




Malignant tumors of the aorta are extremely rare. In most cases, the diagnosis is established when the disease is already advanced, and survival is usually only a few months.1,2 We present the case of a patient with angiosarcoma of the aorta that initiated as a ruptured pseudoaneurysm and was diagnosed after surgery for gastrointestinal bleeding caused by duodenal infiltration.
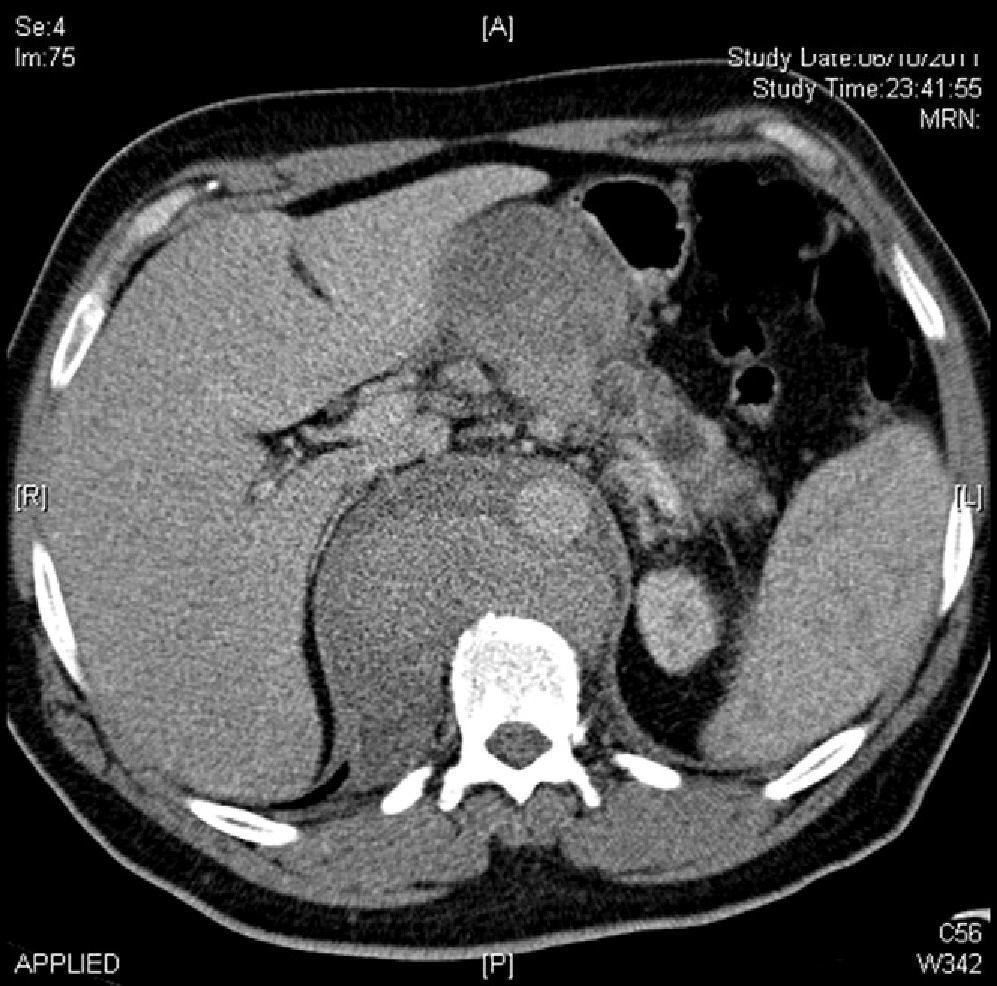
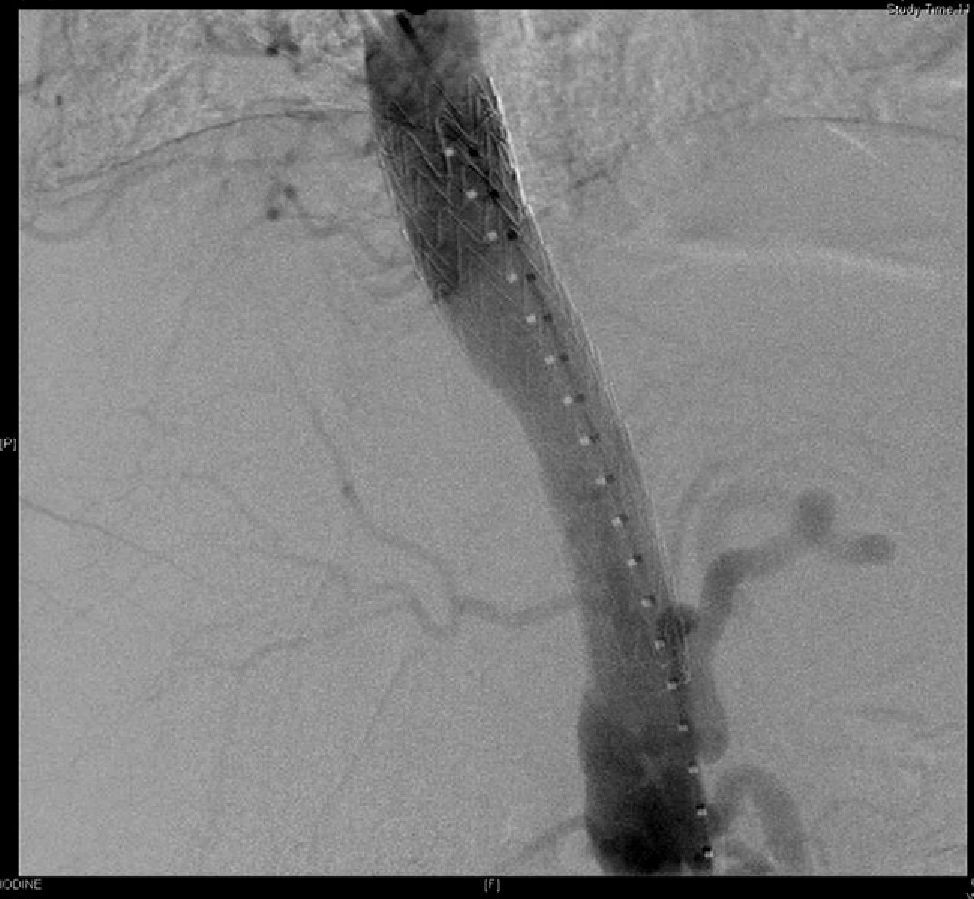
The patient was a 49-year-old male who was hospitalized for progressive abdominal pain accompanied by nausea, constipation and a weight loss of >15% over the course of the previous 2 months. Endoscopic study of the patient was normal. Abdominal CT scan identified an aortic pseudoaneurysm with a contained rupture 4cm from the origin of the superior mesenteric artery, adjacent to the first duodenal branch, measuring 9mm×8mm in diameter, and an aneurysm neck measuring 4mm (Fig. 1). We decided to implant an aortic prosthesis (31mm×15cm). The distal end was situated 1cm from the celiac trunk and was sealed with a tri-lobe balloon catheter (Fig. 2).


The patient was discharged from the hospital after one week but was re-admitted 10 days later due to an episode of upper gastrointestinal bleeding. Upper GI endoscopy revealed bleeding at the duodenal level that could not be sclerosed. We therefore ordered thoracic and abdominal CT studies with contrast, which showed a hematoma in the duodenal region with signs of active bleeding. The gastroduodenal artery was embolized. Due to persistent gastrointestinal bleeding, we decided to perform exploratory laparotomy, where we observed bleeding in the 1st and 2nd portions of the duodenum. Subtotal gastrectomy was performed and samples were sent for pathology studies. The duodenum was packed with gauze, which was removed 72h later. The results of the pathology report showed that the small intestine wall was infiltrated by a poorly differentiated malignant neoplasm compatible with high-grade angiosarcoma of large blood vessels, probably originating in the aorta. Once week later, the patient continued to become more anemic due to gastrointestinal hemorrhage and blood loss through the drain tubes, resulting in his death.
Angiosarcoma of the aorta is a very rare entity that is difficult to diagnose preoperatively. Furthermore, even if complete resection is performed, long-term survival is improbable.3
Most of these cases present as ruptured aneurysms, which are initially attributed to an arteriosclerotic etiology. Therein lies the reason for the late diagnosis made in almost all the cases reviewed in the literature.4 Other rarer complications that may present are cerebral infarction, spontaneous paraplegia and gastrointestinal bleeding secondary to metastasis.5
The definitive diagnosis is established by the pathology study of the fragment from the affected artery, the possible peripheral embolization that it may cause or, as in our case, local infiltration of the digestive tube. The radiological findings are frequently non-specific, so it is not possible to make a preoperative radiological diagnosis of this pathology.6 The morphology and the segment of the obstruction of the aortic lumen without aneurism could assist the differential diagnosis of intravascular malignant diseases.7
According to the growth pattern type, these tumors are classified as intimal, polypoid (intraluminal) or adventitial (or mural). The intimal and polypoid types can have a tendency to extend along the surface of the intima and, frequently, to form intraluminal polyps that can cause embolic phenomena.8
Since the metastases of this type of tumor are mainly located in the bones, bone scintigraphy is recommended in order to substitute the affected fragment with a prosthesis (if there are no metastasis) or an endarterectomy with confirmation of resection in the margins of the removed surgical specimen.9,10
In conclusion, this disease continues to have a very difficult preoperative diagnosis. It should be included in the differential diagnosis in cases of aortic aneurysm disease in order to be able to make an early diagnosis and for definitive treatment.
Please cite this article as: Santana-Cabrera L, Jaimes-Vivas RJ, Galante Miliqua M, Lorenzo Torrent R, Sánchez-Palacios M. Rotura de aorta torácica descendente afectada por un angiosarcoma. Cir Esp. 2014;92:501–503.
