




Appendiceal intussusception is a rare pathology. It represents only 0.01% of indications for apendicectomy1 and is a diagnostic challenge.2
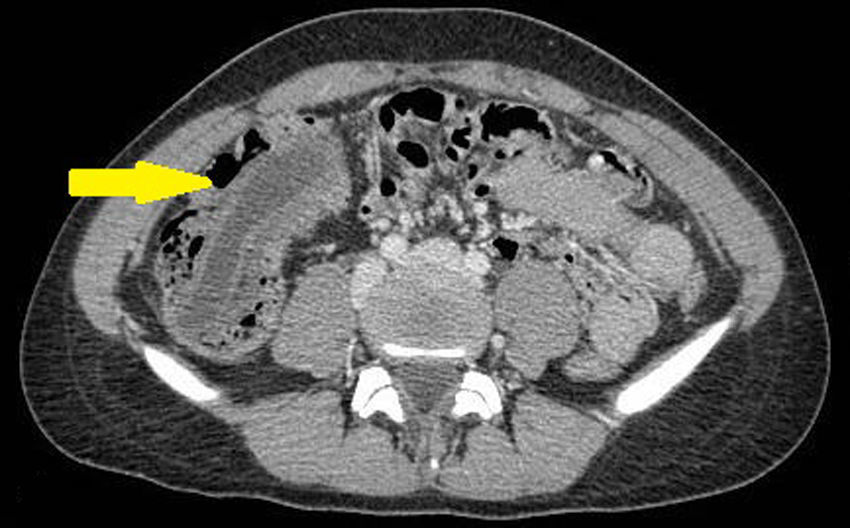
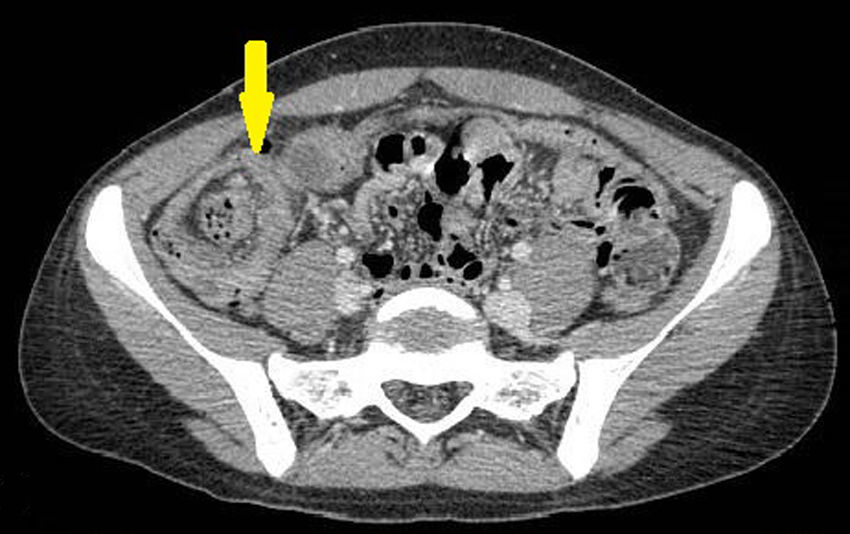
We present the case of a 20-year-old female patient who came to the Emergency Room with colicky abdominal pain in the right iliac fossa that had lasted for several days, with no other associated symptoms. Blood work-up showed no alterations. Due to the persistence of the pain, imaging tests were indicated. Ultrasound revealed an image in the right iliac fossa. A CT scan showed a tubular structure with hypodense content at the hepatic angle that ended in a cecal sac (Fig. 1), as well as the invagination of the terminal ileum and the ileocecal valve in the right colon (Fig. 2). The findings were compatible with the diagnosis of invagination of an appendiceal mucocele, therefore urgent laparoscopic ileocecectomy was performed. The postoperative evolution was favorable, and the patient was discharged from hospital on the third postoperative day. The pathology study reported an appendiceal mucocele with no malignant histological features whose base protruded into the lumen of the cecum, causing intussusception.


Appendiceal intussusception is defined as the invagination of a portion of the appendix into its own lumen or that of the cecum. It is secondary to abnormal peristaltic movements caused by inflammation of the appendix and favored by lax mesoappendices with a broad appendicular lumen or by very mobile and thin appendices.3 This pathology appears more frequently in adults (76%) than in children, and in women than in men, with a 2:1 ratio. The most frequent age at onset is the fourth decade of life.2 In pediatric patients, the most frequent cause is inflammation of the appendix, while in adults the most common etiology is endometriosis (33%) followed by appendiceal mucocele (19%) and appendiceal inflammation (19%). In the remaining cases, the etiology is tumorous and there have been descriptions of carcinoid tumors, metastasis, hamartomas or lymphomas.2,4,5
The clinical manifestations are quite varied, ranging from acute pain in the right iliac fossa simulating acute appendicitis to intermittent chronic symptoms, such as pain, vomiting or rectal bleeding, to symptom-free cases.2–4 In 1941, McSwain established an anatomical classification with the different degrees of appendiceal intussusception6:
- -
Type I: tip of the appendix invaginates into the proximal lumen.
- -
Type II: the invagination starts at some point along the appendix, invaginating with the adjacent appendiceal tissue.
- -
Type III: the invagination starts at the junction of the cecum with the appendix.
- -
Type IV: retrograde intussusception of the appendix, where the proximal appendix invaginates into the distal appendix.
- -
Type V: complete intussusception of the appendix within the cecum due to progression of types I, II or III.
Ultrasound plays an important role in pediatric patients, while in adults CT is the test of choice,2 which identifies a bulls-eye image associated with a well-encapsulated cystic mass in the cecum.3 Colonoscopy provides information by identifying a vegetative image in the lumen of the cecum and allows for the differential diagnosis with primary tumors.3 Surgical treatment varies from appendectomy to right hemicolectomy depending on the etiology and the degree of intussusception.2–4,7 When the cause of the intussusception is an appendiceal mucocele, it is not recommended to reduce the intussusception due to the high risk of exposing the peritoneal cavity to mucin-producing cells.3,7
It is important for the follow-up of these to include colonoscopies, as up to 20% of benign appendiceal cystadenomas are associated with colorectal cancer.7,8
Please cite this article as: Sagarra Cebolla E, Burgos de la Obra Ferrari E, Velasco Sánchez EA, Gómez Lanz L. Intususcepción ileocólica por mucocele apendicular. Cir Esp. 2018;96:244–245.
