





To assess knowledge on the abdominal wall closure through a surgeon cohort survey.
MethodsA twenty question individual questionnaire on laparotomy in elective surgery.
ResultsA total of 131 surgeons from seven hospitals responded (72% specialists and 28% in training). 71% of respondents estimated the frequency of incisional hernia to be higher than 15% and 54% considered the technique to be the most significant risk factor. 85% considered midline laparotomy closed with slow absorbable suture (57%) in a single layer (66%) to be the most appropriate technique. 67% believed retention sutures to be the appropriate prevention technique. 50% did not know or could not apply the 4:1 technique. 87% considered that an incisional hernia can be prevented and that the technique is the most important factor on which to act. 84% believed that a prosthesis can prevent the occurrence of incisional hernia, whereas 40% of respondents never use it and only 38% use it in patients at risk. On comparing surveys between specialists and residents, significant differences appeared in terms of a better understanding of the theoretical technical aspects in trainee surgeons.
ConclusionsAlthough the results show an adequate understanding of the epidemiology and risk factors for development of incisional hernia, training and consensus measures are likely to be introduced in some basic technical aspects in order to improve results in laparotomy closure.
Evaluar los conocimientos sobre el cierre de la pared abdominal mediante una encuesta a una cohorte de cirujanos.
MétodosCuestionario individual de 20 preguntas sobre laparotomía en contexto de cirugía electiva.
ResultadosRespondieron 131 cirujanos de 7 hospitales (72% especialistas y 28% en formación). El 71% de los encuestados estimó la frecuencia de hernia incisional superior al 15% y un 54% consideró la técnica como factor de riesgo más importante. El 85% consideró la laparotomía media cerrada con sutura de absorción lenta (57%) en un solo plano (66%) como la técnica más adecuada. Un 67% estimó adecuados los puntos totales para la prevención. Un 50% desconocía o no sabía aplicar la técnica 4:1. El 87% consideró que una hernia incisional se puede prevenir y que la técnica es el factor más importante sobre el que se debe actuar. El 84% cree que una prótesis puede prevenir la aparición de una hernia incisional, en cambio un 40% de los encuestados no la usa nunca y solo un 38% la usan en pacientes de riesgo. Al comparar las encuestas entre especialistas y residentes, se detectaron diferencias significativas en cuanto a un mejor conocimiento de los aspectos técnicos teóricos en los cirujanos en formación.
ConclusionesAunque los resultados muestran un adecuado conocimiento de la epidemiología y factores de riesgo para desarrollo de hernia incisional, algunos aspectos técnicos básicos son susceptibles de introducción de medidas de formación y consenso para obtener mejores resultados en el cierre de laparotomía.
Abdominal wall closure is a basic technique that any surgeon should be capable of performing with the utmost safety and effectiveness. However, there is a 9%–20% incidence of problems resulting from abdominal wall closure complications, particularly incisional hernias, depending on the study reported.1–3
In general, no control mechanisms are in place for the correct completion of abdominal wall closure. It is frequently performed by trainee surgeons who often lack sufficient supervision or by a surgical team tired after long operations, or without applying prophylactic measures due to a lack of consensus and scientific evidence in this area.
To improve results, three types of action should be considered:
- -
Research into the relevance of the problem.
- -
Improve theoretical knowledge and technical skills.
- -
Reach a consensus and implement prophylactic measures in selected patients.
In our opinion, knowing how to close the abdominal wall and being aware of the consequences may help to improve technique and establish control measures on its effectiveness and results. Given the context described above, we used a survey on a cohort of surgeons in our country to assess their knowledge on abdominal wall closure, the frequency of incisional hernias and evisceration and preventive measures.
MethodsWe used a 20 question, individual questionnaire on laparotomy in elective surgery, given to a cohort of surgeons in Catalonia.
The sample included seven hospitals (three university hospitals and four regional ones) including a total of 104 specialists and 43 trainee surgeons. The surgeons had been contacted beforehand and had agreed to participate in the survey. The questionnaire was distributed (Appendix 1) among fully qualified surgeons and surgical residents of all years of training, during clinical sessions in the relevant departments. Any questionnaires which included mistakes that would hamper the recording of data were excluded from analysis. The survey data was collected anonymously (category and area of specialization), demographic data was not recorded, and specific questions were asked on laparotomy closures, using closed multiple choice responses and covering three sections:
- 1.
Basic technical issues.
- 2.
Knowledge of epidemiology and risk factors involved in the appearance of complications.
- 3.
Systems used to prevent the appearance of incisional hernias and evisceration.
Statistical analysis was performed with the SPSS 20.0 programme (IBM Inc., Rochester, MN, USA) and the findings between the most experienced surgeons and those in training were compared. The association between qualitative variables was analyzed using contingency tables (chi-square and Exact Fisher test when relevant). The data was presented in absolute numbers and percentages. Statistical significance was established at P<.05.
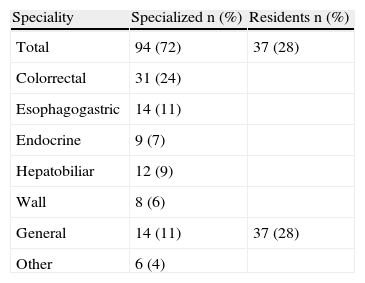
ResultsSeven hospitals in Catalonia with a total staff of 147 surgeons (104 specialists and 43 residents) participated. 140 questionnaires (95% participation) were collected, nine of which were excluded due to incomplete or insufficient data which would have impeded response analysis. Of the 131 (89%) valid questionnaires, 72% (94/104) were completed by specialists and 28% (37/43) by trainee surgeons. The cohort characteristics are shown in Table 1.
The analysis of responses with regard to epidemiology and risk factors associated with abdominal wall closure complications are shown in Table 2.
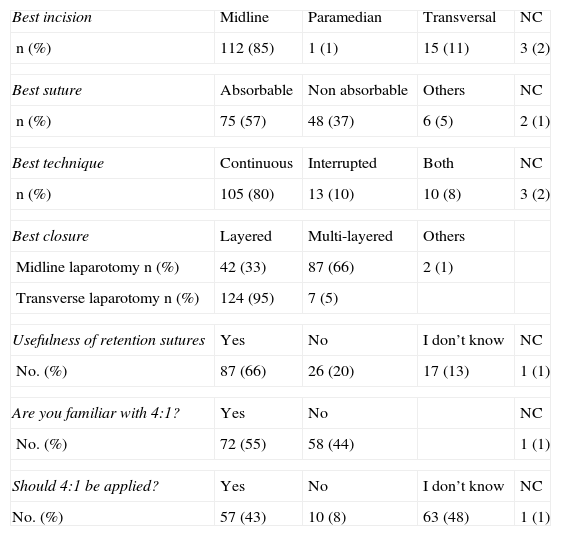
With regard to technique (Table 3), 85% considered midline laparotomy as the most appropriate incision, to be closed with slow absorbable monofilament suture (57%) in a single layer (66%), although 33% of respondents were in favour of closure in 2 layers. 66% considered retention sutures appropriate as a technique to prevent incisional hernias and evisceration. 44% were unfamiliar with, and 48% did not know how to apply the 4:1 technique.
Technical Aspects.
| Best incision | Midline | Paramedian | Transversal | NC |
| n (%) | 112 (85) | 1 (1) | 15 (11) | 3 (2) |
| Best suture | Absorbable | Non absorbable | Others | NC |
| n (%) | 75 (57) | 48 (37) | 6 (5) | 2 (1) |
| Best technique | Continuous | Interrupted | Both | NC |
| n (%) | 105 (80) | 13 (10) | 10 (8) | 3 (2) |
| Best closure | Layered | Multi-layered | Others | |
| Midline laparotomy n (%) | 42 (33) | 87 (66) | 2 (1) | |
| Transverse laparotomy n (%) | 124 (95) | 7 (5) | ||
| Usefulness of retention sutures | Yes | No | I don’t know | NC |
| No. (%) | 87 (66) | 26 (20) | 17 (13) | 1 (1) |
| Are you familiar with 4:1? | Yes | No | NC | |
| No. (%) | 72 (55) | 58 (44) | 1 (1) | |
| Should 4:1 be applied? | Yes | No | I don’t know | NC |
| No. (%) | 57 (43) | 10 (8) | 63 (48) | 1 (1) |
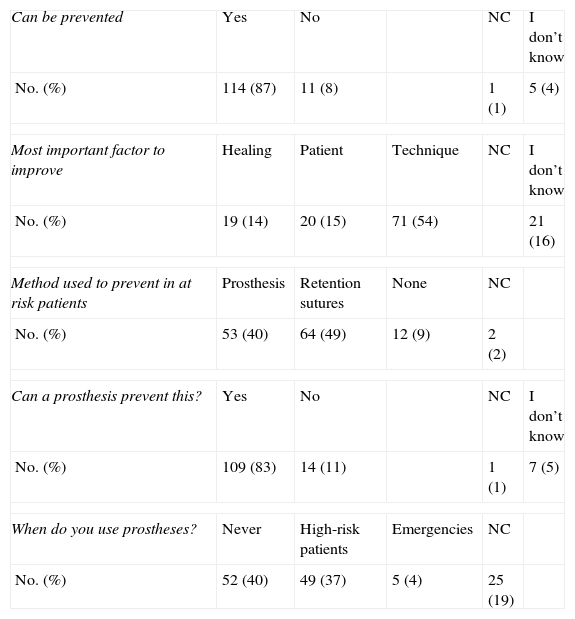
87% considered that an incisional hernia could be prevented and 54% considered that technique is the most important factor on which improvements can be made. 83% believed a prosthesis could be used as prophylaxis against the appearance of an incisional hernia, however, 40% of respondents never use it and only 37% use it in at risk patents, whilst 49% use retention sutures in these patients (Table 4).
Prevention.
| Can be prevented | Yes | No | NC | I don’t know | |
| No. (%) | 114 (87) | 11 (8) | 1 (1) | 5 (4) | |
| Most important factor to improve | Healing | Patient | Technique | NC | I don’t know |
| No. (%) | 19 (14) | 20 (15) | 71 (54) | 21 (16) | |
| Method used to prevent in at risk patients | Prosthesis | Retention sutures | None | NC | |
| No. (%) | 53 (40) | 64 (49) | 12 (9) | 2 (2) | |
| Can a prosthesis prevent this? | Yes | No | NC | I don’t know | |
| No. (%) | 109 (83) | 14 (11) | 1 (1) | 7 (5) | |
| When do you use prostheses? | Never | High-risk patients | Emergencies | NC | |
| No. (%) | 52 (40) | 49 (37) | 5 (4) | 25 (19) | |
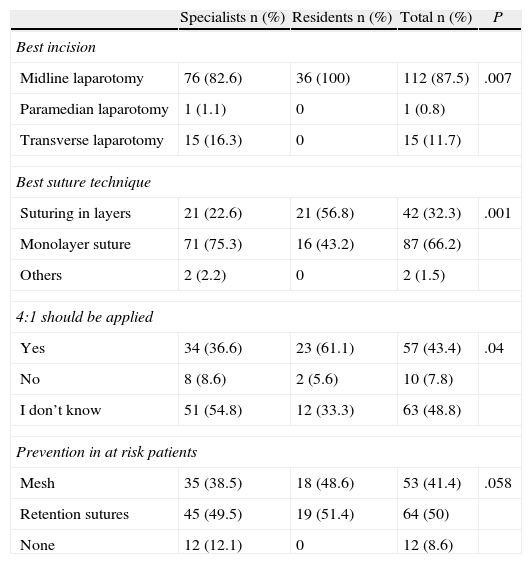
When comparing results between specialists and residents, significant differences were detected regarding awareness of the theoretical technical aspects. A higher percentage of residents were aware of the 4:1 (P=.04) rule; all residents agreed that midline laparotomy is the best line of approach (P=.007); and the majority of specialist surgeons agreed that the best technique for closure is a continuous suture (P=.001). No significant differences were detected with regard to prophylactic measures to be applied for at risk patients (Table 5).
Comparison Responses Between Specialists and Residents (Blank Responses Excluded).
| Specialists n (%) | Residents n (%) | Total n (%) | P | |
| Best incision | ||||
| Midline laparotomy | 76 (82.6) | 36 (100) | 112 (87.5) | .007 |
| Paramedian laparotomy | 1 (1.1) | 0 | 1 (0.8) | |
| Transverse laparotomy | 15 (16.3) | 0 | 15 (11.7) | |
| Best suture technique | ||||
| Suturing in layers | 21 (22.6) | 21 (56.8) | 42 (32.3) | .001 |
| Monolayer suture | 71 (75.3) | 16 (43.2) | 87 (66.2) | |
| Others | 2 (2.2) | 0 | 2 (1.5) | |
| 4:1 should be applied | ||||
| Yes | 34 (36.6) | 23 (61.1) | 57 (43.4) | .04 |
| No | 8 (8.6) | 2 (5.6) | 10 (7.8) | |
| I don’t know | 51 (54.8) | 12 (33.3) | 63 (48.8) | |
| Prevention in at risk patients | ||||
| Mesh | 35 (38.5) | 18 (48.6) | 53 (41.4) | .058 |
| Retention sutures | 45 (49.5) | 19 (51.4) | 64 (50) | |
| None | 12 (12.1) | 0 | 12 (8.6) | |
The data collected through our survey revealed that the cohort of surgeon respondents had a high level of awareness of the importance of abdominal wall closure and possible problems deriving from it. However, the survey revealed a lack of uniformity and basic knowledge regarding the technical aspects of closure and the prevention of postoperative incisional hernias or evisceration.
60% of respondents set the incidence of incisional hernias above 15% and considered that the laparotomy closure technique was the most important factor involved in their appearance. Our opinion is that this could imply that an unsatisfactory result of a basic surgical technique such as abdominal wall closure is being accepted. This is corroborated by recent studies1–3 where, after comparing different sutures, the authors concluded, as did our respondents, that the problem is not the material used but the closure technique employed.
Surprising differences were detected in the section on technique. We therefore find it surprising that 33% of respondents continue to believe that suturing in layers is appropriate when there is sufficient scientific evidence to support closure of the midline in a single layer.4,5 We also consider it unusual that 66% consider retention sutures useful when evidence shows that they are superfluous; there is debate as to whether they prevent fascial dehiscence and they are also associated with considerable complications.6–10 Furthermore, the lack of knowledge about and application of the 4:1 rule for abdominal wall closure is surprising; it seems incomprehensible that half of the participating surgeons should be either unaware of a scientifically contrasted, basic, technical aspect11–13 which has been used for many years, or not know how to apply it. These results lead us to believe that some reflection is required on the need to implement mechanisms to evaluate how abdominal wall closure is being performed in our country and about the results that are being achieved. Such an evaluation would enable the detection of shortcomings and introduce corrective measures to improve and unify technical criteria and optimize the results of abdominal wall closure.
87% of participants consider that prevention of incisional hernia is possible and 54% believe that improved technique is the most important element in prevention. The methods used in patients with risk factors are widely disperse. Of note is the fact that 50% of the surgeons participating in the survey still use retention sutures in these patients, particularly if we take into consideration that 84% of them agreed that mesh could be a useful method of prevention, although 40% acknowledge they never use them. The use of mesh as prophylaxis is questioned in some cases (contaminated or dirty surgery), but it has been demonstrated as effective in several studies involving high risk patients.14,15
The comparison of responses from qualified and trainee surgeons highlighted that many training aspects may not be being consistently conveyed. The fact that 57% consider suturing in layers a better technique when the majority of trainees chose closure using continuous suture, could be explained by the fact that some residents count all layers up to the skin. It is surprising, however, that over 50% of specialist surgeons state they are unfamiliar with the 4:1 rule whilst 61% of residents knew how to apply it. Practically 50% of both groups believed retention sutures to be the best method of preventing incisional hernias.
Respondents highlighted that technical aspects are key to whether or not an incisional hernia will develop.1–3 Therefore, given that the prevalence of incisional hernias continues to be a problem, one possible explanation could be the lack of adequate “surgical education” on the essential technical aspects for opening and closing an abdominal wall. It is over 30 years since laparotomy closure using a ratio of suture length to wound length of 4:1 was described as cost effective and helpful in reducing the occurrence of incisional hernia. Despite this, many surgeons are unaware of the importance of the closure technique or are not meticulous in this regard. A recent survey16 carried out in twelve surgical departments evaluated elective laparotomy closure techniques but did not reach any consensus on wall closure, only on skin closure. Another equally recent study,17 assessing resident's knowledge of abdominal wall closure, showed that although they possessed sufficient technical skill in closing an abdominal wall proficiently, only 10% knew about the 4:1 ratio and only 40% were familiar with any of the relevant medical literature on abdominal wall closure technique.
In the above context, it appears that the lack of “surgical education” as one of the factors in the development of incisional hernia and thus associated with one of the most accessible prevention targets (technique) should require greater attention if we are to reduce the prevalence of incisional hernias.
The abovementioned factors corroborate the need to unify criteria and increase training and research on abdominal wall closure in our country, and even the need to implement measures to certify that specialist and trainee surgeons are able to perform this technique appropriately. Scientific societies should become involved in this regard.
Conflict of InterestThe authors declare that there is no conflict of interest.
The following questionnaire concerns elective laparotomy.
- 1
What do you consider to be the best incision for most abdominal surgery?
- a
Midline laparotomy.
- b
Paramedian lateral laparotomy.
- c
Transverse laparotomy.
- a
- 2
What do you consider the best type of suture for a laparotomy closure?
a. Slow absorbable suture.
b. Unreabsorbable suture.
c. Others, which:…
- 3
What do you consider the best suture technique for a midline laparotomy?
a. Continuous suture.
b. Interrupted suture.
c. Continuous and interrupted suture.
d. Others, which:…
- 4
What do you consider the best suture technique for transverse laparotomy?
a. Continuous suture.
b. Interrupted suture.
c. Continuous and interrupted suture.
d. Others, which:…
- 5
What do you consider the best suture technique for midline laparotomy?
a. Suturing in layers.
b. Single layer suturing.
c. Others, which?:…
- 6
What do you consider the best suture technique for transverse laparotomy?
a. Suturing in layers.
b. Single layer suturing.
c. Others, which?:…
- 7
Do you think retention sutures are useful in laparotomy closure?
a. Yes.
b. No.
c. I don’t know.
- 8
Are you familiar with the 4:1 suture rule for laparotomy closure?
a. Yes.
b. No.
- 9
Do you think that at least the 4:1 rule should be applied in laparotomy closure?
a. Yes.
b. No.
c. I don’t know.
- 10
What do you think is the percentage of appearance of an incisional hernia following midline laparotomy?
a. 5%.
b. 10%.
c. 15%.
d. 20%.
e. Higher than the above.
- 11
What do you think is the most important factor in the appearance of incisional hernia?
a. Wound healing.
b. Patient history.
c. Wall closure technique.
d. I don’t know.
- 12
Do you think incisional hernias can be prevented
a. Yes.
b. No.
c. I don’t know.
- 13
What do you think is the most important factor in the prevention of incisional hernia?
a. Better knowledge of wound healing.
b. Optimizing patient history.
c. Improving the wall closure technique.
d. I don’t know.
- 14
Do you think adding a prosthesis when you close a laparotomy could reduce the appearance of an incisional hernia?
a. Yes.
b. No.
c. I don’t know.
- 15
Do you use prophylactic mesh:
a. Never.
b. In elective surgery in high-risk patients.
c. Only in emergency laparotomy.
d. In elective and emergency surgery.
- 16
What method do you use to prevent incisional hernia/evisceration in high-risk patients?
a. Mesh.
b. Retention sutures.
c. None.
- 17
What technique do you use to repair postoperative evisceration?
a. Continuous suture.
b. Retention sutures.
c. Mesh only in non contaminated site.
d. Mesh always.
- 18
What type of surgery do you most frequently perform?
a. Colorectal.
b. Oesophagogastric.
c. Endocrine and metabolic.
d. Hepatobiliopancreatic.
e. Abdominal wall surgery.
f. General surgery.
g. Other.
- 19
Do you think that prevention is more important in some surgery than in others?
a. Colorectal.
b. Oesophagogastric.
c. Endocrine and metabolic.
d. Hepatobiliopancreatic.
e. Abdominal wall surgery.
f. General surgery.
g. Other.
h. None are more important than the others; they may all equally lead to incisional hernia.
i. I don’t know.
- 20
What is your career stage?
a. Specialist.
b. Resident.
Please cite this article as: Pereira JA, López-Cano M, Marsal F, Feliu X. Resultados de una encuesta nacional sobre el cierre de la pared abdominal. Cir Esp. 2013;91:645–650.
