





FAST is essential to decide whether trauma patients need laparotomy, but it has a notable decrease in accuracy in patients with pelvic fracture.
Our objective is to analyze the consequences of therapeutic decision-making based on the FAST results in trauma patients with pelvic fracture.
MethodsDescriptive study that includes trauma patients older than 16 with a pelvic fracture admitted to the critical care area or who died. The FAST result was compared with a true positive or negative value according to the results of laparotomy or abdominal CT. We recorded diagnosis and treatment of each injury and resolution of the case, detailing the cause of death, among all variables.
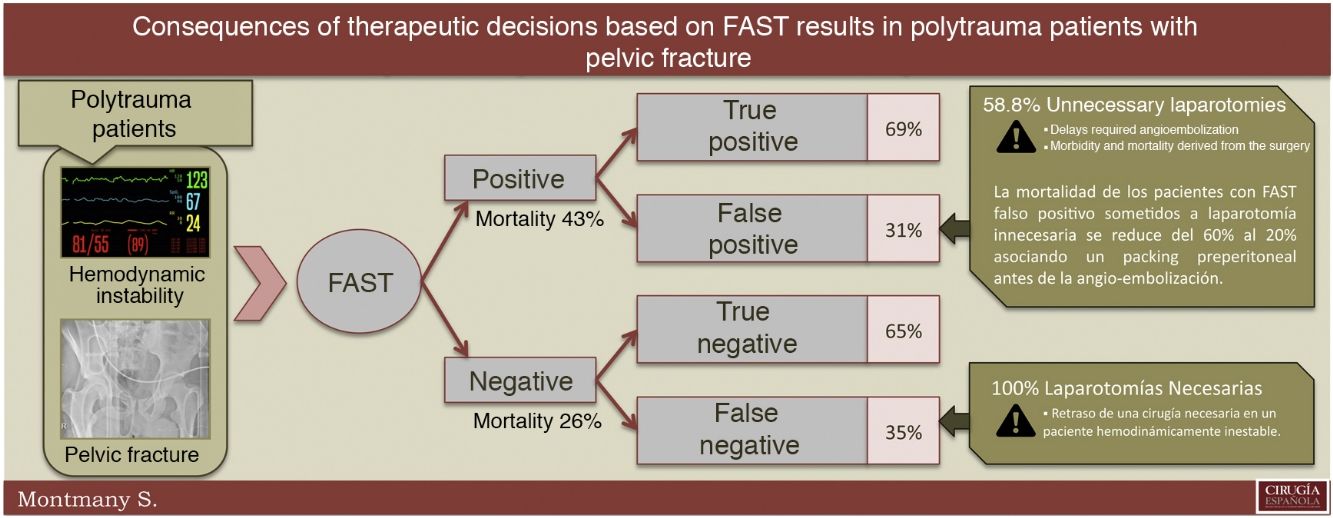
ResultsOver the 13-year period, we included 263 trauma patients with pelvic fracture, with a mean ISS of 31 and mortality of 19%. FAST had a sensitivity of 65.2%, specificity of 69%, false negative rate of 34.8% and false positive rate of 30.9%. Hemodynamically unstable patients died twice as many stable patients (27% vs 14%, P < .05). Patients with positive FAST died more than negative FAST (43% vs 26%); and 4 out of 10 hemodynamically unstable patients who underwent non-therapeutic laparotomy after presenting a false positive FAST died from hypovolemic shock. The mortality rate fell from 60% to 20% when preperitoneal packing was performed before angio-embolization of the pelvis.
ConclusionFAST has low accuracy in polytraumatized patients with pelvic fracture. Patients with false positive FAST have higher mortality, which can be reduced notably by applying preperitoneal packing.
La exactitud del FAST disminuye notablemente en los pacientes politraumáticos con fractura pélvica.
El objetivo es analizar las consecuencias de tomar decisiones terapéuticas basadas en el resultado del FAST en los pacientes politraumáticos con fractura de pelvis.
MétodosEstudio descriptivo de pacientes con politraumatismos mayores de 16 años que han ingresado en el área de críticos o que han fallecido previamente, con fractura pélvica. El resultado del FAST ha sido comparado con un valor realmente positivo o negativo según el resultado de la laparotomía o de la tomografía computarizada.
ResultadosEn 13 años, se ha incluido a 263 pacientes politraumáticos con fractura pélvica (ISS medio de 31; mortalidad 19%). El FAST tenía una sensibilidad del 65,2%, una especificidad del 69%, una tasa de falsos negativos del 34,8% y una tasa de falsos positivos del 30,9%. Los pacientes hemodinámicamente inestables tenían el doble de mortalidad que los pacientes estables (27% vs. 14%, p < 0,05). Los pacientes con un FAST positivo tenían mayor mortalidad que los pacientes con FAST negativo (43% vs. 26%); 4 de 10 pacientes hemodinámicamente inestables con un FAST falsamente positivo que se sometieron a laparotomía exploradora innecesaria murieron por shock hipovolémico. La mortalidad se redujo del 60 al 20% asociando un packing preperitoneal.
ConclusionesLa reducida eficacia del FAST en pacientes con fractura de pelvis nos obliga a cuestionarnos las consecuencias de la toma de decisiones terapéuticas con base en sus resultados. Los pacientes con FAST falsamente positivo tienen una mortalidad mayor, que se puede reducir aplicando un packing preperitoneal.
Polytrauma patients with pelvic fracture are high-energy trauma patients. These fractures are associated with a high risk of mortality that may even reach 45%, a mean injury severity score (ISS)1 of 50 and associated injuries in more than 90% of cases.2–4
Hemodynamically unstable polytrauma patients with pelvic fracture require rapid and effective initial evaluation that allows for appropriate treatment to be initiated as soon as possible to achieve the best results. Focused Abdominal Sonography for Trauma (FAST)5,6 is an essential non-invasive tool used for rapid evaluation of the abdomen in order to detect hemoperitoneum. According to well-standardized studies and protocols,7 the presence of hemoperitoneum is an indicator of intra-abdominal injury requiring immediate surgical intervention. Meanwhile, hemodynamically unstable patients with pelvic fracture and negative FAST require pelvic angioembolization or preperitoneal packing, depending on the therapeutic possibilities.7,8
FAST has a sensitivity >87% and a specificity >92% to detect the presence or absence of hemoperitoneum in polytrauma patients with hypovolemic shock.7,8 These values decrease significantly when the trauma involves pelvic fracture because the false positive and false negative rates increase considerably. In patients with pelvic fracture, the FAST achieves a sensitivity that ranges between 26% and 65%, and a specificity that ranges from 80% to 90%.9–13
The hypothesis of the study is that the low sensitivity and specificity of FAST in polytrauma patients with pelvic fracture leads to a greater number of unnecessary laparotomies and a delay in the angiographic treatment needed.
The main objective of our study is to assess the validity of FAST in polytrauma patients with a pelvic fracture and to analyze the clinical consequences of therapeutic decision-making based on its results.
MethodsWe present a retrospective, descriptive study of polytrauma patients with pelvic fracture over the age of 16 who were either admitted to the critical care unit or died.
The patients were prospectively registered in a protected Access® database from March 2006 until today. The following variables were collected for each case: age, sex, mechanism of action, ISS 8, Revised Trauma Score (RTS),14 prehospital and hospital vital signs, complementary tests performed, diagnosis and treatment of each injury, complications and resolution of the case, specifying the date and cause of death if the patient has died.
When FAST was used,5,6 two possible results have been reported: positive, when free fluid was observed in the abdominal cavity; or negative, when free fluid was not observed in the abdominal cavity. For the purpose of this study, we did not perform pericardial FAST.
A standard reference in surgical patients is the presence or absence of pathological findings. For our study, the presence of pathological findings was defined as a necessary laparotomy (hemoperitoneum >500 cc and injuries requiring surgical treatment). The absence of pathological findings was defined as an unnecessary laparotomy (no pathological findings, or minor injuries requiring no surgical treatment).
The standard reference study in non-operated patients was computed tomography (CT) scan. The presence of pathological findings was defined as CT findings requiring surgical treatment. The absence of pathological findings was defined as either a normal CT scan or pathological findings on CT that required nonsurgical treatment.
We compared the FAST results with the standard reference tests depending on whether the hemodynamically unstable patients (systolic blood pressure ≤90 or heart rate ≥100) underwent laparotomy.
Statistical analysisThe descriptive analysis was presented as mean and standard deviation for continuous variables and as percentages for categorical variables.
We calculated the sensitivity, specificity, positive predictive value and negative predictive value of the FAST. There were no missing data.15,16
We have followed the STARD17 method for reporting the results.
The Student’s t test and the chi-square test were used to compare groups after confirming the normality of the variables and the homoscedasticity of the variance. For the analysis of numerical variables that did not comply with the laws of normality, a non-parametric Mann–Whitney U test was used. IBM SPSS 21.0® was used for the different statistical calculations.
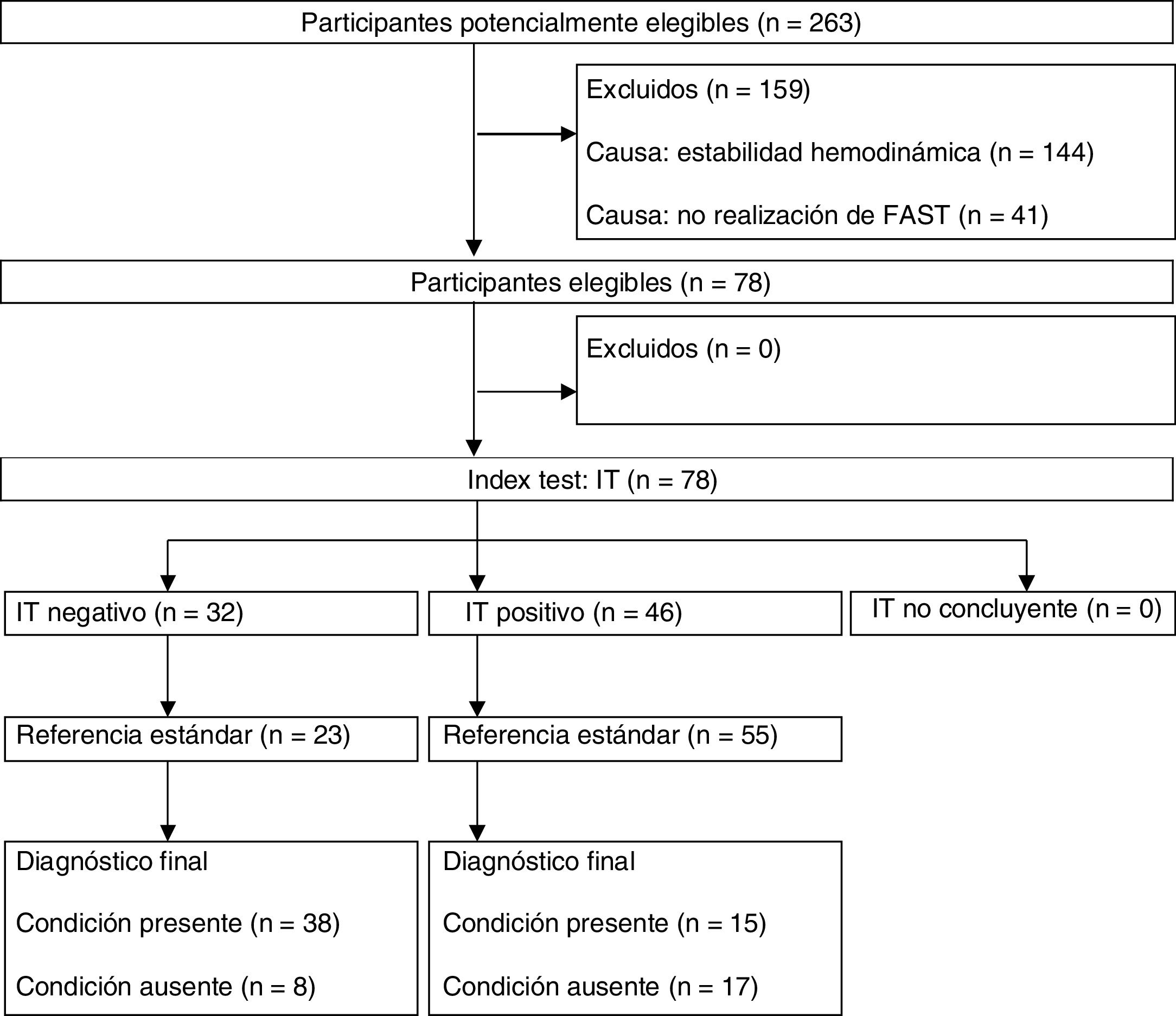
ResultsIn a 13-year period, from March 2006 to March 2019, we registered 1826 patients over the age of 16 with multiple injuries who were either admitted to the critical care unit or died, 14.4% of which (263 patients) presented pelvic fracture. Out of the 263 patients with pelvic fracture, 78 hemodynamically unstable patients studied by FAST were included in our study (see STARD diagram, Fig. 1).

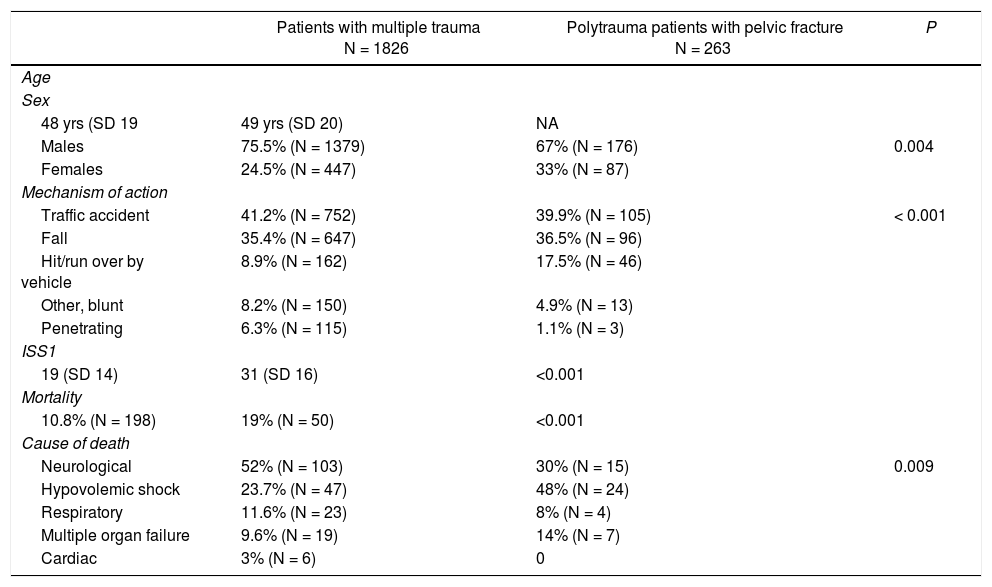
The mean age of the polytrauma patients with pelvic fracture was 49, and 67% of the patients were men. The mechanism of action was mainly blunt trauma (99%), and the most frequent causes were traffic accidents and falls (Table 1).
Demographic data.
| Patients with multiple trauma N = 1826 | Polytrauma patients with pelvic fracture N = 263 | P | |
|---|---|---|---|
| Age | |||
| Sex | |||
| 48 yrs (SD 19 | 49 yrs (SD 20) | NA | |
| Males | 75.5% (N = 1379) | 67% (N = 176) | 0.004 |
| Females | 24.5% (N = 447) | 33% (N = 87) | |
| Mechanism of action | |||
| Traffic accident | 41.2% (N = 752) | 39.9% (N = 105) | < 0.001 |
| Fall | 35.4% (N = 647) | 36.5% (N = 96) | |
| Hit/run over by vehicle | 8.9% (N = 162) | 17.5% (N = 46) | |
| Other, blunt | 8.2% (N = 150) | 4.9% (N = 13) | |
| Penetrating | 6.3% (N = 115) | 1.1% (N = 3) | |
| ISS1 | |||
| 19 (SD 14) | 31 (SD 16) | <0.001 | |
| Mortality | |||
| 10.8% (N = 198) | 19% (N = 50) | <0.001 | |
| Cause of death | |||
| Neurological | 52% (N = 103) | 30% (N = 15) | 0.009 |
| Hypovolemic shock | 23.7% (N = 47) | 48% (N = 24) | |
| Respiratory | 11.6% (N = 23) | 8% (N = 4) | |
| Multiple organ failure | 9.6% (N = 19) | 14% (N = 7) | |
| Cardiac | 3% (N = 6) | 0 | |
SD: standard deviation; ISS: Injury Severity Score.
The mean ISS 1 was 31 (SD 16), which was clearly higher than the mean ISS for patients with multiple injuries registered in our hospital (ISS 19, SD 14). Mortality was 19%, which was also higher than the mortality rate of the global series (10.8%). The main cause of death varied from neurological causes in the general group to hypovolemic shock when the patient presented pelvic fracture (Table 1).
Out of the 263 polytrauma patients with pelvic fracture, FAST was performed in 98 (37%): 39 positive, and 59 negative.
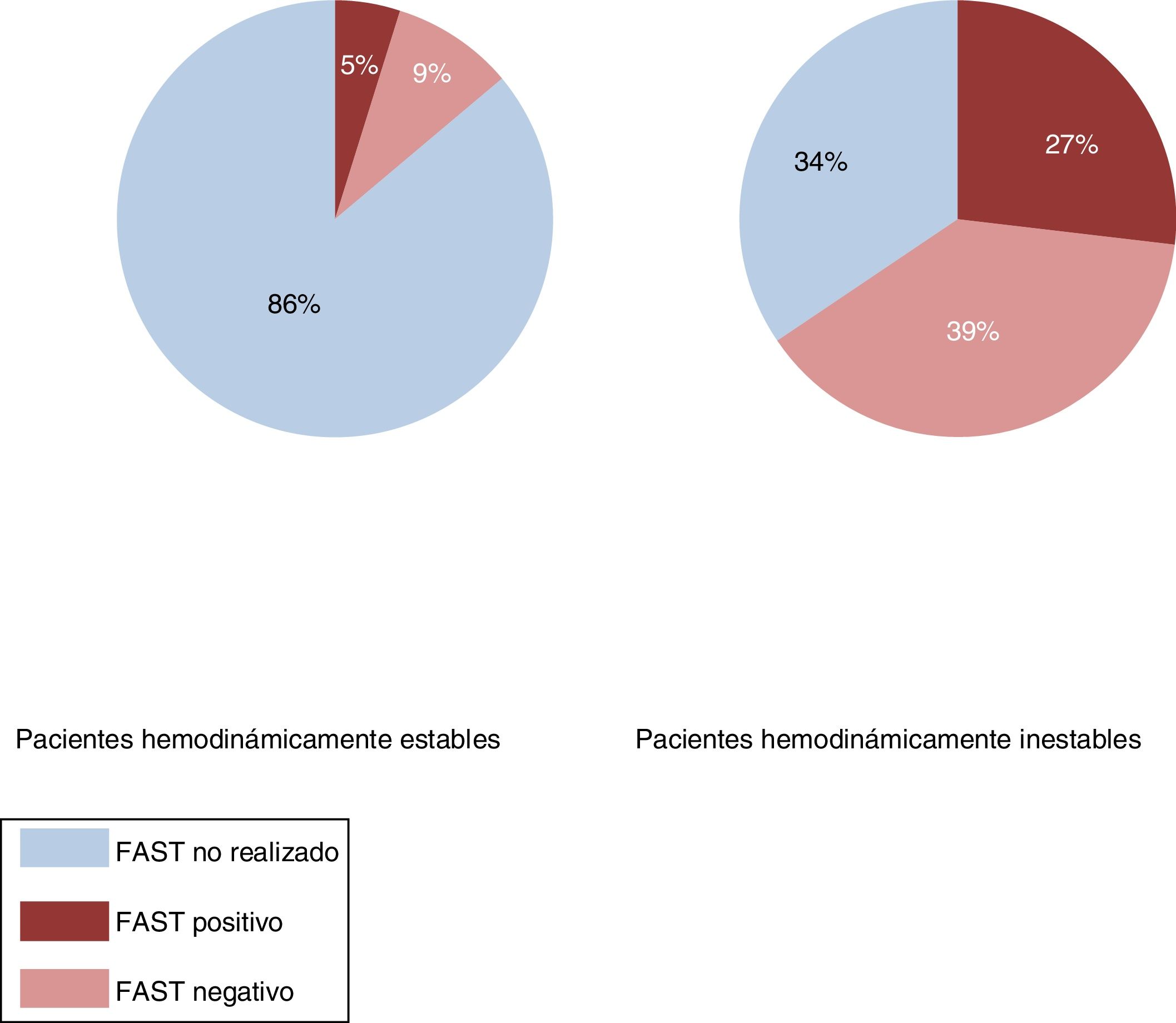
In our series, 144 patients were hemodynamically stable, and FAST was performed in 14% (20 patients), despite their stability. Out of the 119 hemodynamically unstable patients, the FAST score was analyzed in 66% (78), finding 46 patients with negative FAST (39%) and 32 with positive FAST (27%) (Fig. 2).

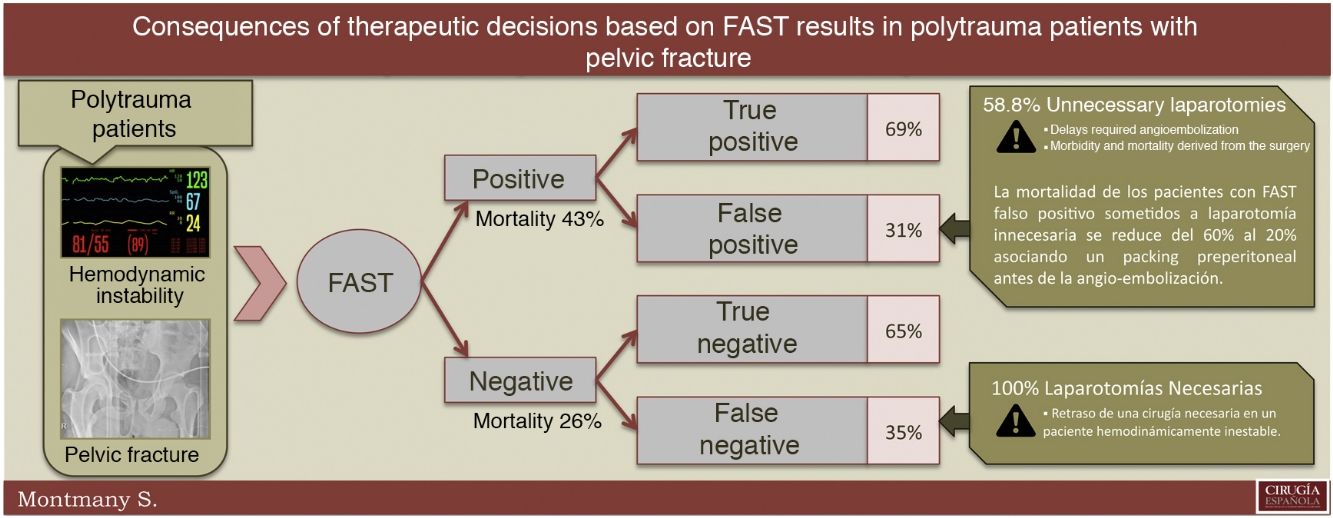
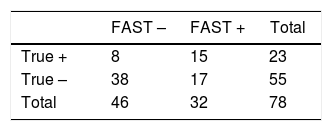
When we analyzed the FAST result versus the actual presence or absence of intra-abdominal bleeding (Table 2), we found a false negative rate of 34.8% and a false positive rate of 30.9%. In our series, the sensitivity of FAST was 65.2% (95% CI: 45.75 %–84.68 %), specificity 69% (95% CI: 56.88 %–81.30 %), positive predictive value 46.8% (95% CI: 29.58 %–64.17 %) and negative predictive value 82.6% (95% CI: 71.66 %–93.56 %). 100% of the FAST false negatives (8 patients) required surgical treatment that was delayed due to the performance of an abdominal CT scan in hemodynamically unstable patients. Meanwhile, 58.8% of the FAST false positives (10 patients) underwent an unnecessary laparotomy, causing a delay in the needed angiographic treatment of the pelvic fracture, with active arterial bleeding. We had temporarily stabilized the pelvis of all patients undergoing laparotomy by means of a strap (sheet, belt, or other device suitable for such use). In no case was surgical external fixation used at this point of treatment.
The analysis of the number of quadrants where free fluid was observed by FAST (hepatorenal fossa, splenorenal fossa and pelvis) found no differences between true positives and false positives. The mean number of quadrants with free fluid detected by FAST was 2 in the false positive cases and 2.13 in the true positives.
When we compared the mortality rate of the different groups of patients, we observed that hemodynamically unstable patients had almost twice the mortality compared to stable patients (27% vs 14%, P < .05). Hemodynamically unstable patients with a positive FAST died more frequently than patients with a negative FAST (43% vs 26%). Although the mortality rate in hemodynamically unstable patients was similar when the FAST was true positive or false positive (40% vs. 41%), 4 out of 10 hemodynamically unstable patients who had undergone unnecessary laparotomy due to a false-positive FAST died from hypovolemic shock secondary to pelvic bleeding. This mortality rate (60%) dropped to 20% when it was associated with preperitoneal packing before angioembolization of the pelvis (Table 3).
Differences in mortality.
| Total | Death | P | |
|---|---|---|---|
| Hemodynamically stable | 144 patients | 14% (N = 20) | 0.01 |
| Hemodynamically unstable | 119 patients | 27% (N = 30) |
| Total | Death | |
|---|---|---|
| Hemodynamically unstable with negative FAST | 46 patients | 26% (N = 12) |
| Hemodynamically unstable with positive FAST | 28 patients | 43% (N = 12) |
| Total | Death | |
|---|---|---|
| Hemodynamically unstable with TP FAST | 15 patients | 40% (N = 6) |
| Hemodynamically unstable with FP FAST | 17 patients | 41% (N = 7) |
| Total | Death | |
|---|---|---|
| Unnecessary laparotomy (FP) with preperitoneal packing | 5 patients | 20% (N = 1) |
| Unnecessary laparotomy (FP) without preperitoneal packing | 5 patients | 60% (N = 3) |
FP: false positive; TP: true positive.
It is already well known3,4,7 that polytrauma patients with pelvic fracture are a group of patients with greater injury severity (mean ISS 31 vs. 19, P < .05) and a higher percentage of mortality (19% vs 10.8%, P < .05) than patients with multiple trauma injuries in general. The management of hemorrhage is essential in polytrauma patients with pelvic fracture since 48% die due to hypovolemic shock.
In our study starting in 2006, abdominal FAST was used to rule out bleeding in 65% of cases. Some 34% of hemodynamically unstable patients endured the risk of transfer for abdominal CT scan without previously ruling out intra-abdominal bleeding using FAST. This coincides with the results published in a multicenter study in Catalonia, where 27%–33% of hemodynamically unstable patients were studied with abdominal CT scan. This percentage did not decrease even after specific training information sessions and the placement of posters in the trauma rooms at different hospitals that provided treatment recommendations for patients with multiple trauma injuries.18
Although the precision of FAST depends on the user, its sensitivity in hemodynamically unstable patients with multiple trauma injuries ranges between 80% and 97%5–8 and has an extraordinary specificity between 95% and 99.5%.5–8 When hemodynamically unstable polytrauma patients have fractured pelvis, there is a significant percentage of false positives and false negatives due to interference from the retroperitoneal hematoma associated with the pelvic fracture. The high rate of false positives and false negatives reduces its sensitivity to values between 26% and 65%, and its specificity to between 80% and 90%,9–13 despite the FAST being performed by examiners with the same experience that achieved a sensitivity and specificity >80%–90% when there is no pelvic fracture. In our hospital, we have identified this significant reduction with a sensitivity of 65.2% and a specificity of 69%, even though the FAST is routinely conducted by radiologists with extensive experience in ultrasound.
In general, 200 mL of blood is needed to be able to visualize free fluid using FAST.13 It is scientifically proven that any amount of free fluid observed by FAST is an indication for laparotomy in hemodynamically unstable patients.5,6,10 The 4 spaces where the presence or absence of free fluid is classically studied with FAST are: cardiac, right flank (hepatic/renal), left flank (splenic/renal), and pelvis (bladder/rectal or uterine).6 In our study, we analyzed whether the number of spaces where free fluid was observed by FAST was associated with a higher rate of false positives versus the rate of true positives. No significant relationship was observed: false positives were found with liquid in 3 quadrants, and very positive values were found with liquid in a single quadrant.
As expected, hemodynamically unstable patients die at nearly twice the rate of hemodynamically stable patients (27% vs 14%, P < .05). More than half of polytrauma patients with pelvic fracture die due to hypovolemic shock (Table 1), and more unstable patients with positive FAST die (43% vs 26%), which is probably associated with having least 2 sources of bleeding instead of one: the pelvis and the abdomen. Although mortality in hemodynamically unstable patients is similar when the FAST is true positive or false positive (40% vs 41%), when we performed an unnecessary laparotomy for a false positive FAST and associated preperitoneal packing before transferring the patient to the relevant destination (angioembolization, Intensive Care Unit, etc.), mortality decreased from 60% to 20%. In these patients, where different and clinically relevant mortality percentages have been found, it has not been possible to analyze their statistical value as the requirements necessary for the chi-square test were not met.
The limitation of the current study is the number of cases registered and included in the study, which provides clinically very relevant results, but the statistical significance would improve with a larger sample size. The results can be extrapolated to any population of polytrauma patients with pelvic fracture and hemodynamic instability who undergo FAST.
It is not easy to find the origin of bleeding in patients with hypovolemic shock and a fractured pelvis. The influence of the mechanism of action on the origin of the bleeding has been described, and more than 80% of patients with pelvic fracture due to a fall bleed from the pelvis itself, while patients with a pelvic fracture caused by a crash-type mechanism may bleed from either the pelvis or abdomen.19
The lower efficacy of FAST in patients with pelvic fracture forces us to question the consequences of making therapeutic decisions based on its results. Patients with a false positive FAST have higher mortality rates, and we must consider making changes in the treatment of these patients to lower these rates.
In addition to the mechanism of injury, we should develop strategies to reduce the rate of false negatives and, especially, false positives in order to optimize appropriate treatment and reduce the mortality rate in hemodynamically unstable patients with polytrauma and pelvic fracture. For this, FAST can be repeated 15−20 min later to compare both results. With this maneuver, the Christian et al. group20 has reduced the rate of false negatives to 2%, but they have found no differences in the rate of false positives.
When faced with a positive FAST, Ruchholtz et al.21 always recommend laparotomy because they consider the risk of not performing a necessary laparotomy to be worse than performing unnecessary laparotomies. In our study, although mortality in hemodynamically unstable patients was similar when the FAST was true positive or false positive (40% vs 41%), 4 out of 10 hemodynamically unstable patients underwent unnecessary laparotomies for a false positive FAST and died from hypovolemic shock. This mortality rate (60%) was reduced to 20% when it was associated with preperitoneal packing before moving the patient for angioembolization of the pelvis. Another possibility to reduce mortality when given a positive FAST would be to compare the FAST result with a more invasive but more effective test, such as a diagnostic peritoneal aspiration, especially in patients who have suffered a crash-type mechanism of action, with the intention of reducing the number of unnecessary laparotomies.
FundingThe article has received no funding, either public or private.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Montmany Vioque S, Rebasa Cladera P. Campos Serra A, Gràcia Roman R, Luna Aufroy A, Navarro Soto S. Consecuencias de la toma de decisiones terapéuticas con base en el resultado del FAST en pacientes politraumáticos con fractura pélvica. Cir Esp. 2021;99:433–439.
