




The definitive acceptance of an organ as valid for transplant depends on the surgical team performing the multiorgan recovery; and unexpected difficulties can occur. The demographic characteristics of donors have changed, and some accepted donors can present difficulties in surgical technique and risky decisions on the validity of the retrieved organ or organs. An alternative method to the cannulation of the abdominal aorta is proposed when there is evidence of disease in the infrarenal aorta during the multiorgan procurement. The retrocardiac descending thoracic aorta is cannulated using an antegrade perfusion; this technique allows an increase in organ recovery.
La aceptación definitiva de un órgano como válido depende del equipo quirúrgico que realiza la extracción multiorgánica, que tendrá de enfrentarse en muchas situaciones a dificultades inesperadas. Las características demográficas de los donantes han cambiado, se aceptan donantes de órganos que hace no muchos años considerábamos subóptimos, lo que implica muchas veces una técnica quirúrgica difícil y una toma de decisión acerca de la validez del órgano u órganos muy arriesgada. Se propone un método alternativo a la canulación de la aorta abdominal cuando se evidencie enfermedad de la aorta infra-renal durante la realización de la extracción multiorgánica. Se realiza la canulación de la aorta torácica descendente retrocardíaca con una perfusión anterógrada, esta técnica permite aumentar el número de órganos a trasplantar.
The surgical technique described by Starlz et al.1,2 in 1984 for multiple organ extraction and its later modifications according to the abdominal organs to be extracted (intestine, pancreas, liver, kidneys, heart and lungs) has been used extensively. The same is true for the Nakazato et al.3 modification in 1991 (total abdominal evisceration) for hemodynamically unstable patients. Undoubtedly, these are the current gold standard techniques in this field.
In recent years, however, transplantation groups have witnessed an important change in the organ donor profile. Thirty years ago, donors were young polytrauma patients who had been in traffic accidents, but now many are elderly patients with occlusive atherosclerotic disease of the infrarenal aorta. This condition is a serious handicap during the cannulation and arterial perfusion of abdominal organs. Massive atherosclerosis and aneurysmatic dilatation of the aorta wall impede cannulation of the abdominal aorta and retrograde perfusion of the organs, causing the loss of the organ to be transplanted. Cannulation of a diseased aorta entails the dissection of its intima, creation of a false lumen, and the embolization of detritus and thrombotic material towards the ostia of the renal arteries and the celiac trunk, causing suboptimal perfusion and loss of the organs. Therefore, several authors have proposed cannulation of the thoracic artery. Fukuzawa et al.4 expose the descending aorta using medial retraction of the left lung. Benedetti et al.5 use cannulation of the aortic arch, Reich et al.6 dissect the diaphragm in order to insert the cannula in the supraceliac aorta, and Kollar et al.7 only dissect the pericardium behind the heart in order to access the aorta and insert a cannula at a right angle for perfusion.
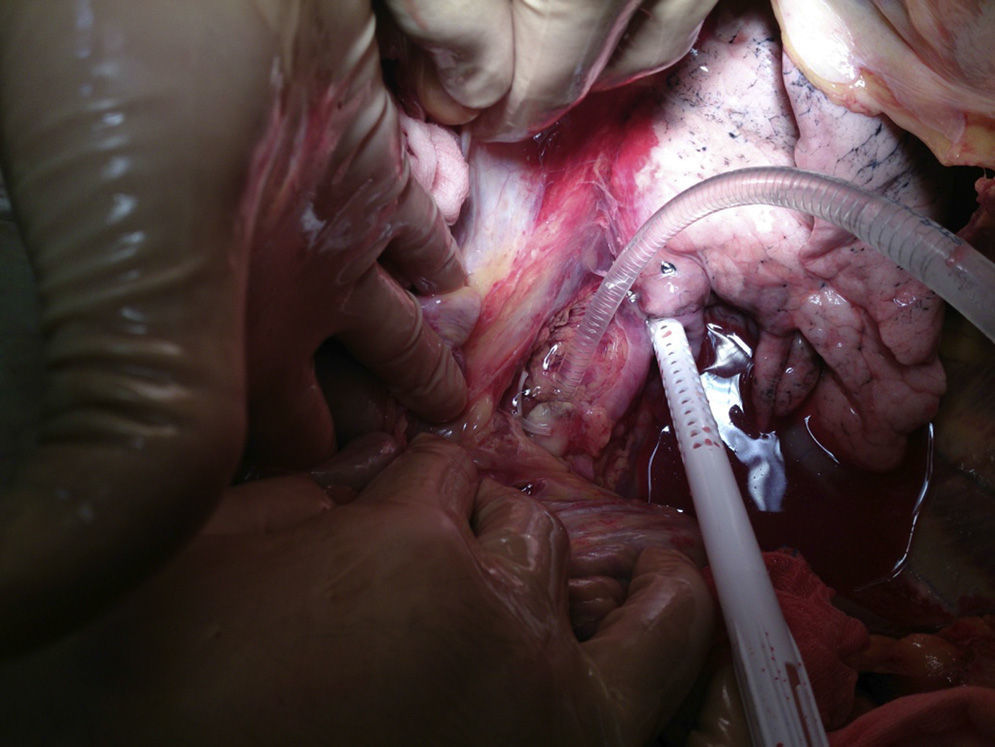
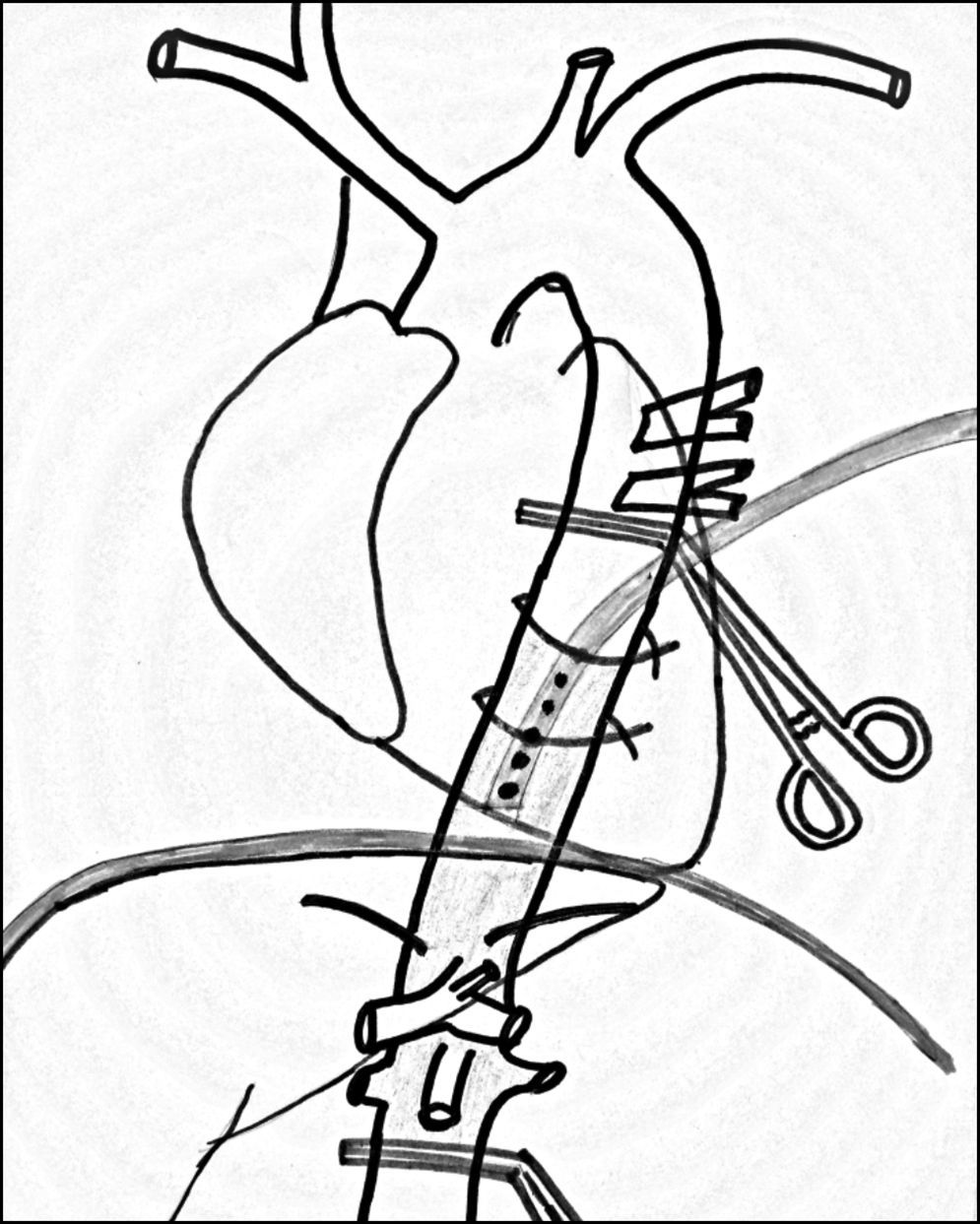
Materials and MethodsThe procedure begins with sternotomy and midline-cross laparotomy. The abdominal aorta is examined; if there is any important atherosclerotic or aneurysmatic disease, we modify the initial strategy by dissecting and controlling the descending thoracic aorta with a tie, after which we assess and consider whether the abdominal organs are potentially valid. To do so, we dissect the left mediastinal pleura, the diaphragm along the mid-line above the esophageal hiatus, and the left pulmonary triangular ligament up to where the left inferior pulmonary vein meets the left atrium; in this manner, the retrocardiac space is accessed, providing an approach of the descending thoracic artery with very simple dissection in a very short period of time (2min on average). The thoracic artery is clamped underneath the left inferior pulmonary vein, the perfusion cannula is inserted in the aorta right under the clamp (after systemic heparinization), and perfusion is initiated through the descending aorta with 4°C University of Wisconsin solution, clamping the abdominal aorta above the aortic bifurcation (Figs. 1 and 2). This approach of the thoracic artery is simple, quick, and it avoids dissection of the retroperitoneum, which, in patients with previous abdominal surgeries, retroperitoneal hematomas or abdominal aortic disease, is difficult as well as tedious. These conditions considerably slow down and complicate surgery and may even cause the loss of the organ or organs to be transplanted.


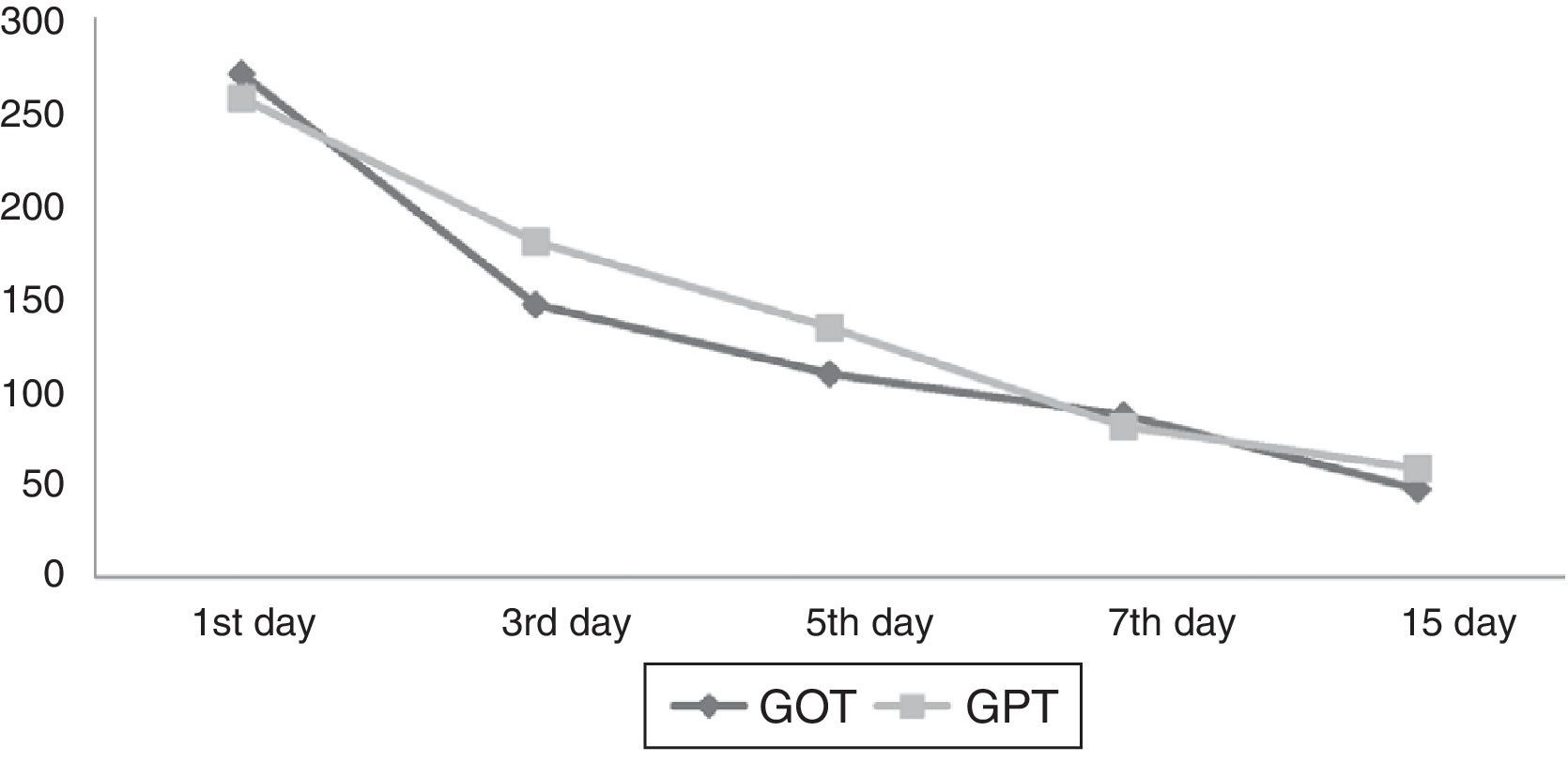
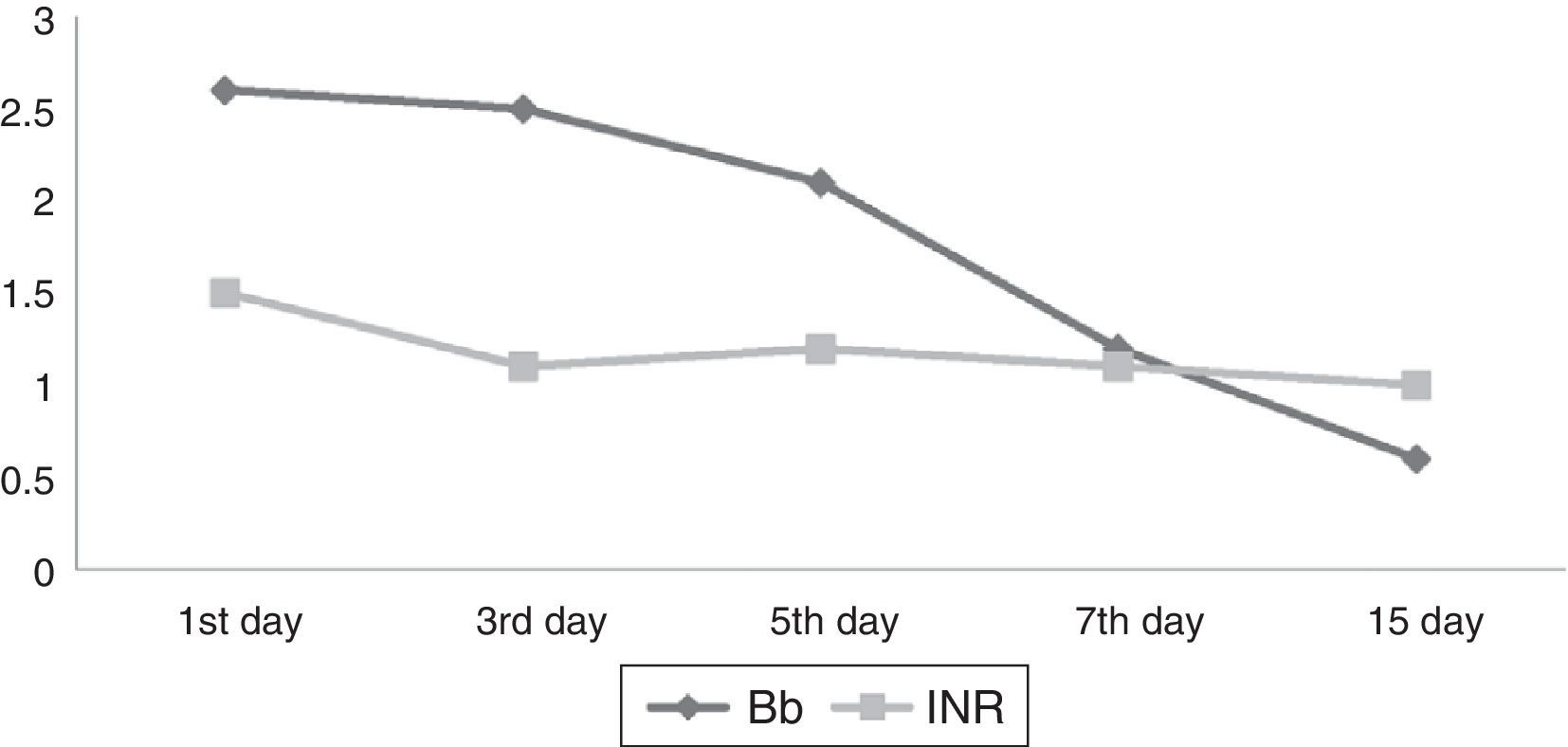
We have used this technique in 8 organ donors with atherosclerotic infrarenal aorta (5 with aneurysmatic disease of the infrarenal aorta; in one case it was possible to simultaneously extract both lungs). The volume of perfused liquid was the same as in the standard procedure (4L through the aorta, 2L through the portal vein). In all cases, the purge speed was excellent (10–15min) and all the organs were successfully transplanted, while no cases presented primary graft dysfunction (Figs. 3 and 4). Mean post-transplantation hospital stay was 21 days. After a mean follow-up period of 18 months, there have been no organ rejections and the recipients have maintained normal liver function.

 and INR (Quick time) values from days 1, 3, 5, 7 and 15 after liver transplantation.")
The technical modification described here is simpler because it eliminates the need to expose the supraceliac abdominal aorta, as described by Reich et al., which is sometimes very difficult and time-consuming. Furthermore, there may be inadvertent injury to a left hepatic artery originating in the left gastric artery. The proposed cannulation technique is much less complicated and faster than the method proposed by Fukuzawa and Benedetti because there is extensive exposure of the thoracic aorta from the inferior pulmonary vein. Minimal dissection is necessary for successful cannulation, simply by surrounding the aorta with the dissector and using 2 ties. Moreover, it is possible to simultaneously extract the heart and lungs if there is collaboration with the cardio-thoracic surgery team.
ConclusionsWe believe that this technique is highly recommendable for patients with abdominal aortic disease or stents as well as for those with retroperitoneal hematomas. It is also an option to consider in hemodynamically unstable or obese patients and those with previous abdominal surgeries.
Conflicts of interestThe authors declare that they do not have any conflicts of interest.
Please cite this article as: González Rodríguez FJ, Fernández Pérez A, Conde Freire R, Martínez J, Varo Pérez E, Bustamante Montalvo M. Utilidad de la canulación de la aorta torácica con perfusión anterógrada en la extracción de órganos abdominales. Cir Esp. 2015;93:39–41.
