




Trauma injuries to the thoracic outlet are serious and can be life-threatening. Most patients with this type of injury die at the scene of the trauma event. Patients who arrive at the emergency room should be carefully evaluated. In case of hemodynamic instability, the most appropriate approach is surgery and, if large vessel injury is suspected, the best approach is sternotomy.1 However, in patients who are hemodynamically stable, the most appropriate option should be carefully evaluated for each case.
The presence of a sharp object lodged in the thorax makes this assessment difficult, as specific imaging tests, such as tomography, can present images that are difficult to interpret due to the artifact caused by the foreign object.
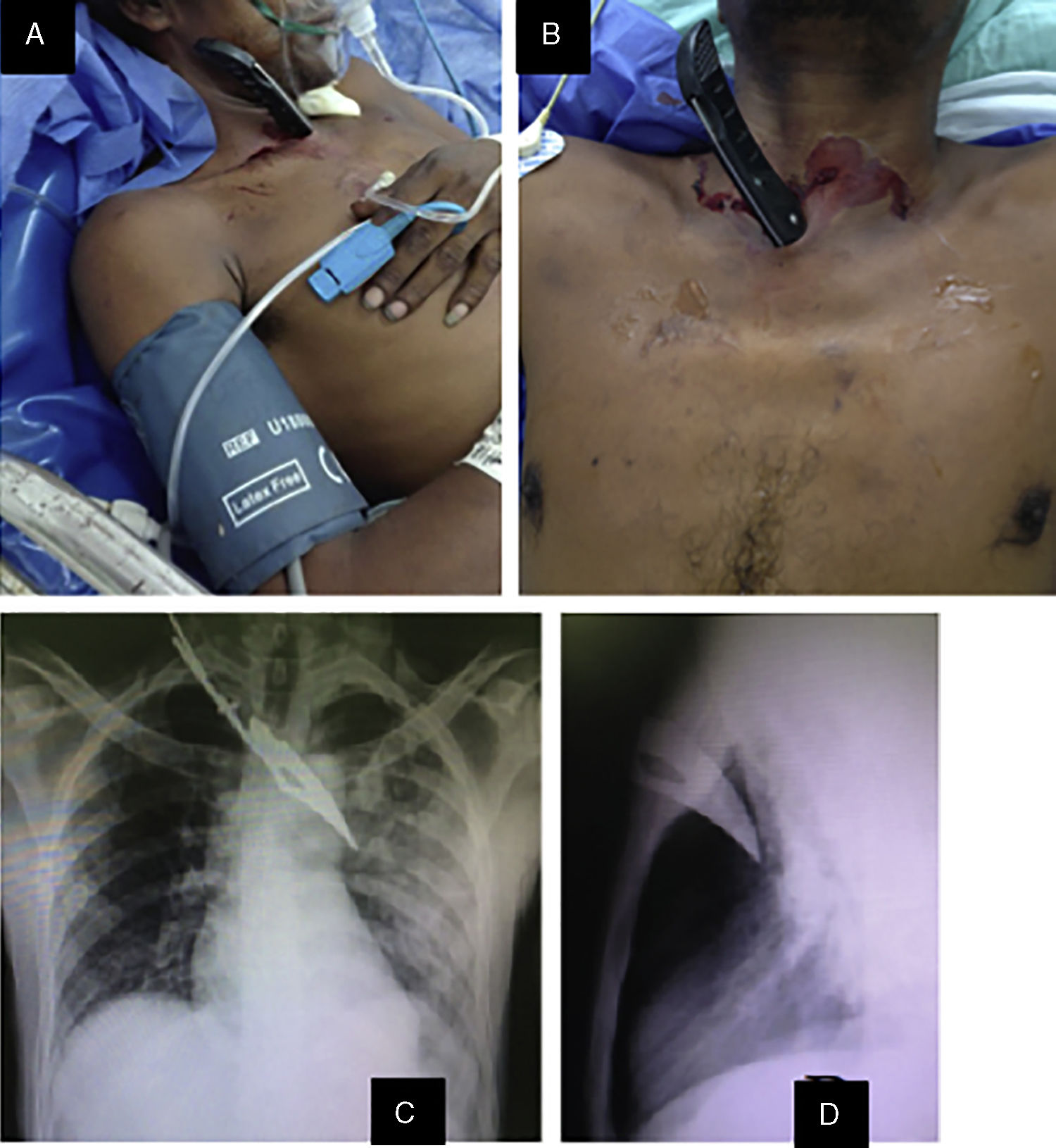
The patient is a 24-year-old man who uses marijuana and bazuco (coca paste) and had a previous laparotomy due to a gunshot wound (no report of this injury was available) and enucleation of the right eye due to a trauma injury. He was brought to our hospital by ambulance because of stab wound in the thoracic operculum. Upon arrival, the patient presented a permeable airway, tachypnea (24 breaths per minute), right tracheal deviation and diminished vesicular sounds in the left lung field. Blood pressure was 120/82mmHg and heart rate was 76 beats per minute, with a capillary filling time of 2s. The patient was alert, with a Glasgow score of 15/15 and no neurological deficit. When he arrived at the ER, the patient had a knife lodged immediately above the manubrium sterni with a left inferolateral vector but no signs of active bleeding (Fig. 1A and B). Posteroanterior and lateral chest radiographs showed the blade embedded in the thorax with an inferolateral vector toward the left thorax and left hemopneumothorax (Fig. 1C and D). After initial care, the patient received tetanus and antibiotic prophylaxis.
 Sharp object embedded at the stabbing site, immediately left of the manubrium sterni (lateral view); (B) anterior view; (C) posteroanterior chest radiograph showing left hydropneumothorax and the sharp object embedded in the left hemithorax; (D) lateral radiograph of the thorax, where the object seems not to have reached any vital structures.")
(A) Sharp object embedded at the stabbing site, immediately left of the manubrium sterni (lateral view); (B) anterior view; (C) posteroanterior chest radiograph showing left hydropneumothorax and the sharp object embedded in the left hemithorax; (D) lateral radiograph of the thorax, where the object seems not to have reached any vital structures.
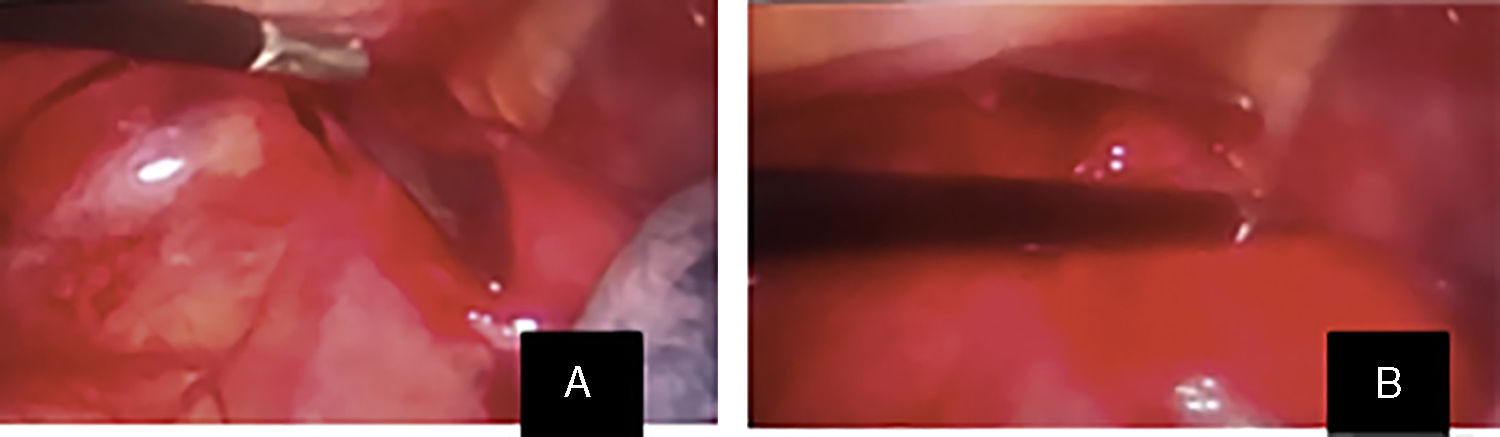
Given the hemodynamic stability of the patient, we decided to carry out an exploratory thoracoscopy. With the patient in the supine position, a 10mm incision was made in the fifth intercostal space on the left anterior axillary line, where a trocar was inserted for the camera, and a second 6mm incision was made on the left clavicular midline in the fifth intercostal space, where a trocar and clamp were inserted. Carbon dioxide insufflation was established and maintained at a pressure of 6mmHg in the pleural cavity. Surgical findings included a sharp 15-cm blade embedded in the left thorax, penetrating the sternal notch immediately medial to the subclavian artery, as well as a coagulated hemothorax of some 500cm3 (Fig. 2).
 15-cm sharp object lodged in the left thorax, penetrating through the sternal notch immediately medial to the subclavian artery; (B) blood clot of 500cm3.")
During surgery, the material needed to carry out urgent sternotomy and vascular control of large vessels was prepared, and the extraction of the foreign object was done safely under direct vision to avoid the risk of injury to the large vessels. The blood clots were suctioned, and the pleural cavity was flushed with 1000cm3 of saline solution. The site was checked and no other injuries were found; correct hemostasis was confirmed and a French 28 intrathoracic tube was left in place.
After surgery, the patient was transferred to the surgery floor. Forty-eight hours after surgery, the patient was eupneic and had good pulmonary ventilation with an expanded lung on the postoperative chest radiography, so the intrathoracic tube was removed and the patient was discharged.
Impalement injuries in the thorax are rare, as most patients with these injuries die at the site of the event.2 Their treatment is very complex. In general terms, patients should be treated in accordance with the basic principles of multiple-trauma patient management.
Upon arrival to the emergency room, if the patient is in a situation of hemodynamic instability, the treatment should be immediate surgery. In patients who are hemodynamically normal, chest radiography with two projections (posteroanterior and lateral) can be useful to determine the trajectory of the object. If we want to expand the study, CT angiography could be used, although with admitted limitations due to the artifacted image caused by the impaled object.1,3
When considering the removal of the object, it is important to bear in mind that the object may have penetrated several cavities and anatomical regions. Therefore, they should never be removed in the emergency room, as possible vascular injuries may be blocked by the object itself and withdrawal must always be carried out in the operating room.4,5
The thoracic outlet is an anatomical region through which important structures run, such as the brachiocephalic trunk, subclavian artery, trachea and esophagus. The classic approach is sternotomy,1 with additional cervical or supraclavicular extension when necessary.
The minimally invasive approach using thoracoscopy seems to be a reasonable and safe option in hemodynamically stable patients with thoracic impalement.6 This technique has important advantages, since it provides complete exploration of the thoracic cavity in order to evaluate other possible injuries and to evacuate clots, reduces postoperative pain, allows for early respiratory recovery and reduces hospital stay.7–9
Thoracoscopy can be a valid surgical approach in trauma injuries to the thoracic outlet in hemodynamically stable patients. It has been shown to be a useful alternative when safely extracting a sharp object lodged in the thoracic cavity.4
Please cite this article as: Durán Muñoz-Cruzado VM, Peñuela Arredondo JD, Meneses Freitte IA, Gonzálaez Haddad A, Herrera Tobon MA. Toracoscopia como alternativa a esternotomía en herida por empalamiento en opérculo torácico en paciente hemodinámicamente estable. Cir Esp. 2019;97:414–416.
