





The development of robotic surgery over the last 10 years has presented an average annual growth rate of about 15%. From 1999 to June 2011, Intuitive Surgical, the company that manufactures the da Vinci system, sold 1744 units throughout the world. Of these, 1277 are found in hospitals in the United States, 324 in Europe, 96 in Asia, 16 in the Middle East and 14 in Australia. Italy and Germany have 50 da Vinci units each, which is the highest number in Europe, and Spain has 24. In 2010, the 50 Italian robots were used for nearly 5000 procedures, a number that is expected to surpass 6000 in 2012.1 The majority of these operations are radical prostatectomies, representing approximately half of the total, followed by a combination of other general surgery procedures. These numbers show a significant trend toward increased propagation and routine use of the only surgical system available assisted by robotics, which has extended throughout the world and to all surgical specialties.
Nevertheless, for many general surgeons, it is still not clear what the true benefit of robotic surgery is or what its current limitations are.2 Critics argue that users and hospitals are exaggerating the supposed advantages of this technology and state that we still lack objective, scientific evidence demonstrating that robotic surgery is better than conventional laparoscopy for general surgeons.3 The current financial limitations of most healthcare systems in Western countries have led to added concerns regarding the use of robotic surgery, which is perceived as a privilege for a select few public hospitals and private centers, rendering the decision-making process even more complex for health-care administrators.4 It is not surprising that the scientific information and the messages in the media about robotic surgery are still confusing and often offer opposing points of view; meanwhile, the technology is still rapidly evolving and incorporating new tools and innovative instruments. In this review, I will try to center my attention, from my perspective as a basic user, on the pros and cons of current robotic systems in general surgery, and I will offer a general view of their expected future evolution.
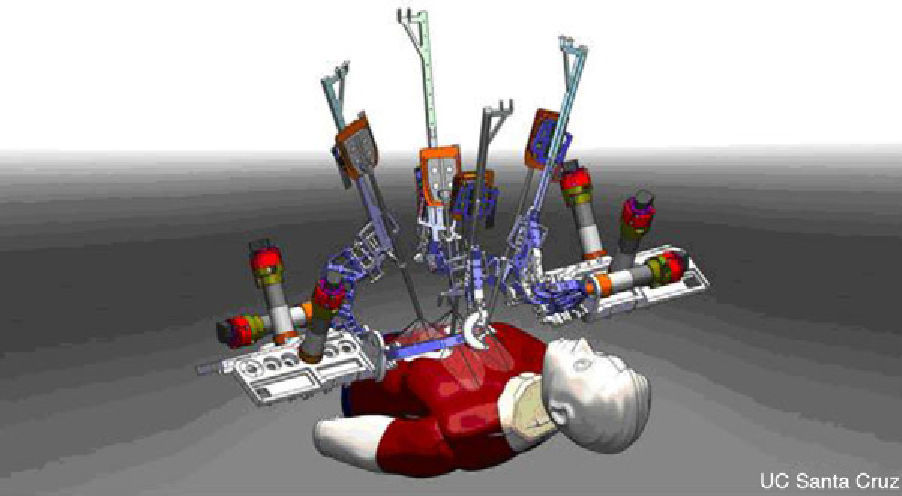
The Problem is the CostThe da Vinci system is manufactured by Intuitive Surgical, a company with headquarters in California that is currently the only big player in the robotic surgery business. Founded in 1995, the company has adapted technology that was originally designed for long-distance remote surgery, producing several generations of multi-use robots before the latest version: the “da Vinci Si” 4-armed double console system, with a price tag of around 2 million dollars (Fig. 1). The da Vinci robotic system is still monopolizing the market; obviously, competition would drive the price down. Another medical company called Computer Motion (manufacturer of another surgical robot, Zeus) merged with Intuitive Surgical in 2003, and many designs from its old competitor have been incorporated into the new da Vinci system.5 Intuitive Surgical now has dozens of patents that make it extremely difficult in the immediate future for any competing surgical robot to be launched. Nonetheless, as these patents gradually expire, other competitors will appear. It is expected that at least one other figurehead will appear on the market in the near future: the Canadian robot Amadeus by Titan Medical, Inc., which is expected to incorporate haptic technology (tactile interface). This robot will soon be involved in clinical trials, but little is known about its performance. Lastly, the Raven robotics program, originally developed for the US Army, has produced a surgical robot that is compact, light and relatively cheap (it should cost around $250000) (Fig. 2). In the near future, it may become a product apt for cardiac surgery, and it enjoys the academic support of several universities in the US, led by the University of Washington. Nevertheless, at present it lacks FDA approval. Therefore, during the next few years, it is likely that the da Vinci system will continue to be the only surgical robot available for general surgeons and its price will continue to remain high and inaccessible for many users.
General Surgeons Have no Robotic Procedure Without Competition
.")
For urologists, radical prostatectomy is what might be called a “killer procedure”, or without competition, meaning that there is no therapeutic alternative that has survived after its introduction into clinical practice.6 There are four points that a surgical procedure should meet to become an unequaled procedure:
- (1)
It must be a common procedure (nearly 100000 radical prostatectomies are done per year in the US).
- (2)
It must be an enabling technology (it can only be done by robot, since the alternative is open surgery).
- (3)
It must provide improved clinical results (robotic prostatectomy is associated with improved functional results over the short and long term).
- (4)
It must be reproducible (most urologists have adopted the new technique with ease).
In general surgery, there is no procedure that meets these criteria because most operations that are done with the da Vinci can also be done by laparoscopy, which is a simpler, less expensive method. Instead of an “enabling technology”, the robot in general surgery is more of a “facilitating technology”. Thus, laparoscopic surgery purists see no additional benefit in the use of robotic surgery, which leads to criticism about its additional expense.7
The question is: is there a place for still-expensive “facilitating technology” within the field of minimally invasive general surgery? The answer is still uncertain. It may be “yes” when we consider that only 20%–25% of colorectal cancer is treated with laparoscopy, probably due to the intrinsic technical difficulties of this method. Technology that is able to simplify laparoscopy can result in greater diffusion of the minimally invasive option and proven benefits for patients. The same is true for more advanced laparoscopic procedures, which are now restricted by their limited diffusion.
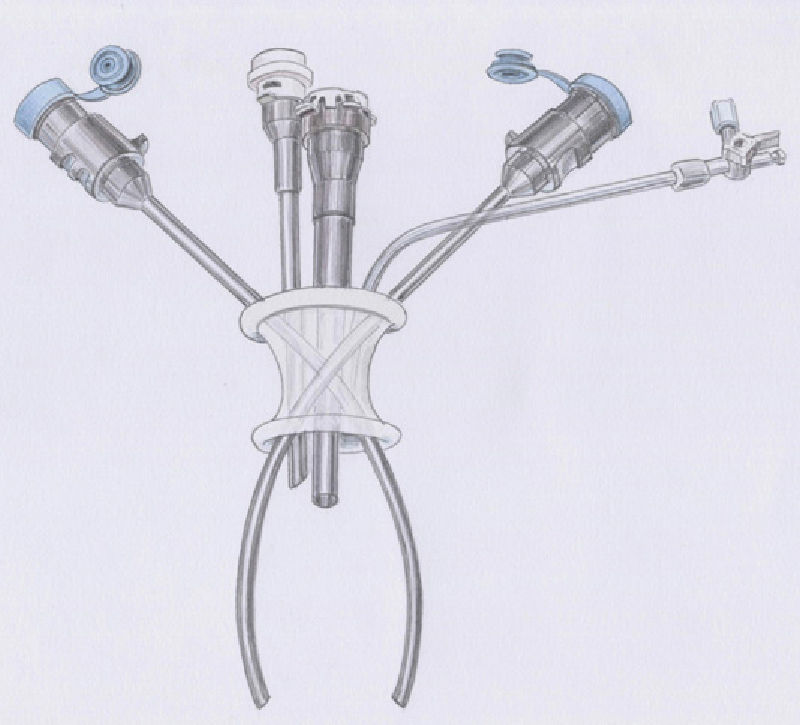
Robotic Single-Port SurgeryRecently, new instruments have been developed for the da Vinci Si system as well as single-port accessories that have been tested in humans in preliminary studies.8,9 This new technology has the potential to surpass many limitations of classic single-incision laparoscopic surgery (SILS) regarding triangulation, ergonomics, quality visibility and range of movement of the instruments. The robotic forceps automatically recognize the shape of the single-access curved cannulas and reassign each master control to the instrument on the opposite side, thus compensating for the cross-over of the curved cannulas (Fig. 3). The system includes a series of 5-mm semi-rigid, non-wristed instruments including a monopolar hook, different types of forceps, curved scissors, a medium-large Hem-o-lock clip applier (Teleflex Medical), needle holder and an aspirator-irrigator. The single access port is disposable; all the instruments are rechargeable with a limited number of uses and the metallic cannulas are reusable with disposable covers. The robotic technology is a compensatory technique that can overcome obstacles and the ergonomic limitations of SILS and is able to take advantage of all the potentials of the single-access approach. We have demonstrated that it allows users to quickly overcome the learning curve that is typical in most new procedures, particularly the single-incision laparoscopic approach.10 It is probable that this increases the safety of SILS and, at the same time, could make it more accessible to a larger number of general surgeons for more surgical procedures.

The future evolution of the single-access robotic system will probably lead to technological solutions for the challenges of natural orifice translumenal endoscopic surgery (NOTES), which has limited diffusion in practice due to its difficulty. Miniaturized, articulated and multi-area robotic tools will sooner or later substitute multi-port robotic approaches, and it is likely that this large jump forward can only come about with advances in robotic technology.
Training Future SurgeonsThe second console of the da Vinci Si system has been designed for educational purposes. In fact, the majority of minimally invasive procedures, both laparoscopic as well as robotic, require only one surgeon since the need for tissue exposure is less than in open surgery. However, the possibility that a surgeon in training can sit at the second console during a case of robotic surgery is a unique opportunity for sharing the same view as the operating surgeon in high-definition 3D. On the other hand, some steps of the procedure can be performed by the apprentice surgeon under the supervision of the surgeon in charge at the other console, who, after completely turning over the master controls, can use virtual pointers to direct the correct approach of the surgical dissection.11 In this way, double-console technology is the most powerful teaching device ever seen in surgery, even though its potential as a training tool has not yet been recognized. I firmly believe that teaching institutions should consider this important variable in the algorithm used when deciding to buy the robot or not. In my personal experience, it is much easier to teach young surgeons colorectal resection with robotics than with conventional laparoscopy.
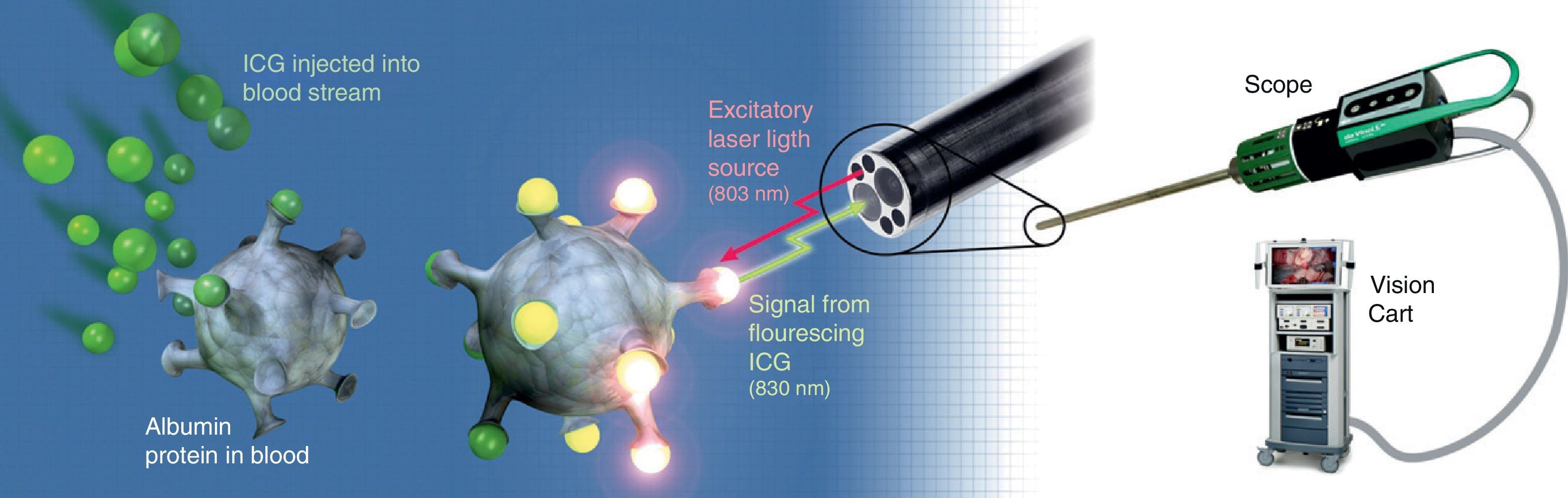
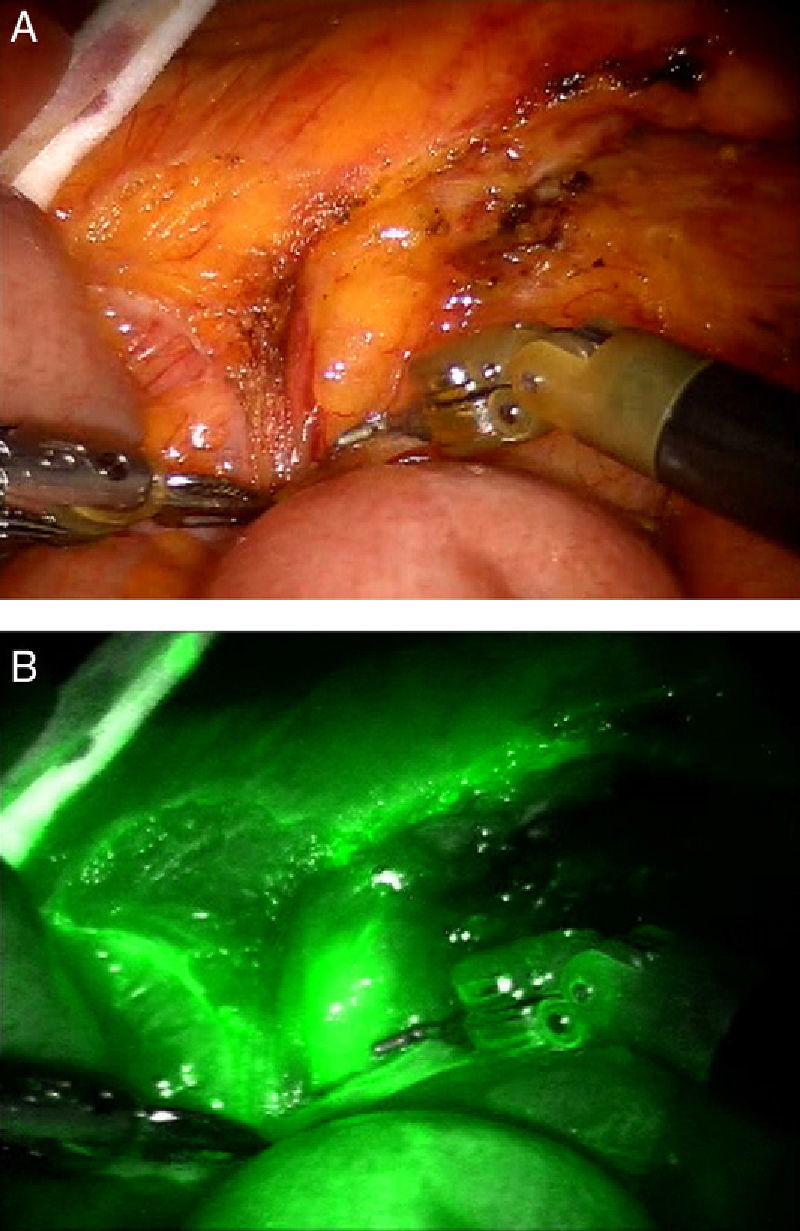
New Dissecting Tools and Firefly TechnologyThe new EndoWrist One is an articulated tool with radiofrequency that combines the sealing ability of this technology with an incorporated blade that cuts between clamps. With this new tool, robotic technologies close the gap with pure laparoscopy, in which the instruments for electrical dissection have been used for 10 years. The EndoWrist One system will accelerate robotic dissection, so surgery will therefore become much quicker and probably safer. The usual criticism about longer operating times in robotic surgery will probably disappear after the introduction of this technology. Firefly fluorescence technology provides imaging guides and real-time identification of anatomical reference points.12 The robot near-infrared camera enables visualization of vascularized tissue, vessels, lymph and bile ducts after the intravenous injection of indocyanine green (ICG), which is activated with near-infrared light (Fig. 4). The system is able to change between views of standard endoscopic images in real time and images of the tissues illuminated with the dye. Real-time visual demonstration of tissue perfusion can help the surgeon cut the intestine at the desired point and thus preserve blood flow. In addition, given that the staining of neoplastic tissue is different from that of healthy tissue, it could help differentiate between malignant and normal tissues.13 During robotic surgery, anomalies in the anatomy of the bile duct could also be detected; therefore, the possibility arises for this technique to replace intraoperative cholangiography as a standard for evaluating the biliar anatomy.14 The use of ICG as a contrast medium can show bile leaks on the surface of the transection after hepatectomy. Direct endoscopic injection of ICG could be used in colorectal cancer to detect the lymphatic dissemination trajectory and obtain samples of sentinel lymph nodes15 (Fig. 5A and B). Although this technique has still not been approved in the framework of colorectal cancer, it could be valuable to avoid unnecessary extensive resection during the early stage of the disease. It is likely that the future evolution of this visual detection technology will bring about more selective stains that are able to distinguish between metastatic and reactive lymph nodes, which would give way to tailored oncologic surgery to patients of the future.
Conclusion
 standard endoscopic view; (B) view with Firefly demonstrating dye uptake by the lymph node.")
In 1983, a mobile phone cost 4000 dollars. The battery charge lasted only 20min, and their size, shape and weight were similar to that of a brick. Today, robotic surgery is in its infancy, like the mobile phone industry was in the 1980s. We all know the rest of the cell phone story, but we can only make assumptions about the future of surgical robots. As more manufacturers join the robotics market, the speed of innovation will accelerate and costs will come down. Tool miniaturizations and augmented reality will help us carry out a wide range of procedures more quickly and safely. The educational potential of robotic systems like the da Vinci Si could change the traditional methods used for teaching surgical techniques in recent decades.
I have little doubt that robotic surgery is here to stay and that the new generation of surgeons should have the opportunity to be trained with these systems.
Please cite this article as: Pietrabissa A, et al. Cirugia robótica: controversias actuales y expectativas futuras. Cir Esp. 2013;91:67–71.
