




We have read with great interest the recent and interesting contribution by Dr. Francia et al. about a case of late cardiac tamponade due to myocardial contusion.1 We would like to make certain observations regarding a similar case that we have recently treated.
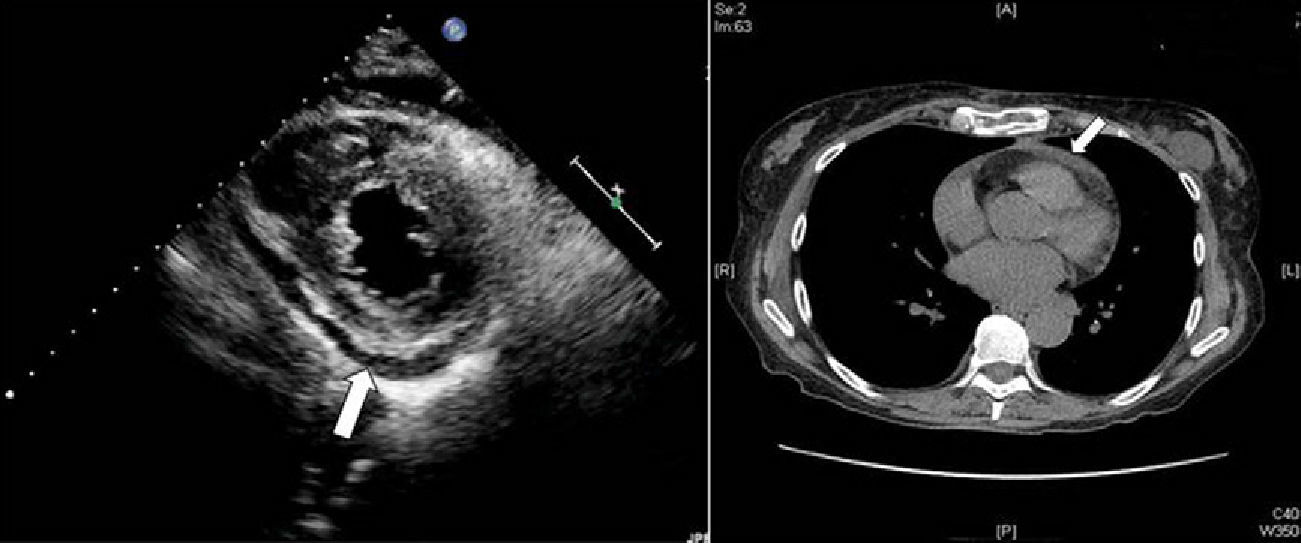
A 70-year-old woman came to our emergency department after having undergone the Heimlich maneuver because of choking. Upon admittance, the patient was conscious, oriented, with stable respiratory function and hemodynamics. She only presented mild pain on palpation in the lower sternal region, with no associated signs or symptoms. Three hours after hospitalization, ECG and myocardial enzymes presented no alterations (troponin I: 0.20ng/ml). Chest X-ray showed a simple sternal fracture in the distal third of the sternum. The patient remained under observation, and after 8h her enzymes began to rise progressively (troponin I: 0.62), although the ECG was normal. After 24h, high enzyme levels peaked (troponin I: 0.92) and there was evidence of inverted T-waves in leads V1–V3 on the ECG. Echocardiogram showed mild pericardial effusion and hypokinesis of the medial and apical anteroseptal segments with maintained EF (Fig. 1A). Chest CT demonstrated the sternal fracture and the aforementioned pericardial effusion (Fig. 1B), with no other findings. With the diagnosis of myocardial contusion, the patient was admitted to the cardiology ward for 12 days. She evolved favorably, with no progression of the pericardial effusion, although electrocardiographically she presented more T-wave inversion in the anterior wall and minimal elevation of ST in I and aVL. Coronary catheterization showed normal coronary branches.
 Echocardiogram 2D; parasternal short-axis plane: posterior pericardial effusion (arrow). (B) Thoracic CT: evidence of sternal fracture, as well as mild pericardial effusion (arrow).")
As for the initial description of the case by Dr. Francia, we would like to point out that any sternal trauma of less than 24h, even though apparently trivial, can entail serious complications. Thus, in cases of recent sternal trauma, it is advisable to maintain the patient under observation for at least 24h in order to rule out any possible myocardial contusion and resulting complications.2 This measure would be recommendable even in asymptomatic patients because, as it has been demonstrated both in the case described by the authors as well as in ours, the initial absence of noticeable symptoms and signs does not rule out the possibility that serious complications may present. During the observation period, we would emphasize the need for electrocardiography and myocardial enzyme monitoring3 in order to quickly detect possible myocardial injuries. Lastly, we should underline the association between myocardial contusion and pericardial effusion, as seen in both cases described. We coincide with the authors in considering that echocardiogram is fundamental when there is a suspicion of these entities.
Please cite this article as: Fariña Ruiz AP,et al. Contusión miocárdica y derrame pericárdico tras traumatismo esternal cerrado asintomático. Cir Esp. 2013;91:205-6.
