




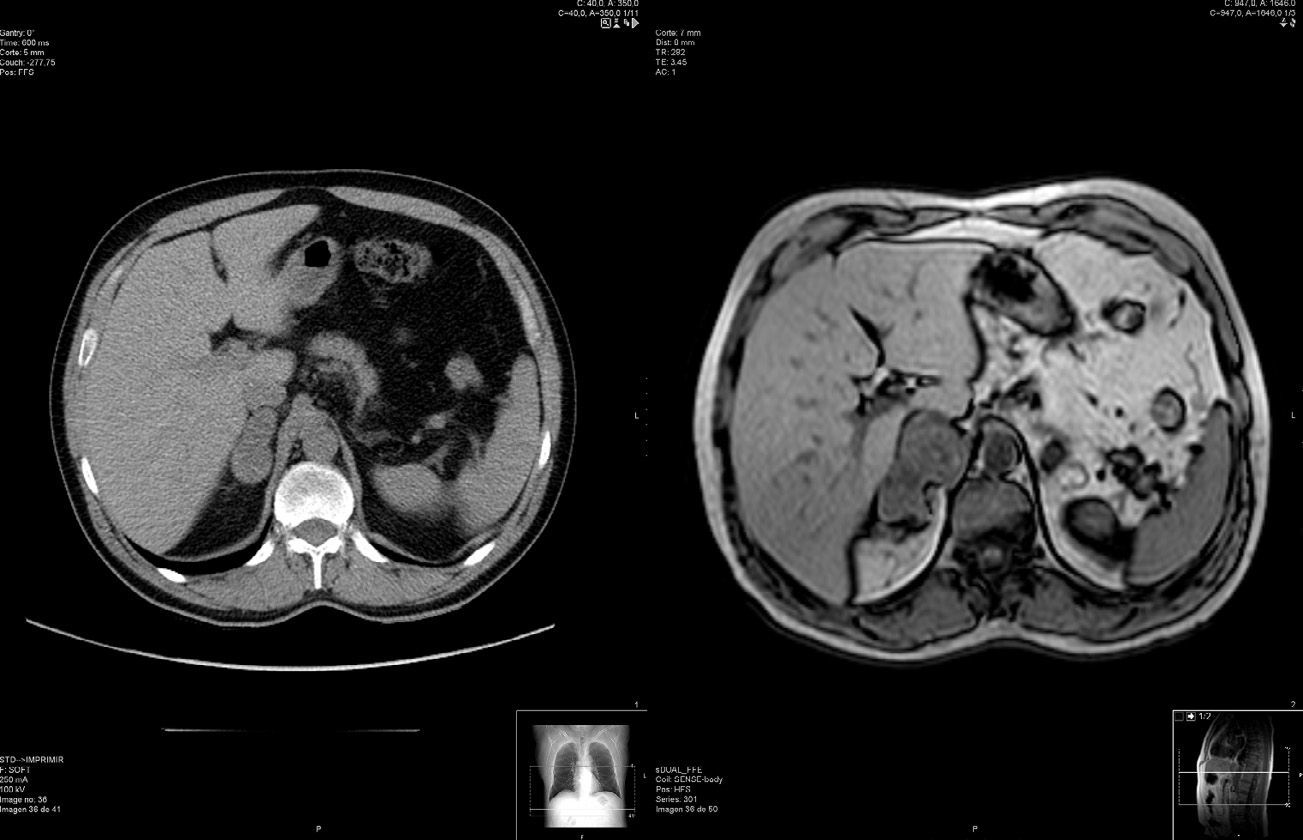
The patient is a 48-year-old male. During a CT study for pulmonary emphysema, a nonspecific nodular lesion was observed in the right adrenal gland, measuring 4×2.5×2cm. To complete the study of the incidental adrenal mass, an MRI was ordered, which showed evidence of a heterogenous right adrenal mass measuring 6.8×4.4×3.9cm that was in close contact with the pillar of the diaphragm and the inferior vena cava, which was being compressed (Fig. 1). These findings were compatible with carcinoma or a metastatic lesion. At the time of the MRI, the patient expressed the appearance of constant, mild pain in the right hypochondrium.

General examination showed a patient with normal habits who was normotensive, and physical examination showed no alterations.
On the initial complementary tests, the results from the hemogram, ESR, and general biochemistry (including transaminases and ions) were normal. Tumor marker levels (alpha-fetoprotein, CEA, CA 19.9, CA 125, CA 15.3 and PSA) were also normal. Metanephrine study in 24h urine, plasma catecholamine and plasma cortisol were normal. ACTH was not suppressed, and the aldosterone/plasma renin activity ratio was normal. The hormone study showed urinary free cortisol, dopamine, adrenaline and noradrenaline in 24h urine, estradiol, progesterone, 17-OH-progesterone, testosterone, androstenedione and dehydroepiandrosterone sulfate within normal limits.
Given the diagnosis of a rapidly growing non-functioning adrenal mass, we decided to operate and performed a laparoscopic right adrenalectomy with an anterior subcostal transperitoneal approach.
The surgery was difficult due to the retrocaval location of the gland; macroscopic infiltration of the liver capsule was observed. We completely resected the gland as well as the area of macroscopic infiltration.
The postoperative period was uneventful, and the patient was discharged 6 days after the procedure.
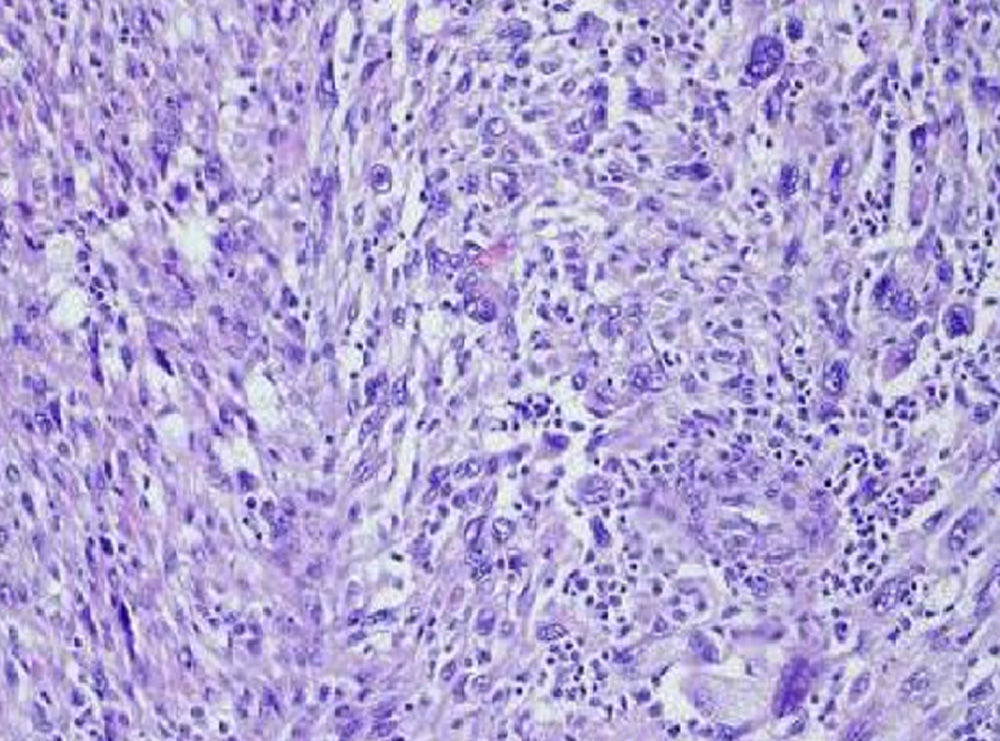
The pathology study of the surgical specimen reported an adrenal gland weighing 47g that contained a non-encapsulated mass measuring 7×4.5×4.2cm with a cut surface that appeared fleshy and had small hemorrhagic areas. Microscopically, the adrenal gland was overcome by an extensive mass with a solid pattern and areas of necrosis. Some areas showed a clustered pattern with spindle cells, although the majority presented an atypical cytological appearance that was highly pleomorphic, with large-size cells and marked irregularities in nuclear size, lobulated nuclei and prominent nucleoli, and a mitotic rate of 10 mitoses per high power field. Immunohistochemistry showed intense positivity for Ki-67 (>75%) and negativity for keratin 8/18, keratins AE1-AE3, protein S 100, HMB45, melan A, chromogranin and synaptophysin, with intense staining for vimentin, actin and desmin (Fig. 2).
 and negative for keratin 8/18, keratins AE1-AE3, S-100 protein, HMB45, melan-A, chromogranin and synaptophysin, showing intense stain for vimentin, actin and desmin. The pathology study showed the lesion had a markedly atypical cytological appearance that was highly pleomorphic, with large cells and marked irregularities in nuclear size, lobulated nuclei and prominent nucleoli, and a mitotic rate of 10 mitoses per high power field (H-E 200×).")
Immunohistochemistry was intensely positive for Ki-67 (>75%) and negative for keratin 8/18, keratins AE1-AE3, S-100 protein, HMB45, melan-A, chromogranin and synaptophysin, showing intense stain for vimentin, actin and desmin. The pathology study showed the lesion had a markedly atypical cytological appearance that was highly pleomorphic, with large cells and marked irregularities in nuclear size, lobulated nuclei and prominent nucleoli, and a mitotic rate of 10 mitoses per high power field (H-E 200×).
Later follow-up studies were done every 3 months. The initial MRI study centered on the surgical site of the right adrenalectomy in order to study the post-surgery changes or any persistence of local disease; this was complemented with thoracoabdominal CT and general lab workup. The remaining follow-up studies have entailed thoracoabdominal CT and general workup. To date, and after 17 months of follow-up, the patient remains free of recurrence, both at the surgical site as well as any distant metastases.
Due to the absence of scientific evidence of residual local or distant disease in the radiological testing and the presence of free margins in the pathology study of the adrenalectomy specimen, the Oncology Department at our hospital, supported by the Oncology and Pathology Departments at the Complejo Hospitalario Universitario de Santiago de Compostela, decided not to administer adjuvant chemotherapy.
Leiomyosarcomas (LMS) are mesenchymal tumors derived from smooth muscle cells, whose most frequent location is the myometrium, retroperitoneum and respiratory tract.1,3 Primary LMS of the adrenal glands develops from smooth muscle structures, such as the main adrenal vein and its tributary branches. Its primary form is rare, and metastatic adrenal LMS or extension from the retroperitoneum are more frequent.1–9 The first case published in the international literature was in 1981 by Choi and Liu.2 Since then, a few more than 20 cases have been published. An extremely rare variety is pleomorphic LMS, for which we have found only 4 cases published in the international literature.1,3–5
Primary adrenal LMS do not predominantly affect either of the sexes, nor do they present laterality. They are more frequent during middle age, and cases have been reported in patients from 25 to 68 years of age.1 There are no well-defined risk factors, although a greater incidence has been found in immunosuppressed patients infected by HIV and Epstein–Barr virus.1,10
Rapid growth is characteristic, as observed in this case (Fig. 1), and lesions smaller than 5cm are usually asymptomatic. The most frequent symptoms are abdominal and lumbar pain, the sensation of a mass effect in the hypochondrium, as well as asthenia and weight loss.10 Almost all the published cases with lesions larger than 8cm presented distant metastasis at the time of diagnosis.1,3,10
Laboratory and hormone analyses do not usually detect significant alterations. As for imaging studies, no specific characteristics for these tumors have been described, although right tumors frequently extend along the vena cava inferior to the right pillar of the diaphragm.1,7,8 In our case, the tumor extended up to the liver capsule.
In all reported cases, diagnosis is made during surgery or autopsy. Adrenalectomy is the treatment of choice, although in many cases it was associated with nephrectomy due to the tumor size.1,3 The role of chemotherapy and radiotherapy is controversial, although they have been used to control pain and metastatic lesions.1,6
Pathologically, LMS are solid fleshy tumors that occasionally have areas of necrosis. Histologically, they present a fascicular pattern with spindle cells, lobulated nuclei, prominent nucleoli and a high mitotic rate, with a certain degree of nuclear and nucleolar atypia. Immunohistochemically, the cells are positive for vimentin, actin and desmin (Fig. 2).9
The prognosis for primary adrenal LMS is poor and is related to tumor stage, local invasion and distant metastasis. Microscopically, the number of mitosis per high power field seems to be related with survival4: mean survival is 8.4 months in patients with more than 10 mitoses/field and reaches 48 months in cases with less than 10.10
Primary adrenal pleomorphic LMS is an extremely rare variation, and only 4 cases were found on PubMed.1–5 With a high grade of malignancy, histologically they behave as a non-encapsulated mass with a solid pattern, areas of necrosis, and a defined cytological atypia. They are highly pleomorphic, with large cells and very irregular nuclear sizes, lobulated nuclei, prominent nucleoli, and a high mitotic rate per high power field. Out of the 4 cases, 3 were women, and mean age was 49 (28–63). In 2 cases, the predominant symptom was abdominal pain, while one was an incidentaloma. Three cases presented metastasis at diagnosis or in the following 12 months. Treatment was affected by extraglandular involvement; 2 patients received chemotherapy and radiotherapy, one patient underwent surgery, and the remaining case treatment is unknown.1,3–5
Please cite this article as: Pereira-Beceiro J, Rodríguez-Alonso A, Janeiro-Pais JM, Alvarez-Fernández JC, Durana Tonder C. Leiomiosarcoma pleomórfico adrenal, un tumor suprarrenal maligno infrecuente. Cir Esp. 2015;93:256–258.
