestinal obstruction.1,2 It is caused by the migration of one or several stones through a biliodigestive fistula, which tend to develop in patients with a history of acute cholecystitis (25%–75%), although it can also occur in patients with no history of gallbladder disease and even in cholecystectomised patients.3 Most commonly a cholecysto-duodenal fistula forms (65%–75%), which enables the stone to pass and progress through the digestive tract until it becomes impacted at any level. The most common location for obstruction is the terminal ileum (70%) followed by the proximal jejuno-ileum (25%), the duodenum (5%), or the colon (2%). It is rarer for a cholecystocolonic fistula to develop (10%–25%), which enables the stone to pass directly to the colon, there are even cholecystogastric fistulas (5%).4
It is important to take the stone's size and morphology into account, since it is difficult for stones smaller than 2–2.5cm to cause an intestinal obstruction at the level of the large bowel unless there are altered bowel dynamics, or a reduction in its lumen, due to benign disease, for example diverticulitis, or an undiagnosed malignant process.5 Our patient's stone was larger than 5cm, impacted at the level of the sigmoid colon, and she had no underlying disease (Fig. 3).

This picture generally occurs in women of advanced age, with multiple associated comorbidities, which can mask the symptoms,1–3,6 giving rise to a delay in diagnosis and high morbidity and mortality. Although it usually manifests as symptoms of mechanical intestinal obstruction with pain and distended abdomen, associated with vomiting and constipation, it is not uncommon for a definitive diagnosis to be reached intraoperatively.4,5 However, there are various diagnostic options which help to determine the cause of this clinical picture.
It is essential first to perform a plain X-ray of the abdomen, whenever an obstruction is suspected, where we can identify a pathognomonic triad (40%–50%) of this disease, such as: intestinal distension, pneumobilia and ectopic gallstone, which can be seen on our patient's X-ray.5 Ultrasound reveals the current state of the gallbladder and the bile duct (gallstones and intra-gallbladder ultrasound image), whether there is a bilioenteric fistula, with the presence of pneumobilia, and can identify a stone in the bowel lumen. An abdominal CAT scan shows an image of the gallstone and the exact location of the intestinal obstruction, air in the gallbladder and the fistula. This was the definitive diagnostic test for our patient.1,2,4
Once the clinical picture has been diagnosed, the therapeutic approach needs to be decided, taking these patients’ characteristics into account. There are data where the picture has been resolved by colonoscopy which would enable any underlying disease to be discounted. However, the most common approach is surgical, after basic support measures. In the case of our patient, endoscopy was ruled out because her symptoms worsened over a few hours. Surgery should resolve the obstruction, and cholecystectomy and repair of the fistula should be left for a second occasion, if there are clinical signs of recurring biliary disease.3 Surgery involves a laparotomy or exploratory laparoscopy, identifying, disimpacting and removing the stone by enterotomy or intestinal resection if there is involvement of the colon wall, associated disease, intestinal perforation etc. It is important to palpate the gallbladder and the entire bowel meticulously to search for other stones, which might cause subsequent occlusion.1–3,5
The morbidity described in these patients is 50%, the most common complication being surgical wound infection, which as we described earlier, was the main cause for our patient's admission.3,6,7
ConclusionWe would stress that this disease is an emergency that is difficult to diagnose, due to the characteristics of the patient, with a high rate of morbidity and mortality. It benefits from early intervention aimed solely at resolving the obstruction, with cholecystectomy on a second occasion, in patients with repeated symptoms and confirmed gallstones.
Conflict of interestsThe authors have no conflicts of interests to declare.
Please cite this article as: Marenco-de la Cuadra B, López-Ruiz JA, Tallón-Aguilar L, López-Pérez J, Oliva-Mompeán F. Íleo biliar colónico: una rara causa de obstrucción intestinal. Cir Cir. 2017;85:440–443.