





Eccrine porocarcinoma is a rare cutaneous neoplasm that arises from the intraepidermal portion of the eccrine sweat glands.1 Its incidence varies between 0.005 and 0.01% of all skin tumors, and it is more common in women over 60 years of age,2,3 although cases have been reported in children and young adults.4
While the etiology of this neoplasm is unknown, it has been related to chronic sun exposure, exposure to chemical agents, and immunosuppression.1
The presentation is usually as a verrucous mass or nodule that can ulcerate. It is more frequent in the lower extremities (33.9%) and in the head and neck (39.9%).1 To date, few cases of porocarcinomas in the breast have been published in the literature.1,5,6
The rates of recurrence and locoregional metastatic extension are high, with multiple nodules in the area of the lesion.2 Distant metastatic extension (31%) usually has a fatal prognosis and develops mainly in lymph nodes (57.7%) and the lungs (12.8%).
The treatment of choice for this type of tumor is surgical resection of the lesion plus locoregional radiotherapy.1
Despite complete removal of the lesion, recurrence rates are around 20%, distant metastases are found in 12% of patients, and mortality rates are above 50%.3
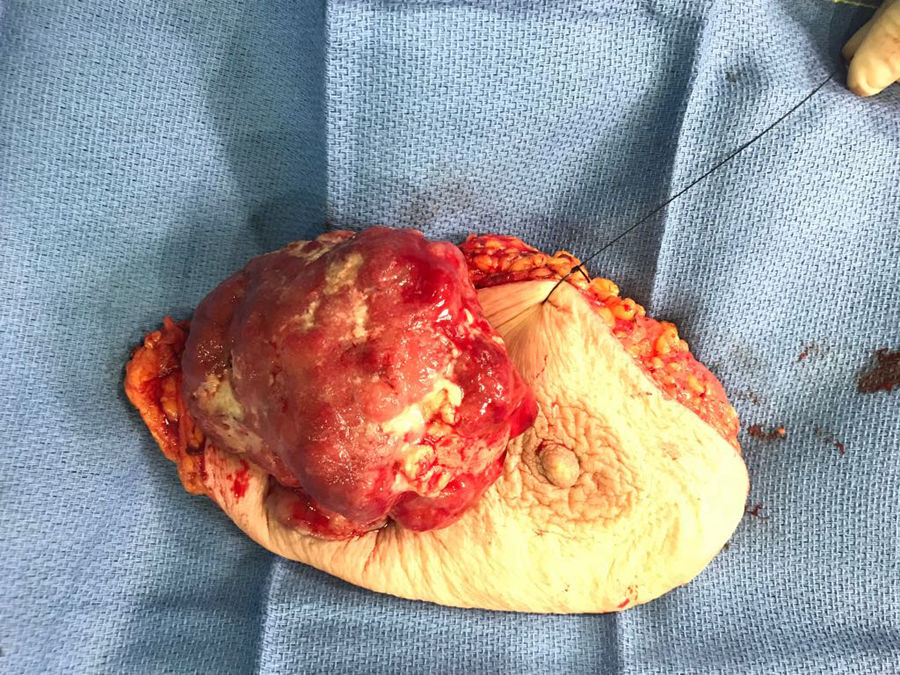
We present the case of a 92-year-old woman with a history of arterial hypertension, dyslipidemia, polyarthritis and vitamin D deficiency, who came to the emergency department after having suffered traumatic brain injury in the context of a constitutional syndrome with weight loss over several previous months. During physical examination, an indurated, ulcerated, exophytic mass measuring about 5 × 6 cm was observed on the right breast, with no signs of infection, but capillary bleeding when touched (Figs. 1 and 2). The patient reported progressive growth of the lesion over the last 2 years, but had not reported it to her physician.


Lab work detected a hemoglobin level of 8.4 g/dL.
With the suspicion of a mammary neoplasm, and due to the capillary bleeding, we decided to treat the patient surgically with a simple right mastectomy, which was performed without incident. The patient presented good postoperative progress and was discharged 7 days after the intervention.
After the pathology report provided the diagnosis of porocarcinoma, an extension study was ordered, which identified multiple axillary lymphadenopathy clusters on the right side. Given her age, the patient decided not to undergo adjuvant treatment.
Porocarcinoma located in the breast is a very rare entity in the literature. In this case, it was treated surgically, which is the treatment of choice. Although there are no established protocols due to its poor response, in the event of locoregional or distant metastases, treatment can be completed with lymph node resection, radiotherapy and chemotherapy. Our patient herself rejected the treatment due to her advanced age.
In this case, the differential diagnosis included breast carcinoma, and a biopsy would usually have been necessary prior to treatment. However, given that the mastectomy was palliative in this patient, the biopsy would not have changed the therapeutic decision. Early diagnosis is of vital importance in this type of tumors, given their high rates of recurrence and distant disease.
FundingNone.
Conflict of interestsNone.
Please cite this article as: Correa Bonito A, de la Hoz Rodríguez Á, Marín Campos C, Doblado Cardellach B, Martín Pérez E. Porocarcinoma de localización mamaria, a propósito de un caso. Cir Esp. 2020. https://doi.org/10.1016/j.ciresp.2019.12.007
