


Carcinoid of the small intestine, is a well-differentiated neuroendocrine tumour that rarely presents with clinical signs. This tumour can be associated with other conditions, such as inflammatory bowel disease, presenting a wide range of symptoms. In some cases they have an aggressive and highly symptomatic behaviour; thus, clinical suspicion must be high to make an early diagnosis.
Clinical caseA 60 year-old male patient with Crohn's disease and gastrointestinal symptoms attributed to this disease within the last year. He presented with intestinal obstruction initially treated with conservative management with no improvement. Exploratory laparotomy was performed finding a mesenteric tumour that caused the bowel obstruction.
Bowel resection with primary anastomosis was performed. The pathology report showed an intestinal carcinoid tumour with lymph node metastases. The patient recovered well, and was discharged without complications to continue medical treatment and follow-up by the Oncology department.
ConclusionIn almost 42% of the cases, the most common site of carcinoid tumours is the small intestine, and of these, 41% are presented as locoregional disease. Patients with Crohn's disease present a higher incidence. In these cases, the most common presentation is an acute intestinal obstruction (90%). Surgery is usually curative, and follow up is important as the symptoms of Crohn's disease can hide any recurrence.
El carcinoide intestinal es una neoplasia neuroendocrina del intestino delgado que en pocas ocasiones se presenta con manifestaciones clínicas. Estos tumores pueden estar asociados a otras patologías, como enfermedad inflamatoria intestinal, y tienen un rango amplio de sintomatología, aunque la mayoría crecen lentamente y producen síntomas poco específicos. En algunos casos tienen un comportamiento agresivo y altamente sintomático, por lo que la sospecha clínica debe ser alta para realizar un diagnóstico temprano.
Caso clínicoMasculino de 60años con antecedente de enfermedad de Crohn y síntomas gastrointestinales de un año de evolución, atribuidos a dicha enfermedad. Presentó cuadro de oclusión intestinal sin mejoría con manejo conservador. Se realizó laparotomía exploradora, encontrando tumoración del mesenterio, la cual condicionaba una obstrucción intestinal mecánica.
Se realizó resección intestinal con anastomosis primaria. El reporte histopatológico evidenció un tumor carcinoide intestinal con metástasis ganglionares. Evolucionó adecuadamente y fue dado de alta para continuar tratamiento médico y seguimiento por oncología.
ConclusionesEl sitio más común de presentación de los tumores carcinoides es el intestino delgado hasta en un 42% de los casos; de estos, el 41% se presentan como patología locorregional. Existe una mayor incidencia en pacientes con enfermedad de Crohn y en estos casos, la presentación más común es un cuadro agudo de obstrucción intestinal (90%). La cirugía suele ser curativa y el seguimiento es importante, ya que los síntomas de la enfermedad de Crohn pueden ocultar alguna recidiva.
Carcinoid of the intestine is a neuroendocrine neoplasia of the small intestine which usually presents insidiously, due to its slow growth and its minimally aggressive behaviour. It is associated with other pathologies, such as non-specific chronic ulcerative colitis and Crohn's disease. Symptoms can be non-specific and can be confused with the abovementioned diseases or functional gastrointestinal disorders.1
Clinical caseA 60-year old male patient with a diagnosis of Crohn's disease of 10 years evolution, treated with mesalazine.
A year prior to admission, the patient started to experience non-specific, generalised, abdominal pain associated with intermittent episodes of diarrhoea with no mucous or blood, which was managed medically; it partially improved temporarily. He attended the emergency department due to increased abdominal pain, and nausea without vomiting. On physical examination his abdomen was distended, there was increased peristalsis in the lower quadrants, generalised pain on superficial and deep palpation, tympanic on percussion, with no signs of peritoneal irritation. The initial results of the laboratory tests showed no changes; abdominal tomography was requested, which showed thickening of the intestinal wall with signs of intestinal occlusion, inflammatory changes in the mesenteric fat, mesenteric adenopathies and free fluid in the pelvic cavity.
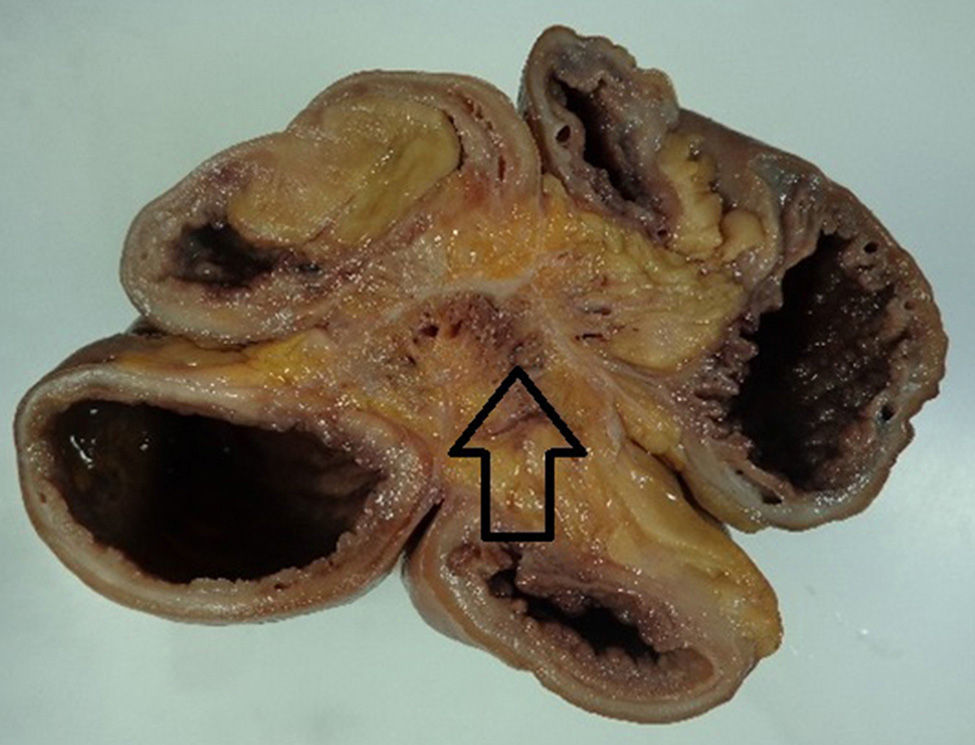
It was decided to opt for conservative management with naso-gastric tube. However, 24h after the patient was admitted, his pain increased and he presented leukocytosis of 11,800/mm3, with 3% bands, and therefore an exploratory laparotomy was performed. A fibrotic tumour was found in the mesentery 20cm from the ileocaecal valve (Fig. 1), which was causing obstruction and had involved approximately 60cm of the loops of the small intestine, including the ileocaecal valve with inter-loop adherences, and 4 extracapsular punctiform lesions of hard consistency, 3mm in diameter in the anterior surface of the liver.

A 60cm resection was made of the terminal and blind ileum, with ileo-ascending anastomosis, latero-lateral mechanics, as well as a biopsy of one of the hepatic lesions.
The patient recovered satisfactorily, and was discharged on the seventh postoperative day with adequate oral tolerance and gastrointestinal function.
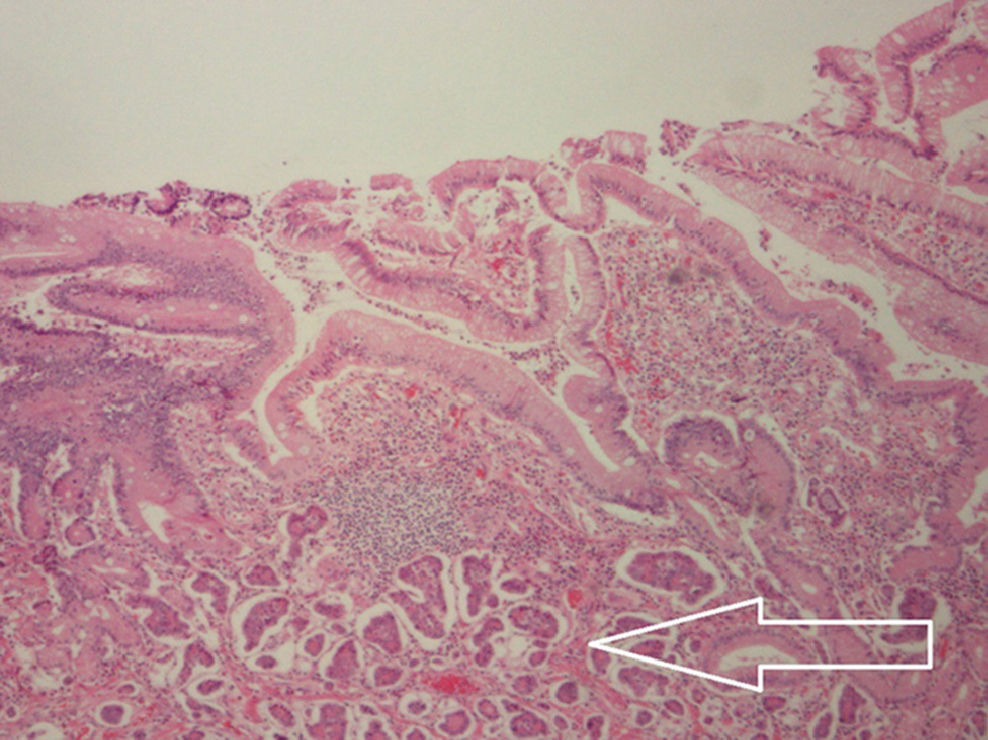
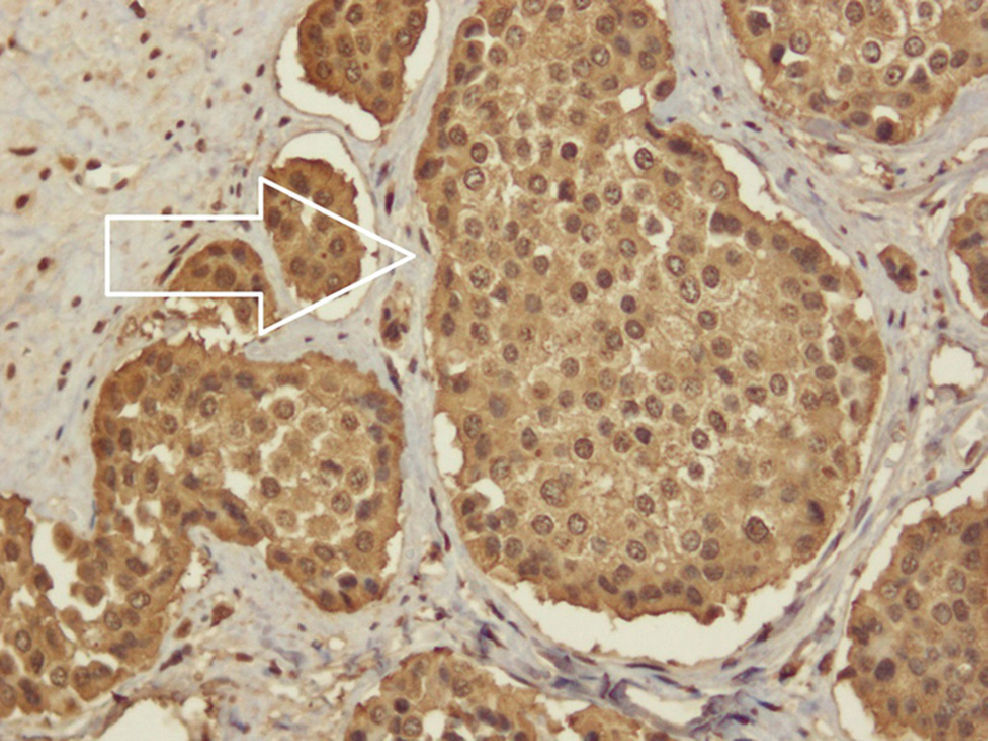
The pathology report showed a grade one neuroendocrine neoplasia, with negative surgical borders. The tumour was carcinoid, its longest diameter was 2.5cm and the shortest was 2cm, and it was infiltrating the serosa, as well as 4 out of 15 lymph nodes with metastases (Figs. 2 and 3).
 which is infiltrating the lamina propria, muscularis mucosae, submucosa, muscularis propria and serosa.")

Carcinoid of the intestine is the most common malignant tumour of the distal small intestine. In up to 42% of cases it presents in the small intestine, and 41% of these cases present as locoregional disease. Its incidence is increasing, at 0.67/100,000 inhabitants with carcinoid tumours of the jejunum and ileum; it is similar for both sexes, and the average age of presentation is 66. Although its prevalence is relatively high, the presence of symptoms or carcinoid syndrome is very rare.1 When it presents clinically, 12% of patients have distant metastases, whereas carcinoid syndrome only occurs in one out of 300,000 patients with this tumour.2
Carcinoid tumours form part of the neuroendocrine neoplasias that derive from the enterochromaffin cells of the intestinal crypts, which share a common source in the ectoderm; these cells synthesise serotonin from tryptophan absorbed in the gastrointestinal tract.3 Two enzymes are involved in serotonin synthesis: tryptophan hydroxylase, which catalyses the conversion of tryptophan in 5-hydroxyindolacetic acid (5-HIIA), and monoamine oxidase: 5-HIIA is metabolised by the kidney, and its levels increase in urine in the presence of a carcinoid tumour, which supports the diagnosis of this disease.3,4
Clinical presentation is due to the pathophysiological mechanisms involved, and symptoms can be secondary to the tumour or to carcinoid syndrome; manifestations are acute, and chronic, depending on the evolution time of the tumour. Intestinal obstruction is the most common acute presentation (90% of cases) and occurs secondary to the desmoplastic reaction that this generates, in both the intestine and the mesentery. This reaction can cause acute mesenteric ischaemia in 30% of cases. Another acute intestinal manifestation is bleeding from the digestive tract, which is usually not abundant, and due to its location, can be difficult to identify.3,4
Chronic intestinal manifestations usually present with a history of pain over several months or years, and are usually diagnosed mistakenly as malabsorption syndrome or irritable bowel syndrome, due to the association with changes in bowel habits. Chronic presentation can even reflect an associated condition which is related to carcinoid tumours, such as Crohn's disease.4
Patients with Crohn's disease present more frequently with gastrointestinal tumours compared with the general population. The malignant strains associated with this disease are adenocarcinoma, lymphoma and epidermoid carcinoma.5
There is evidence of the association between patients with Crohn's disease and intestinal carcinoid. West et al.6 presented a series of cases where they concluded that carcinoid tumours are 15 times more common in patients with Crohn's disease, a 3.6% incidence compared with 0.25% in the control group, in addition to the increased risk of presenting carcinoid tumours, the symptoms from this tumour can be falsely attributed to Crohn's disease, and this is why there are delays in diagnosis.7
The secondary presentation of carcinoid syndrome only occurs when there are liver metastases, as these secrete serotonin, as well as other derivatives of tryptophan metabolism. The most common manifestations of this syndrome include: facial reddening, diarrhoea, abdominal pain, telangiectasias, oedema and signs of cardiac dysfunction.4
Abdominal tomography is the study of choice for diagnosing carcinoid tumours of the intestine. It is used to detect tumours, metastasis, and to identify the anatomy. Abdominal ultrasound is the most sensitive test for liver metastases of less than 1cm.8 In terms of functional tests; radionuclide scanning with 111In-octreotide has 83% diagnostic sensitivity and 100% positive predictive value. Useful markers in diagnosis are chromogranin A and 5-HIIA, which has 88% specificity and 35% sensitivity; however, these can be high in the presence of other types of neuroendocrine tumours.3
The principal treatment objective is to increase survival, and to control symptoms and improve quality of life. This can be achieved by wide surgical resection, including the mesentery and lymph nodes. Revision of the entire intestine is essential, as there are other carcinoid tumours of the intestine in 25% of cases. If full resection is not possible due to retroperitoneal spread or spread to the large vessels, cytoreductive surgery should be performed, with a view to reducing or normalising 5-HIIA levels, to reduce systemic symptoms and prevent local complications. There are several options in cytoreductive therapy, such as ablation with radiofrequency, cryotherapy and surgical metastasectomy.4,9 A survival of 71% at 5 years and complete resolution of the symptoms of carcinoid syndrome between 4 and 120 months in 86% of cases was reported in a meta analysis where partial cytoreductive hepatectomy was performed. In cases where the metastases are unresectable, arterial embolism can be performed to reduce the tumour and the symptoms of carcinoid syndrome.9
The response to chemotherapy is variable, it rarely exceeds 30%. Commonly used drugs are 5-fluorouracil and streptozocin, although results are generally not favourable and they are only used palliatively. Radiotherapy does not play a therapeutic role and its use is limited to painful bone metastases or metastases of the central nervous system.4,9
The prognosis and follow-up of patients with intestinal carcinoid depends on their clinical condition at the time of diagnosis, and the therapy that they have received. Monitoring with serum markers such as chromogranin A and 5-HIAA should be carried out routinely every 6 months, and for the first 3 years, and subsequently annually. Abdominal tomography is recommended during the first 3 years, and subsequently the need for this test should be evaluated with laboratory findings and clinical symptoms. The decision to suspend monitoring after the fifth year post treatment depends on the clinical evolution during this time.10
ConclusionsCarcinoid tumours are rare and have a wide range of symptoms; the majority are slow-growing and have non-specific symptoms. Therefore early suspected diagnosis and appropriate treatment will be of greatest benefit to patients.
Conflict of interestsThe authors have no conflict of interest to declare.
Please cite this article as: Mussan-Chelminsky G, Vidal-González P, Núñez-García E, Valencia-García LC, Márquez-Ugalde MA. Tumor carcinoide intestinal: reporte de un caso. Cir Cir. 2015;83:438–441.