




A 77-year-old male patient with several pathologies (ASA IV, Charlson Comorbidity Index 7) and a history of recurrent acute cholecystitis managed conservatively on 4 occasions consulted for pain in the right hypochondrium and fever. Urgent lab work showed elevated acute phase reactants.
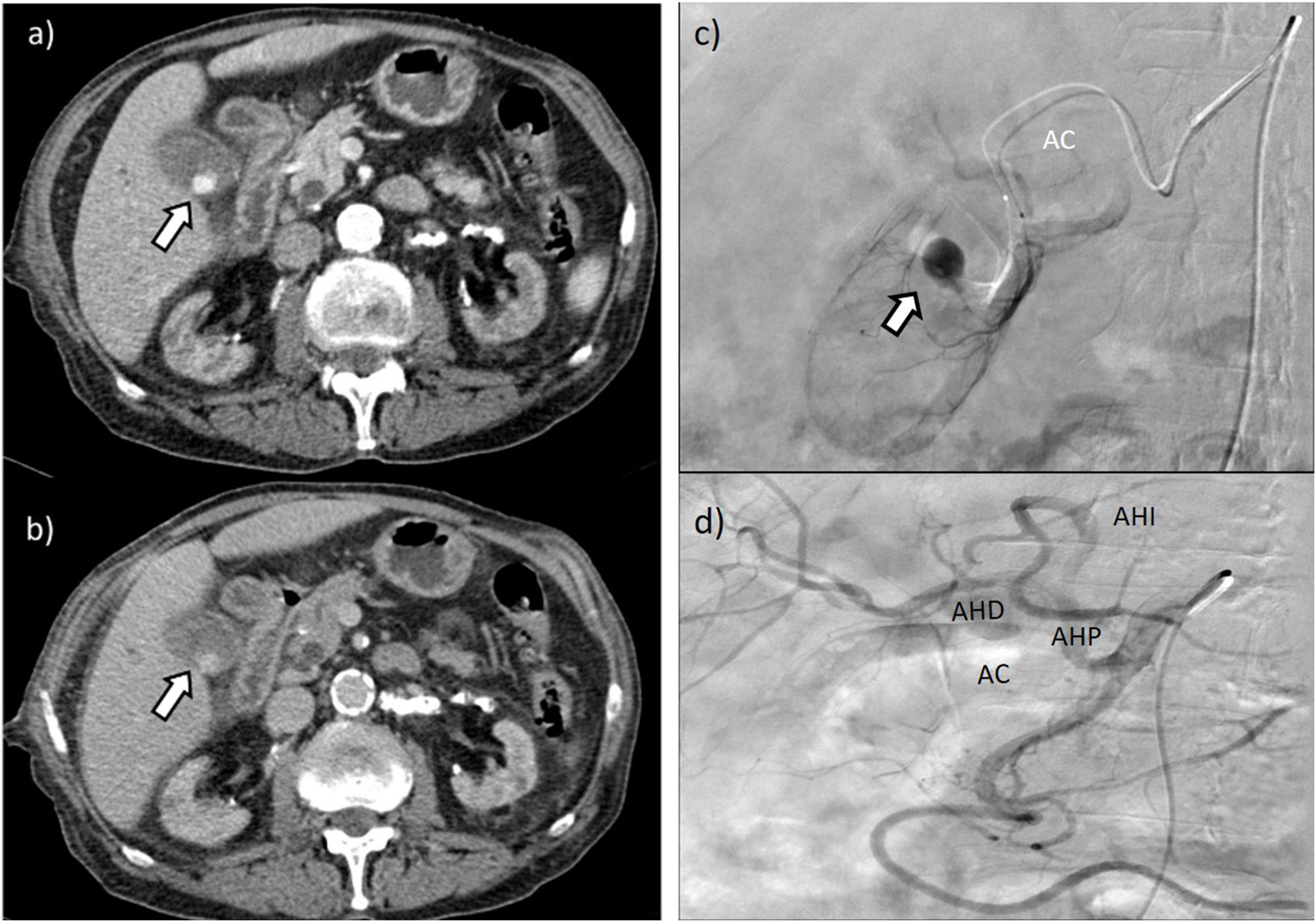
Abdominal ultrasound was compatible with acute gangrenous cholecystitis, revealing a gallbladder occupied by hypoechoic material. As we suspected a concomitant respiratory infection, a computed tomography scan was ordered, which demonstrated a hyperdense image in the gallbladder during the arterial phase and contrast washout in the late phase, suggestive of an endoluminal pseudoaneurysm of the cystic artery. We performed arteriography with super-selective catheterization of the branch of the cystic artery that supplied the pseudoaneurysm. Due to its size, embolization was performed with BioGlue®. Subsequently, we conducted laparoscopic cholecystectomy, with no intraoperative or postoperative incidences (Fig. 1).
Funding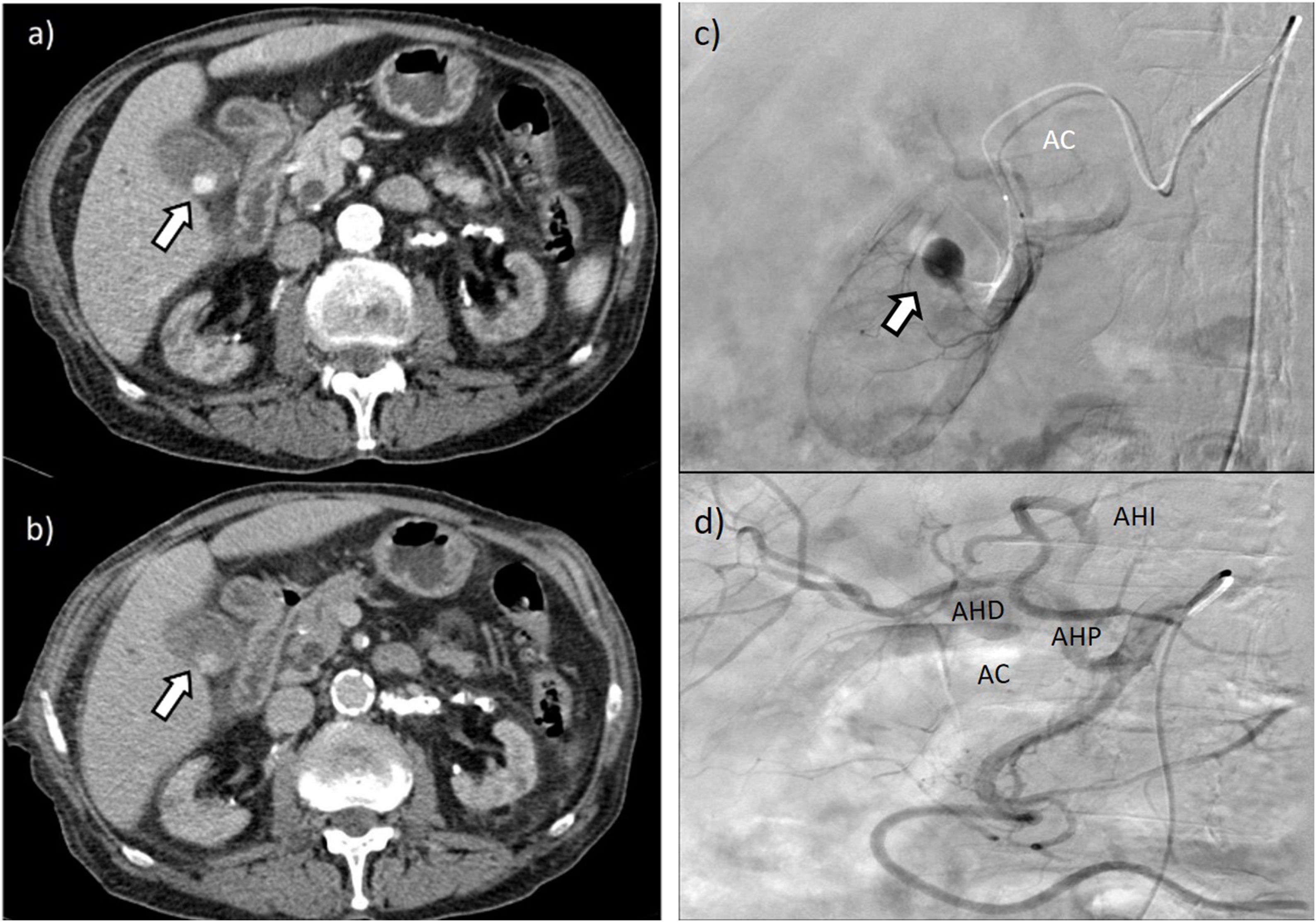
No funding was received for this article.
Please cite this article as: Tovar Pérez R, Di Martino M, Blanco Terés L, Martín-Pérez E. Seudoaneurisma de arteria cística secundario a colecistitis aguda. Cir Esp. 2022;100:171.
