




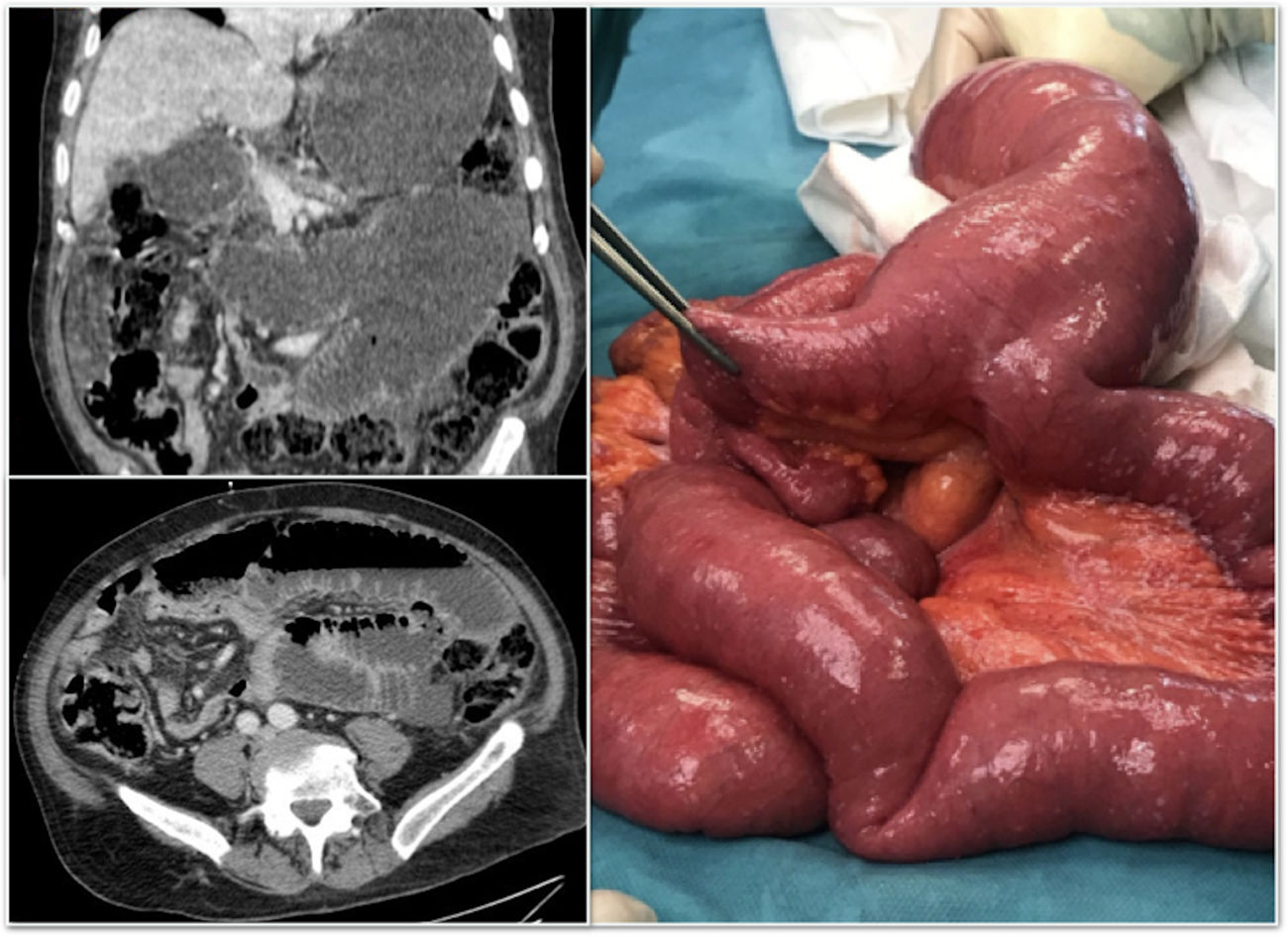
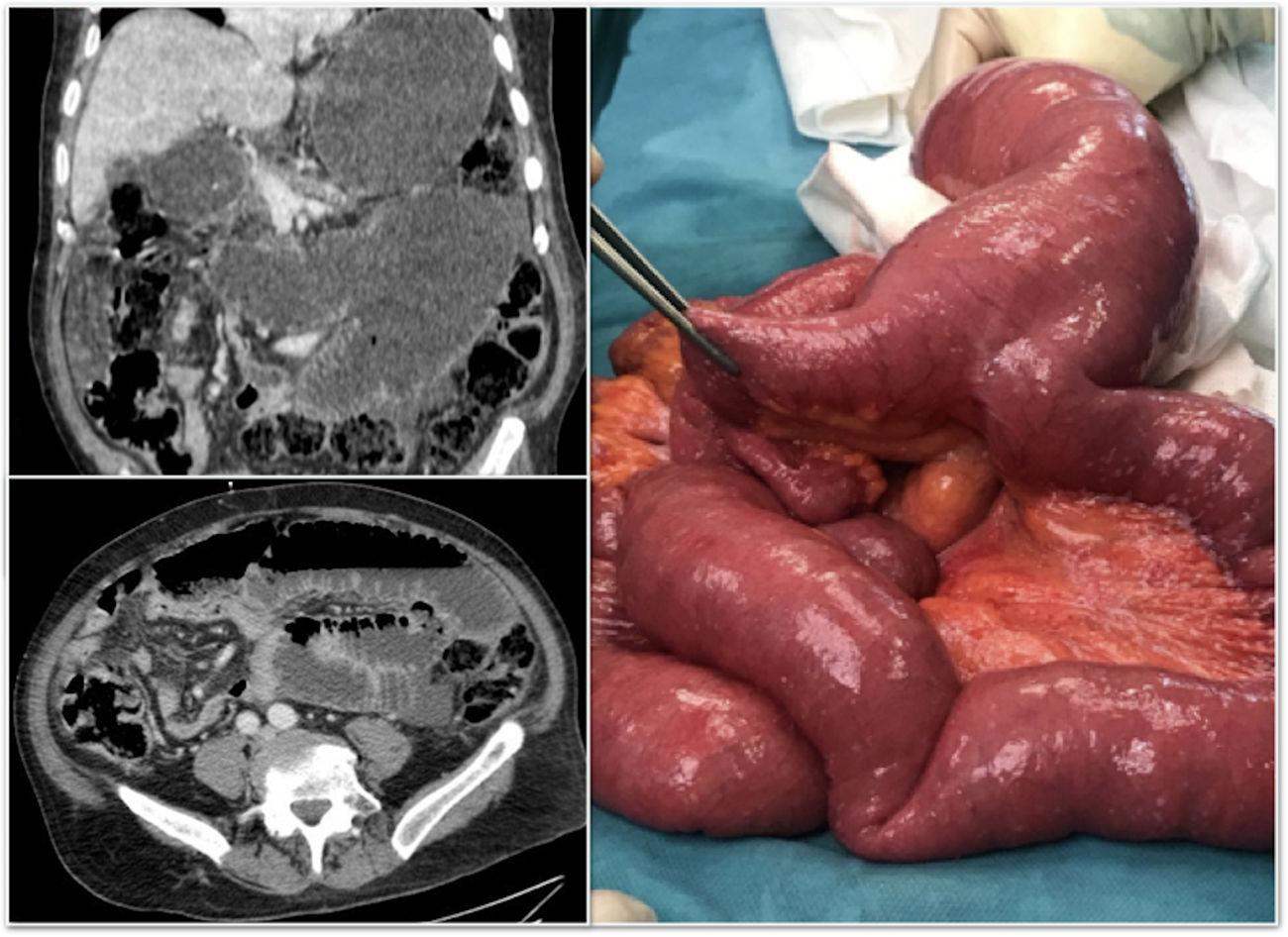
Male patient of 73 years, carrier of a gastrostomy. Go to the emergency department for abdominal pain, nausea and vomiting. The examination revealed a distended and tympanic abdomen, without signs of peritoneal irritation. The laboratory test shows an increase in acute phase reactants. In the abdominal X-ray, dilatation of the small intestine and air-fluids levels its observed, performing a CAT scan that shows a change in caliber in mesogastrium, suggestive of adhesions. Surgical intervention was performed, showing a large diverticulum of Meckel (Fig. 1), twisted, generating a retrograde dilation. A diverticulectomy is performed with a favorable evolution.
Please cite this article as: Vivas Lopez A, Pastor Altaba D, Nutu O-A, Marcacuzco Quinto A. Divertículo de Meckel gigante: causa infrecuente de obstrucción intestinal. Cir Esp. 2019;97:405.
