







Cirugia mínimamente invasiva de pared abdominal
Más datosSurgeons use abbreviations and acronyms frequently to describe surgical techniques. Recent advances and innovations in repair of abdominal wall hernias, have given rise to a plenitude of novel acronyms. For each small deviation of an existing technique authors have proposed a novel acronym. Since an acronym is most of times not self-explaining it is often hard to understand literature, lectures, symposia programs and discussions in social media. Regularly, we discover different acronyms used for the same procedure and sometimes the same or similar acronyms are used for different techniques. A clear and non-ambivalent description of surgical techniques in the literature is most valuable to summarize scientific evidence in systematic reviews and meta-analyses.
We would like to propose a more rational use of abbreviations to describe hernia repair techniques based on the type of access, type of hernia, mesh position, type of mesh used and type of mesh fixation.
Los cirujanos utilizan con frecuencia abreviaturas y acrónimos para describir las técnicas quirúrgicas. Los recientes avances e innovaciones en la reparación de las hernias de la pared abdominal han dado lugar a una plétora de novedosas siglas. Para cada pequeña desviación de una técnica existente los autores han propuesto un nuevo acrónimo. Dado que un acrónimo la mayoría de las veces no se explica por sí mismo, a menudo es difícil de entender la literatura, las conferencias, los programas de simposios y los debates en las redes sociales. Regularmente descubrimos que se utilizan diferentes acrónimos para el mismo procedimiento y, a veces, se utilizan acrónimos iguales o similares para diferentes técnicas. Una descripción clara y sin ambivalencias de las distintas técnicas quirúrgicas que podemos encontrar en la literatura es muy valiosa para resumir la evidencia científica en revisiones sistemáticas y metaanálisis.
El objetivo del presente escrito es proponer un uso más racional de las abreviaturas para describir las técnicas de reparación de las hernias en función del tipo de acceso, el tipo de hernia, la posición de la malla, el tipo de malla utilizada y el tipo de fijación de la misma.
Surgeons use abbreviations and acronyms frequently to describe surgical techniques. The recent advances and innovations in repair of abdominal wall hernias, have given rise to a plenitude of novel acronyms. For each small deviation of an existing technique authors have proposed a novel acronym. Since an acronym is most of times not self-explaining it is often hard to understand literature, lectures, symposia programs and discussions in social media. Regularly, we discover different acronyms being used for the same procedure and sometimes the same or similar acronyms are used for different techniques. A clear and non-ambivalent description of surgical techniques in the literature is most valuable to summarize scientific evidence in systematic reviews and meta-analyses.
We would like to propose a more rational use of abbreviations to describe hernia repair techniques based on the type of access, the type of hernia, the mesh position, the type of mesh used and the type of mesh fixation.
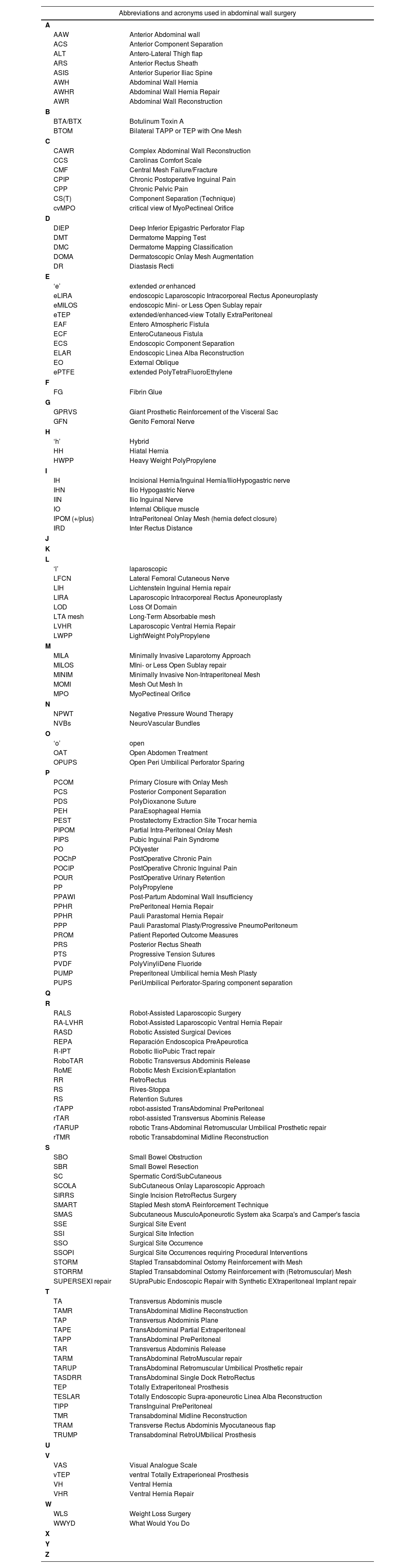
Current state of the acronyms and eponyms in hernia repair techniquesWith a search on which acronyms are being used we want to summarize the current status and the foundation why a proposal for rationalisation is important. We show the results in Table 1 but we do realise that many abbreviations or acronyms that also have been used might not have been included.
A list of abbreviations or acronyms used in relation to abdominal wall surgery, but we do realise that many abbreviations or acronyms that also have been used are not included.
| Abbreviations and acronyms used in abdominal wall surgery | |
|---|---|
| A | |
| AAW | Anterior Abdominal wall |
| ACS | Anterior Component Separation |
| ALT | Antero-Lateral Thigh flap |
| ARS | Anterior Rectus Sheath |
| ASIS | Anterior Superior Iliac Spine |
| AWH | Abdominal Wall Hernia |
| AWHR | Abdominal Wall Hernia Repair |
| AWR | Abdominal Wall Reconstruction |
| B | |
| BTA/BTX | Botulinum Toxin A |
| BTOM | Bilateral TAPP or TEP with One Mesh |
| C | |
| CAWR | Complex Abdominal Wall Reconstruction |
| CCS | Carolinas Comfort Scale |
| CMF | Central Mesh Failure/Fracture |
| CPIP | Chronic Postoperative Inguinal Pain |
| CPP | Chronic Pelvic Pain |
| CS(T) | Component Separation (Technique) |
| cvMPO | critical view of MyoPectineal Orifice |
| D | |
| DIEP | Deep Inferior Epigastric Perforator Flap |
| DMT | Dermatome Mapping Test |
| DMC | Dermatome Mapping Classification |
| DOMA | Dermatoscopic Onlay Mesh Augmentation |
| DR | Diastasis Recti |
| E | |
| ‘e’ | extended or enhanced |
| eLIRA | endoscopic Laparoscopic Intracorporeal Rectus Aponeuroplasty |
| eMILOS | endoscopic Mini- or Less Open Sublay repair |
| eTEP | extended/enhanced-view Totally ExtraPeritoneal |
| EAF | Entero Atmospheric Fistula |
| ECF | EnteroCutaneous Fistula |
| ECS | Endoscopic Component Separation |
| ELAR | Endoscopic Linea Alba Reconstruction |
| EO | External Oblique |
| ePTFE | extended PolyTetraFluoroEthylene |
| F | |
| FG | Fibrin Glue |
| G | |
| GPRVS | Giant Prosthetic Reinforcement of the Visceral Sac |
| GFN | Genito Femoral Nerve |
| H | |
| ‘h’ | Hybrid |
| HH | Hiatal Hernia |
| HWPP | Heavy Weight PolyPropylene |
| I | |
| IH | Incisional Hernia/Inguinal Hernia/IlioHypogastric nerve |
| IHN | Ilio Hypogastric Nerve |
| IIN | Ilio Inguinal Nerve |
| IO | Internal Oblique muscle |
| IPOM (+/plus) | IntraPeritoneal Onlay Mesh (hernia defect closure) |
| IRD | Inter Rectus Distance |
| J | |
| K | |
| L | |
| ‘l’ | laparoscopic |
| LFCN | Lateral Femoral Cutaneous Nerve |
| LIH | Lichtenstein Inguinal Hernia repair |
| LIRA | Laparoscopic Intracorporeal Rectus Aponeuroplasty |
| LOD | Loss Of Domain |
| LTA mesh | Long-Term Absorbable mesh |
| LVHR | Laparoscopic Ventral Hernia Repair |
| LWPP | LightWeight PolyPropylene |
| M | |
| MILA | Minimally Invasive Laparotomy Approach |
| MILOS | MIni- or Less Open Sublay repair |
| MINIM | Minimally Invasive Non-Intraperitoneal Mesh |
| MOMI | Mesh Out Mesh In |
| MPO | MyoPectineal Orifice |
| N | |
| NPWT | Negative Pressure Wound Therapy |
| NVBs | NeuroVascular Bundles |
| O | |
| ‘o’ | open |
| OAT | Open Abdomen Treatment |
| OPUPS | Open Peri Umbilical Perforator Sparing |
| P | |
| PCOM | Primary Closure with Onlay Mesh |
| PCS | Posterior Component Separation |
| PDS | PolyDioxanone Suture |
| PEH | ParaEsophageal Hernia |
| PEST | Prostatectomy Extraction Site Trocar hernia |
| PIPOM | Partial Intra-Peritoneal Onlay Mesh |
| PIPS | Pubic Inguinal Pain Syndrome |
| PO | POlyester |
| POChP | PostOperative Chronic Pain |
| POCIP | PostOperative Chronic Inguinal Pain |
| POUR | PostOperative Urinary Retention |
| PP | PolyPropylene |
| PPAWI | Post-Partum Abdominal Wall Insufficiency |
| PPHR | PrePeritoneal Hernia Repair |
| PPHR | Pauli Parastomal Hernia Repair |
| PPP | Pauli Parastomal Plasty/Progressive PneumoPeritoneum |
| PROM | Patient Reported Outcome Measures |
| PRS | Posterior Rectus Sheath |
| PTS | Progressive Tension Sutures |
| PVDF | PolyVinyliDene Fluoride |
| PUMP | Preperitoneal Umbilical hernia Mesh Plasty |
| PUPS | PeriUmbilical Perforator-Sparing component separation |
| Q | |
| R | |
| RALS | Robot-Assisted Laparoscopic Surgery |
| RA-LVHR | Robot-Assisted Laparoscopic Ventral Hernia Repair |
| RASD | Robotic Assisted Surgical Devices |
| REPA | Reparación Endoscopica PreApeurotica |
| R-IPT | Robotic IlioPubic Tract repair |
| RoboTAR | Robotic Transversus Abdominis Release |
| RoME | Robotic Mesh Excision/Explantation |
| RR | RetroRectus |
| RS | Rives-Stoppa |
| RS | Retention Sutures |
| rTAPP | robot-assisted TransAbdominal PrePeritoneal |
| rTAR | robot-assisted Transversus Abominis Release |
| rTARUP | robotic Trans-Abdominal Retromuscular Umbilical Prosthetic repair |
| rTMR | robotic Transabdominal Midline Reconstruction |
| S | |
| SBO | Small Bowel Obstruction |
| SBR | Small Bowel Resection |
| SC | Spermatic Cord/SubCutaneous |
| SCOLA | SubCutaneous Onlay Laparoscopic Approach |
| SIRRS | Single Incision RetroRectus Surgery |
| SMART | Stapled Mesh stomA Reinforcement Technique |
| SMAS | Subcutaneous MusculoAponeurotic System aka Scarpa's and Camper's fascia |
| SSE | Surgical Site Event |
| SSI | Surgical Site Infection |
| SSO | Surgical Site Occurrence |
| SSOPI | Surgical Site Occurrences requiring Procedural Interventions |
| STORM | Stapled Transabdominal Ostomy Reinforcement with Mesh |
| STORRM | Stapled Transabdominal Ostomy Reinforcement with (Retromuscular) Mesh |
| SUPERSEXI repair | SUpraPubic Endoscopic Repair with Synthetic EXtraperitoneal Implant repair |
| T | |
| TA | Transversus Abdominis muscle |
| TAMR | TransAbdominal Midline Reconstruction |
| TAP | Transversus Abdominis Plane |
| TAPE | TransAbdominal Partial Extraperitoneal |
| TAPP | TransAbdominal PrePeritoneal |
| TAR | Transversus Abdominis Release |
| TARM | TransAbdominal RetroMuscular repair |
| TARUP | TransAbdominal Retromuscular Umbilical Prosthetic repair |
| TASDRR | TransAbdominal Single Dock RetroRectus |
| TEP | Totally Extraperitoneal Prosthesis |
| TESLAR | Totally Endoscopic Supra-aponeurotic Linea Alba Reconstruction |
| TIPP | TransInguinal PrePeritoneal |
| TMR | Transabdominal Midline Reconstruction |
| TRAM | Transverse Rectus Abdominis Myocutaneous flap |
| TRUMP | Transabdominal RetroUMbilical Prosthesis |
| U | |
| V | |
| VAS | Visual Analogue Scale |
| vTEP | ventral Totally Extraperioneal Prosthesis |
| VH | Ventral Hernia |
| VHR | Ventral Hernia Repair |
| W | |
| WLS | Weight Loss Surgery |
| WWYD | What Would You Do |
| X | |
| Y | |
| Z | |
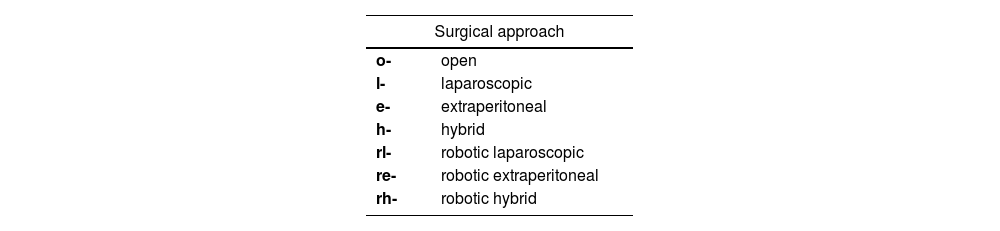
We propose to use a lowercase letter to indicate the approach used. This is regularly used to indicate a robotic approach (r-TAPP). We propose to use the same for other approaches. Open surgery is a repair performed via an open incision in the skin. Laparoscopic surgery is an endoscopic approach involving the creation of a pneumoperitoneum, which is often also named trans-abdominal approach (TAPP, TARUP, TARM). An extraperitoneal approach is an endoscopic approach where the goal is to avoid creating a pneumoperitoneum and to stay extraperitoneal to perform the repair (TEP, eTEP). A hybrid procedure is an endoscopic procedure with a planned open procedural step where a skin incision is made to perform part of the surgery via this incision. A hybrid approach is different from a conversion, where the surgery is moved from an endoscopic approach to an open approach because of an intraoperative change of plan caused by surgical difficulties or complications. All the endoscopic approaches can be performed using a robotic platform and are than called robot assisted endoscopic surgeries. A proposal for the lower-case letter(s) to be used for each approach is given in Table 2. We also propose the lowercase letter indicating the surgical approach to be followed by a hyphen to set it apart from the main abbreviations on hernia type, mesh type, mesh position and mesh fixation.
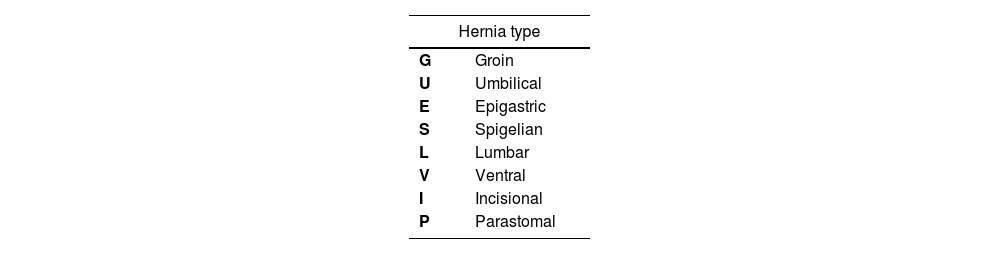
Hernia typeGroin hernia is a collection of lateral inguinal hernias, medial inguinal hernias, and femoral hernias. For the description of these group of cases we propose to use the letter G. Groin hernias are classified according to the European Hernia Society (EHS) classification in lateral (L), medial (M) and femoral (F) hernias, with the size of the hernia defect described as size 1, 2 or 3.1
Primary ventral hernias are described by the EHS as umbilical, epigastric, spigelian and lumbar hernias. We propose to use U, E, S and L.2 Secondary ventral hernias are mostly incisional hernias and we propose to use I. Some studies combine primary and secondary ventral hernias, for which we propose to use the letter V. Primary ventral hernias are classified by the EHS classification according to the type and the size of the hernia (small <2cm; medium 2–4cm; large >4cm). Incisional ventral hernias are classified by the EHS classification according to the location of the hernia (medial zones M1–M5; lateral zones L1–L4) and the width of the hernia (W1 <4cm; W2=4–10cm; W3 >10cm).
Parastomal hernias are classified according to the EHS classification according to the size and presence of a concomitant incisional hernia (Type I to Type IV) (Table 3).3
Mesh positionMeshes can be implanted in different layers of the abdominal wall during hernia repair. A consensus on mesh position terminology has been described recently and is proposed using the first letter of the abdominal wall plane. If no mesh was placed, we propose to use X. Four planes are described: Onlay (O), Retrorectus/Retromuscular (R), Preperitoneal (P) and Intraperitoneal (I) (Table 4).
Mesh typeFor hernia repair without the use of a mesh we propose the letter X. Meshes can be divided based on their origin (synthetic versus biological) and whether they are permanent or will absorb over time. Moreover, some combinations of partially absorbable meshes do exist. We propose the letters S and B for synthetic and biologic mesh respectively as an uppercase added by a lowercase p or a, to indicate permanent or absorbable meshes (Table 5).
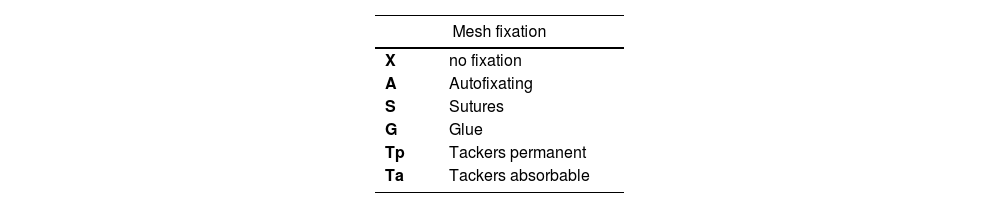
Mesh fixationMeshes can be either not fixed, fixed with sutures, fixed with glue or fixed with tackers. The tackers can be either permanent or absorbable (Table 6).
SummaryIn Table 7 we present an overview of the proposal and in Table 8 we list some examples of using the proposal for commonly used hernia repair techniques.
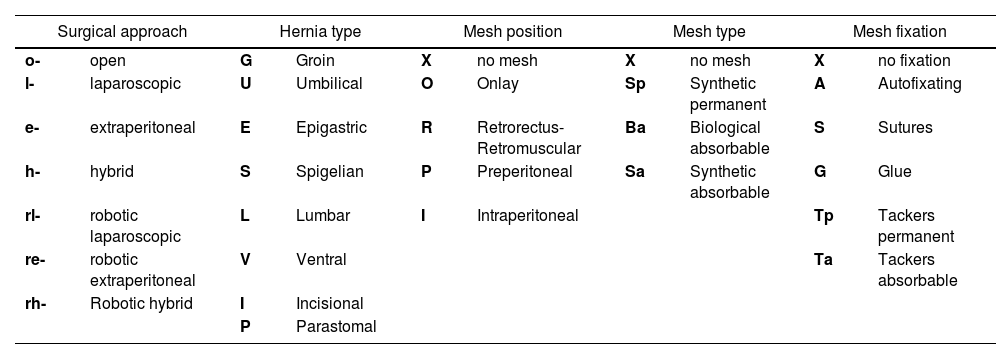
Overall proposal for rational use of abbreviations to describe hernia repair techniques.
| Surgical approach | Hernia type | Mesh position | Mesh type | Mesh fixation | |||||
|---|---|---|---|---|---|---|---|---|---|
| o- | open | G | Groin | X | no mesh | X | no mesh | X | no fixation |
| l- | laparoscopic | U | Umbilical | O | Onlay | Sp | Synthetic permanent | A | Autofixating |
| e- | extraperitoneal | E | Epigastric | R | Retrorectus-Retromuscular | Ba | Biological absorbable | S | Sutures |
| h- | hybrid | S | Spigelian | P | Preperitoneal | Sa | Synthetic absorbable | G | Glue |
| rl- | robotic laparoscopic | L | Lumbar | I | Intraperitoneal | Tp | Tackers permanent | ||
| re- | robotic extraperitoneal | V | Ventral | Ta | Tackers absorbable | ||||
| rh- | Robotic hybrid | I | Incisional | ||||||
| P | Parastomal | ||||||||
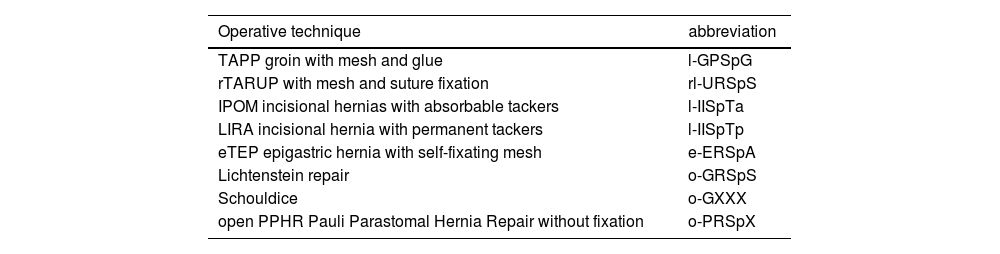
Examples of using the proposed rational use of abbreviations for commonly used acronyms of surgical hernia repair techniques.
| Operative technique | abbreviation |
|---|---|
| TAPP groin with mesh and glue | l-GPSpG |
| rTARUP with mesh and suture fixation | rl-URSpS |
| IPOM incisional hernias with absorbable tackers | l-IISpTa |
| LIRA incisional hernia with permanent tackers | l-IISpTp |
| eTEP epigastric hernia with self-fixating mesh | e-ERSpA |
| Lichtenstein repair | o-GRSpS |
| Schouldice | o-GXXX |
| open PPHR Pauli Parastomal Hernia Repair without fixation | o-PRSpX |
A plenitude of acronyms is currently used to describe surgical advances in hernia surgery. To overcome ambiguity in reporting scientific literature, we propose a more rational use of abbreviations to describe hernia repair techniques based on the type of access, the type of hernia, the mesh position, the type of mesh used, and the type of mesh fixation.
FundingNone declared.
Conflict of interestFM reports having received research grants from Medtronic, Intuitive Surgical and FEG Textiltechnik besides speakers’ honoraria from Medtronic, BD Bard, Intuitive Surgical and WL GORE, consultancy honoraria from Medtronic, CMR surgical and expert testimony from Sofradim. FM is proctor for Intuitive Surgical and participates in the Advisory Board of Medtronic.
MV reports participation in the Advisory Board of Medtronic.

