




To analyze obesity, level of adherence to the Mediterranean diet, physical activity and body dissatisfaction in people aged 16–50 years in the Region of Murcia, Spain.
MethodDescriptive and cross-sectional study. A total of 85 people (58 men) aged 16–50 years (28.68 ± 8.846) from 3 sports centers with similar sociodemographic characteristics participated in the study. Anthropometric values were recorded. They were tested for adherence to the Mediterranean diet, International Physical Activity Questionnaire (IPAQ) and test for dissatisfaction with their body (BSQ) and it was statistically related.
ResultsIt can be seen that the level of physical activity of both men and women is low, according to the IPAQ questionnaire, the men presented a METs/min per week of 3687.9 (DT = 3137.2) significantly higher than women’s.
In body dissatisfaction we see that women’s concern with their bodies (59.3%) is greater than men’s (31%), with a statistically significant difference (p = 0.013). Eating habits and BMI do not have statistically significant differences according to sex.
When applying the Mediterranean diet adherence test, it is observed that 95.3% of those with weight overload have a medium or low score, and only 4.7% have a discharge score (p = 0.128).
Those with weight overload have a score of 2935.73 MET/min per week (DT = 2633.16) and those without weight overload have a value of 3826.73 (DT = 3164.93, p = 0.268). There are significant differences regarding the values of body dissatisfaction. The level of concern of those with weight overload is 53.5%, compared to those without weight overload who have a level of concern of 26.2% (p = 0.014).
ConclusionsWeight overload is associated with body dissatisfaction and a low score in the test of adherence to the Mediterranean diet in people aged 16–50 years. The concern about body image in women was 59.3%.
Analizar la obesidad, adherencia a la dieta mediterránea, actividad física e insatisfacción corporal en personas de 16 a 50 años de la Región de Murcia.
MetodoEstudio descriptivo y transversal. Se incluyó a 85 personas (58 hombres) de 16 a 50 años de 3 centros deportivos con características sociodemográficas homogéneas. Se registraron los valores antropométricos. Posteriormente se les pasó un test de adherencia a la dieta mediterránea, el cuestionario internacional de actividad física (IPAQ) y el test de insatisfacción con su cuerpo (BSQ) y se relacionaron estadísticamente.
ResultadosSe puede observar que el nivel de actividad física tanto de hombres como de mujeres es bajo, según el cuestionario IPAQ. Los hombres presentaron un MET/min semanales de 3.687,9 (DE = 3.137,2) significativamente superior al de las mujeres.
En la insatisfacción corporal vemos que la preocupación de las mujeres con su cuerpo, 59,3%, es mayor que la que tienen los hombres, 31%, con diferencia estadísticamente significativa (p = 0,013). Los hábitos alimenticios y el IMC no tienen diferencias significativamente estadísticas en función del sexo.
Al aplicar el test de adherencia a la dieta mediterránea se observa que el 95,3% de los que tienen sobrecarga ponderal tiene una puntuación media/baja, y solo el 4,7% tiene una puntuación alta (p = 0,128). La puntuación de los que tienen sobrecarga ponderal tienen es de 2.935,73 MET/min semanales (DE = 2.633,16) y la de los que no tienen sobrecarga ponderal es de 3.826,73 (DE = 3.164,93; p = 0,268). Hay diferencias significativas con respecto a los valores de insatisfacción corporal. El nivel de preocupación de los que tienen sobrecarga ponderal es de 53,5%, respecto a los que no la tienen, cuyo nivel de preocupación es del 26,2% (p = 0,014).
ConclusionesLa sobrecarga ponderal se asocia con una insatisfacción corporal y una baja puntuación en el test de adherencia a la dieta mediterránea en personas de 16 a 50 años. La preocupación por la imagen corporal en las mujeres fue del 59,3%.
Obesity is considered the epidemic of the 21st century by the World Health Organization, affecting all ages, all social groups, and all countries.1 Despite decades of struggle against this epidemic, which represents a major threat to public health, the sharp increase in obesity in childhood and adolescence is one of this century’s greatest public health challenges.2 Each year, 3.4 million people die from this and associated diseases. In recent decades we have seen a significant increase in their prevalence, which tripled between 1975 and 2016.1
It is a chronic disease of multifactorial origin that is associated with potentially serious complications and requires a multidisciplinary approach due to its high clinical impact and costs of the medical care it requires.2 Hereditary factors seem to be the cause of 30%–50% of variation in adiposity; however, individual genetic defects and the syndromes associated with obesity represent less than 1% of childhood obesity.3 Therefore, we can conclude that the rapid increase in obesity rates must be attributed to recent changes that have led, on the one hand, to lifestyle changes, with different eating habits and a progressive decrease in physical activity and, on the other, to the increased availability of food, particularly with a high calorie content. This reinforces the concept of multifactorial disease, involving environmental factors closely related to underlying genetic risk factors.
Metabolic syndrome, bearing in mind that obesity is its most frequent feature, is the main cause of cardiovascular disease and therefore of morbidity and mortality in advanced countries. Moreover, half of adults with type 2 diabetes mellitus are obese,4,5 with a body mass index (BMI) ≥30 kg/m2.
It should be noted that most epidemiological studies observe large geographical differences in cardiovascular disease incidence rates. If we compare northern European countries and the United States with the countries of southern Europe, such as France, Spain, Greece and Italy, there is a low incidence of coronary diseases in the latter. The Mediterranean diet has been the most important factor in explaining this difference.6
People’s diets seem to directly affect adiposity and therefore the risk of obesity and the diseases with which it is correlated. Most of the few studies that currently link diet with obesity conclude that following a traditional Mediterranean diet is inversely associated with the risk of obesity or weight gain.7
It should be noted that, just as eating habits have positive effects on health, physical activity also has fundamental implications for health. Physical activity is an effective strategy in the primary and secondary prevention of chronic diseases. There is evidence that it improves the functioning of the cardiorespiratory, digestive, and endocrine systems, that it strengthens the musculoskeletal system, decreases serum cholesterol and triglyceride levels, obesity, and adiposity, and is also closely related to better mental health.8
Current guidelines recommend that adults undertake at least 150 min per week of moderate or 75 min per week of vigorous aerobic physical activity. Despite the benefits of physical activity, so intricately linked to the reduction of obesity and adherence to the Mediterranean diet, just over half of adults comply with these recommendations. There are still barriers to physical activity such as lack of time, low motivation or ‘lack of energy’9 and barriers in young people reflecting the increasingly sedentary behaviour of children and adolescents, especially in passive screen-based leisure activities.1
There are various methods to assess levels of physical activity. However, the most validated and reliable methods to study an individual’s physical activity are difficult to apply due to their high cost and methodological difficulty. An alternative is the physical activity questionnaires, such as the International Physical Activity Questionnaire (IPAQ), which is easy to complete and does not alter the person’s behaviour.10
The PREDIMED study (Prevention with Mediterranean diet), which is a well-known field trial aimed at the primary prevention of chronic diseases through the Mediterranean diet, enables us to assess how this dietary pattern can counteract the adverse effects of abdominal obesity and thus reduce the risk of cardiovascular events.11 But modifying a diet not only requires a great deal of collaboration from the patient, but also from their environment, with easy access to certain products and willingness to buy and cook food according to the dietary plan. In addition, measuring adherence to the diet involves greater effort on the part of both the participant and the investigator. The enormous diversity of eating habits, basal metabolic status and nutritional and dietary goals are limitations for comparisons between studies conducted in different contexts.6–13
Obesity and therefore high BMI are described as factors directly associated with dissatisfaction with one’s body. Slimmer people show more positive perception of their bodies, while overweight people show more dissatisfaction.14,15 While body image refers to the way one perceives, imagines, feels, and acts towards one’s own body, when a person feels dissatisfied with that image, they tend to dislike their appearance and worry excessively about their bodies. Besides the affective and cognitive aspects, there are also perceptive aspects to this dissatisfaction, which influence body assessment. A person who is dissatisfied with their body tends to hide it, subject it to extreme diets and exercise, and avoid social situations where they subject to other people’s gaze.16
Knowing the groups at risk, with their differences in weight, and studying dissatisfaction with body image facilitates the design of prevention programmes to help acceptance of the body and shape healthy eating habits that are not harmful and do not complicate existing health problems. This will also enable an understanding of the behavioural patterns of physical activity.16 This idea alerts us to the population of young adolescents, as they are an intermediate group between the populations that identify as being at risk of obesity and are vulnerable to developing greater dissatisfaction with the natural physical changes taking place at this age.
Finally, we should highlight that there are few data and studies in the Region of Murcia, yet almost all support the fact that the level of physical activity is low (3–3.5 h/week) and that the calorie profile of the diet is notably far from that recommended for a balanced diet.17 All this serves to explain why the Region of Murcia has one of the highest standardized mortality rates for ischaemic heart disease and cerebrovascular disease among the Spanish Autonomous Communities, not to mention its higher rate of smoking among men compared to other communities.18 This study was set up on these premises, with the aim of analysing the relationship between obesity and adherence to the Mediterranean diet and physical activity in our region. As a secondary objective, we set out to assess acceptance of body image.
MethodDesign and participantsA descriptive and cross-sectional study was carried out. A total of 85 people (58 men and 27 women) aged 16–50 (28.68 ± 8.8) from 3 sports centres in the Region of Murcia (Spain) with similar socio-demographic characteristics participated in the study. To this end, the sample was selected by non-probabilistic sampling. Although we used this type of sampling, all the people selected were invited to participate.
Three centres were selected in different, representative areas of Murcia with homogeneous sociodemographic characteristics. Assuming a 21% prevalence of obesity in each centre and a .05 error, an approximate sample of 23 people per centre was calculated.
These individuals were informed beforehand about the purpose of the study and the nature of the tests through an information document. Both the anthropometric measurements and the questionnaires were carried out on any given day before starting the training session.
ProceduresAnthropometric measurementsThe height of the participants was measured using a portable height measure with an accuracy of .1 cm (Leicester Tanita HR001, Tokyo, Japan). The measurement was taken with the participants standing upright, barefoot and wearing light clothing (underwear or similar), with the heels, buttocks, and upper middle back in contact with the vertical axis of the measure, arms extended parallel to the body, i.e., hanging down by sides with palms facing the thighs, and heels together forming a 45° angle, and head positioned in the horizontal Frankfurt plane (horizontal plane nose-tragus). The body weight of the subjects was measured using an electronic scale (with an accuracy of .1 kg) (Tanita BC-545, Tokyo, Japan). The measurement was taken with the subject standing in the centre of the scale in a standard upright position, barefoot and wearing light clothing (underwear or similar), and with their back to the measurement recorder, and their body not touching anything around them.12 The BMI was calculated from the body weight (kg) divided by height in meters squared (m2) of the participants. Furthermore, the BMI was determined using the age and sex-specific thresholds of the World Health Organisation, with 4 categories: underweight (BMI < 18.5 kg/m2); normal weight (BMI = 18.5–24.9 kg/m2); overweight (BMI = 25.0–29.9 kg/m2) and obesity (BMI ≥ 30.0 kg/m2).12 The subjects were then categorised into those who were overweight (overweight + obesity) and those who were not (normal weight + underweight).
Prevention with the Mediterranean diet (PREDIMED)This is a questionnaire on adherence to the Mediterranean diet from the PREDIMED study (MeDiet-PREDIMED). The PREDIMED test is a short dietary assessment tool comprising a set of 14 short questions to provide information on adherence to the Mediterranean diet. It takes the form of a face-to-face interview with the participant. The 14-item tool was developed in a Spanish case-control study of myocardial infarction, in which the best cut-off points were selected to discriminate between cases and controls for each food or food group. In this first step, 9 of the 14 items were obtained. Five elements were added later, considered particularly relevant in assessing adherence to the traditional Mediterranean diet.7 There are 14 direct questions on the consumption of the main foods in the Mediterranean diet: olive oil, fruits, vegetables, pulses, fish, nuts, moderate consumption of wine and white meat, and low consumption of red and processed meat. The scores are grouped together into 4 categories: high adherence: 12–14 points; medium adherence: 8–11.99 points; low adherence: 0–7.99 points.19
International Physical Activity Questionnaire (IPAQ (MET-min per week)The short version of the IPAQ is an instrument that evaluates the frequency (days), duration (time per day) and intensity (moderate, vigorous physical activity, walking) of physical activity in a week. Physical activity was described in terms of MET, which refers to the metabolic equivalent in which 1 MET is the rate of energy expenditure while at rest, sitting. MET-minute per week is the product of the number of METs multiplied by the minutes of activity per day, multiplied by the days of the week (MET × min of activity/day × days of the week). The population’s physical activity levels were classified as high, moderate, and low considering the intensity of aerobic physical activity, on an absolute scale, classified as mild intensity physical activity (performed at 1.1–2.9 times the intensity at rest: 1.1–2.9 MET), moderate intensity (3–5.9 MET) and vigorous intensity (6 or more MET). Therefore, low physical activity level (not reporting any type of physical activity or reporting some activity, but not sufficient to meet the criteria for moderate and high levels); moderate physical activity level (any of the following 3 criteria: 3 or more days of vigorous physical activity of at least 20 min per day, 5 or more days of moderate or vigorous physical activity or walking at least 30 min per day and 5 or more days of any combination of walking, moderate or vigorous physical activity with a minimum of 600 MET-min per week); high physical activity level (any of the following 2 criteria: vigorous physical activity on at least 3 days, accumulating a minimum of 1500 MET-minute per week and 7 or more days of any combination of walking, moderate or intense physical activity, accumulating a minimum of 3000 MET-min per week.13
Body Shape QuestionnaireThe Body Shape Questionnaire (BSQ) was used to evaluate body dissatisfaction. It is a self-administered questionnaire consisting of 34 items that are assessed using the following scale (1 = never, 2 = rarely, 3 = at times, 4 = often, 5 = very often, 6 = always), thus the test range is 34–204 points.
Five factors are assessed by the Spanish version: BSQ 1, concern about weight; BSQ 2, concern about the unsightly aspects of obesity; BSQ 3, dissatisfaction and general body concern; BSQ 4, dissatisfaction with the lower body and BSQ 5, use of vomiting or laxatives to reduce dissatisfaction. Based on the total score, 4 categories or levels of concern due to body dissatisfaction are established: no concern (score <80), mild concern (between 81 and 110), moderate concern (between 111 and 140) and extreme concern (>141 points).20
Statistical analysisMeans and standard deviation (SD) are reported for all quantitative variables, and frequencies and percentages (%) are presented for all qualitative variables. The normality of the data was checked using a Kolmogorov–Smirnov test with Lilliefors’ correction, and the homogeneity of the variations was checked using a Levene’s test.
The χ2 test was used to contrast the proportions between qualitative variables. The Student’s t-test was used to compare the quantitative variables of 2 groups, depending on whether the assumption of normality was met. The correlations were determined by Pearson's correlation coefficient. In addition, a binary logistic regression was calculated to predict the probability of obtaining different results depending on the BMI category. A p < .05 was considered statistically significant.
SPSS software (IBM Corp., Armonk, NY, USA) for Windows (version 24.0) and the Excel 2016 database (MicrosoftCorp, Redmond, WA, USA) were used for the data analysis.
Ethical aspectsThe study was submitted to the Research Commission of the University of Castilla La Mancha and was agreed. The study was carried out in accordance with recognised ethical standards and best clinical practice. The data was protected from uses not permitted by persons unconnected with the research and the confidentiality of personal data protection and Law 41/2002 of 14 November, the basic law regulating patient autonomy and rights and obligations in the field of clinical information and documentation, was respected. Therefore, the information generated in this study was considered strictly confidential for the participating parties.
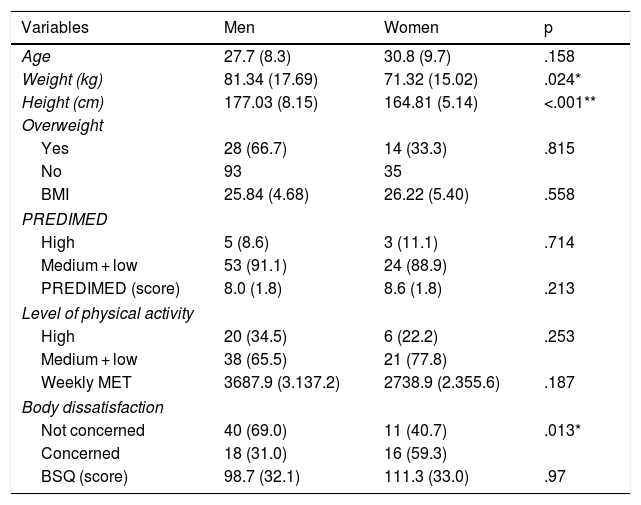
ResultsComparison of variables by sex and level of overweightTable 1 (differences by sex) shows the following data:
Comparison of variables by sex.
| Variables | Men | Women | p |
|---|---|---|---|
| Age | 27.7 (8.3) | 30.8 (9.7) | .158 |
| Weight (kg) | 81.34 (17.69) | 71.32 (15.02) | .024* |
| Height (cm) | 177.03 (8.15) | 164.81 (5.14) | <.001** |
| Overweight | |||
| Yes | 28 (66.7) | 14 (33.3) | .815 |
| No | 93 | 35 | |
| BMI | 25.84 (4.68) | 26.22 (5.40) | .558 |
| PREDIMED | |||
| High | 5 (8.6) | 3 (11.1) | .714 |
| Medium + low | 53 (91.1) | 24 (88.9) | |
| PREDIMED (score) | 8.0 (1.8) | 8.6 (1.8) | .213 |
| Level of physical activity | |||
| High | 20 (34.5) | 6 (22.2) | .253 |
| Medium + low | 38 (65.5) | 21 (77.8) | |
| Weekly MET | 3687.9 (3.137.2) | 2738.9 (2.355.6) | .187 |
| Body dissatisfaction | |||
| Not concerned | 40 (69.0) | 11 (40.7) | .013* |
| Concerned | 18 (31.0) | 16 (59.3) | |
| BSQ (score) | 98.7 (32.1) | 111.3 (33.0) | .97 |
Regarding physical activity, both the men and the women have a low level of activity according to the IPAQ questionnaire, however, it should be noted that the men showed a weekly MET-min of 3687.9 (SD = 3137.2) and the women showed a MET-min of 2738.9 (SD = 2355.6; p = .187).
In terms of body dissatisfaction, we see that the women’s concern with their body (59.3%) is greater than that of the men (31%), with a statistically significant difference (p = .013).
We did not find any statistically significant differences according to sex in eating habits and BMI.
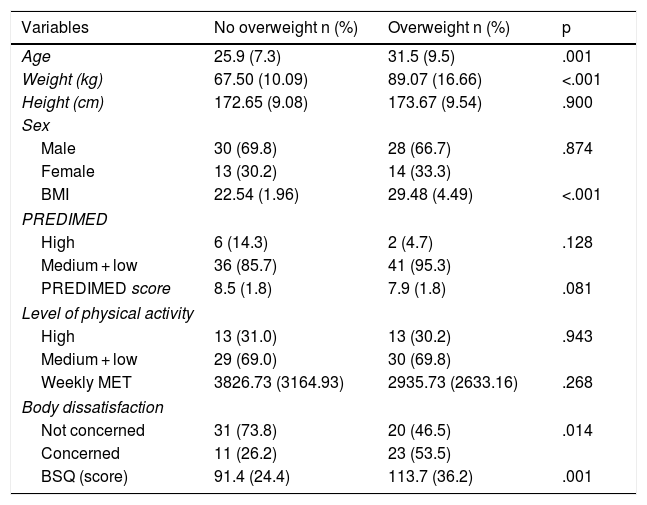
Table 2 (differentiating individuals who are overweight from those who are not) shows:
Comparison of variables according to level of overweight.
| Variables | No overweight n (%) | Overweight n (%) | p |
|---|---|---|---|
| Age | 25.9 (7.3) | 31.5 (9.5) | .001 |
| Weight (kg) | 67.50 (10.09) | 89.07 (16.66) | <.001 |
| Height (cm) | 172.65 (9.08) | 173.67 (9.54) | .900 |
| Sex | |||
| Male | 30 (69.8) | 28 (66.7) | .874 |
| Female | 13 (30.2) | 14 (33.3) | |
| BMI | 22.54 (1.96) | 29.48 (4.49) | <.001 |
| PREDIMED | |||
| High | 6 (14.3) | 2 (4.7) | .128 |
| Medium + low | 36 (85.7) | 41 (95.3) | |
| PREDIMED score | 8.5 (1.8) | 7.9 (1.8) | .081 |
| Level of physical activity | |||
| High | 13 (31.0) | 13 (30.2) | .943 |
| Medium + low | 29 (69.0) | 30 (69.8) | |
| Weekly MET | 3826.73 (3164.93) | 2935.73 (2633.16) | .268 |
| Body dissatisfaction | |||
| Not concerned | 31 (73.8) | 20 (46.5) | .014 |
| Concerned | 11 (26.2) | 23 (53.5) | |
| BSQ (score) | 91.4 (24.4) | 113.7 (36.2) | .001 |
There are no significant differences between the men and the women (p = .874).
According to PREDIMED, it is observed that 95.3% of the participants with overweight have a medium/low score and only 4.7% have a high score (p = .128).
In terms of physical activity undertaken (MET-min per week), those with overweight achieved a score of 2935.73 (SD = 2633.16) and those without overweight 3826.73 (SD = 3164.93; p = .268).
Finally, it should be noted that there are significant differences with respect to body dissatisfaction. The level of concern of those with overweight is 53.5% and that of those without is 26.2% (p = .014).
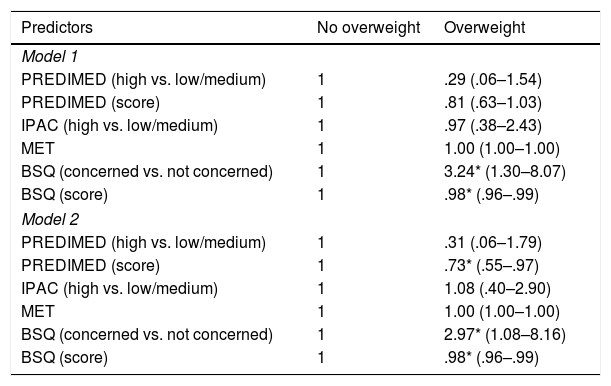
Association between variables and level of overweightA logistic regression is given in Table 3, which expresses the level of association between those with and without overweight with the continuous quantitative variables PREDIMED, IPAQ (MET-min per week) and the BSQ. For this purpose, the Table is divided into Model 1 and Model 2, which unlike Model 1, is adjusted by sex and age.
- -
In model 1, PREDIMED indicates that those with overweight have a 71% lower likelihood of obtaining a high PREDIMED score. What is characteristic of Model 1 is that those with overweight are three times more likely to express concern about their physical condition (324%).
- -
Model 2 shows that there is a clear association between the PREDIMED score and overweight individuals. In other words, there is a lower likelihood of obtaining higher PREDIMED scores in subjects who are overweight (OR = .73; 95% CI: .55–.97).
- -
It is also observed that there is a 297% greater likelihood that those who are concerned with their physical condition are overweight, with a lower likelihood of obtaining lower scores on the BSQ (OR = .98; 95% CI: .96–.99).
Binary logistic regression according to level of overweight.
| Predictors | No overweight | Overweight |
|---|---|---|
| Model 1 | ||
| PREDIMED (high vs. low/medium) | 1 | .29 (.06–1.54) |
| PREDIMED (score) | 1 | .81 (.63–1.03) |
| IPAC (high vs. low/medium) | 1 | .97 (.38–2.43) |
| MET | 1 | 1.00 (1.00–1.00) |
| BSQ (concerned vs. not concerned) | 1 | 3.24* (1.30–8.07) |
| BSQ (score) | 1 | .98* (.96–.99) |
| Model 2 | ||
| PREDIMED (high vs. low/medium) | 1 | .31 (.06–1.79) |
| PREDIMED (score) | 1 | .73* (.55–.97) |
| IPAC (high vs. low/medium) | 1 | 1.08 (.40–2.90) |
| MET | 1 | 1.00 (1.00–1.00) |
| BSQ (concerned vs. not concerned) | 1 | 2.97* (1.08–8.16) |
| BSQ (score) | 1 | .98* (.96–.99) |
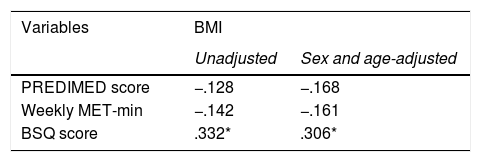
A correlation using Pearson’s r coefficient is shown in Table 4 and only a strong association between BMI and BSQ score is observed. However, the correlation study revealed that BMI negatively correlated with the PREDIMED and the level of physical activity (MET-min per week).
DiscussionThis study attempts to describe, compare, and establish the level of association between BMI and level of adherence to the Mediterranean diet, physical activity and body dissatisfaction in people aged between 16 and 50 in the Region of Murcia, according to sex.
The main results of this study indicate that people with overweight tend to have greater body dissatisfaction, especially women, and there is a lower level of physical activity in both men and women. It should be noted that the men had a higher metabolic equivalent score (higher physical activity) than the women. Overweight was also associated with a lower PREDIMED score, i.e., poorer adherence to the Mediterranean diet. Similarly, participants classified as overweight were more likely to show a lower PREDIMED score and higher BSQ score compared to participants classified as not overweight.
The relationship of BMI with adherence to the Mediterranean diet is interesting, assessed using only a short 14-item questionnaire, which is less time consuming, less costly and requires less collaboration from participants than more comprehensive methods such as the Food Frequency Questionnaire.7 And with only 14 items reporting on the diet quality of each individual, the improvement of cardiovascular risk factors is demonstrated, which is directly related to HDL cholesterol and inversely to BMI (reduction of abdominal and visceral adiposity), serum triglycerides and fasting glucose (improvements in sensitivity and reduction of insulin), according to other studies.7 Other aspects studied in different articles also show that the Mediterranean diet reduces some biomarkers of inflammation, oxidative stress, postprandial inflammation, as well as other mechanisms associated with abdominal fat deposit. In our study, no significant differences in diet between women and men were found, however, in most studies there are also usually no significant differences in dietary pattern with respect to sex.2 In short, worth highlighting is the beneficial effect on the risk of metabolic syndrome with the measurement of only 14 items.7 However, unlike the studies mentioned above, no data on different biochemical parameters (glucose, cholesterol, etc.) were analysed in our study.
Geographical location is a factor that helps obtain significant scores in PREDIMED, since, as a Mediterranean country, we follow a “more Mediterranean” diet than Nordic countries.2
As we have mentioned, the concepts of healthy eating and physical activity are related, and those who eat healthy foods can be shown to be more likely to be physically active and less sedentary than those who eat less healthy foods. The conclusion is that having healthy eating habits is an indicator for adopting a more active lifestyle.21
We can confirm that in our study the men had a higher level of physical activity than the women, without high statistical significance; however, other studies do conclude a high level of statistical significance in this aspect.1 This may be because some traditional socio-cultural factors currently seem to play a major role, such as the view that women are physically weaker and that physical activity or sport is related to strength and, therefore, not common practice among women. In addition, women assess their sports skills less well, and therefore are also likely to participate less in sports.1
As we observed, in our study overweight people usually have a low level of physical activity, but its statistical significance is quite low. However, in other studies a statistically significant level has been obtained for this aspect. That is, a reduction in BMI with physical activity and therefore also an improvement in cardiovascular risk factors.14 Furthermore, several studies detail a wide and heterogeneous number of benefits, outside the cardiovascular area. Planned, aerobic and constant exercise favours an increase in skeletal muscle fibres, mainly oxidative type IIA fibres; it also increases insulin sensitivity and glucose uptake through the non-insulin-dependent translocation of glut4, increases the activity of the AMPK enzyme (AMP-activated protein kinase), which increases glucose uptake from muscle through non-insulin-dependent pathways, improves the cardiorespiratory profile and increases synthesis of lipoprotein lipase (protein of lipoprotein and lipid metabolism). It also improves low-grade inflammation in obese patients and has been shown to induce a genetic profile that degrades glucose more efficiently, as well as circulating lipids.14
Similarly, people who are more physically active may want to improve their performance by choosing a better diet, or even the simple fact that more physical activity requires more energy may have an impact.21
As in other studies, to avoid overestimation in the IPAQ questionnaire, in our study we also analysed physical activity quantified in MET-min per week.
However, the most relevant and statistically significant data of the study is body dissatisfaction and overweight, especially in women. It is interesting that this dissatisfaction is found in overweight groups and not only in underweight groups, which have been frequently associated with eating and body image disorders (anorexia and bulimia),16 and with depression and low self-esteem. Therefore, it is important to prevent or treat body dissatisfaction.20 In our study, as in others, statistically significant differences appear, since body dissatisfaction is related to negative attitudes towards the body, including factors such as negative perception of body size and loss of familiarity with one’s own body, as a factor of body dissatisfaction, since today’s ideal is to be slim.16 This trend is led by the media and social pressure, and mainly affects women who are concerned about their weight and bodies.20
As mentioned, women are more vulnerable to body dissatisfaction and their poorer physical and emotional self-perception is remarkable. This dissatisfaction should be studied in relation to low self-esteem and affective disorders, as there is evidence of the presence of depression and anxiety in overweight women. However, even so, it is noteworthy that women are the most vulnerable group due to their low body image (linked with the perception of their body) as well as their perceived poor physical ability.16
Given that education is the foundation of many personal values in childhood and adolescence, we propose adopting the recommendations on diet and physical activity outlined by Simovska et al. and to promote a diet based on nutritional recommendations in schools. As lines of action, it would be advisable to programme activities of a preventive and multimodal nature at community level, to ensure appropriate outdoor infrastructures for the promotion of physical activity, to design specific strategies to encourage exercise among girls and disadvantaged groups and to seek the help of specialist professionals.1
Our study has the advantage that its participants go to sports centres to exercise to lose weight and improve their body appearance, and similarities can be found with the PREDIMED-Plus study,22 in which changes in diet and physical activity went in the expected direction, with significant improvements. After 12 months, participants in the intervention group lost an average of 3.2 vs. .7 kg in the non-intervention group (p < .001), with a mean difference of −2.5 kg (95% CI: −3.1 to −1.9). Weight loss ≥5% occurred in 33.7% of participants with the intervention compared to 11.9% without the intervention (p < .001). Similarly, cardiovascular risk factors, including waist circumference, fasting glucose, triglycerides, and HDL cholesterol, were significantly improved (p < .002). Therefore, the PREDIMED-Plus intensive lifestyle intervention for 12 months was effective in reducing adiposity and improving cardiovascular risk factors in overweight or obese older adults with metabolic syndrome, as well as in people with diabetes or at risk of developing diabetes.
Therefore, in this line marked by PREDIMED-Plus, we must educate about physical activity and diet. Specialists refer to the importance of addressing groups with body dissatisfaction, considering the medical implications of risk to health, who therefore require timely psychological care.16 In our research study, when analysing the factors related to body dissatisfaction, an educational activity for women could be to seek healthy body measurements and change their BMI.
This study presents certain limitations that need to be explained. First, due to its cross-sectional design, it cannot be concluded that the observed relationships reflect causal relationships. Secondly, although the PREDIMED index is an instrument used to determine adherence to the Mediterranean diet, information on the frequency of consumption of certain foods characteristic of the Mediterranean diet could be interesting. Thirdly, although we use validated physical activity questionnaires, we do not use accelerometer devices, which would have provided a more accurate assessment of the level of physical activity and sedentary behaviour. Finally, BMI is another confounding factor in the study worth mentioning, as the analysis of overweight with BMI does not tell us whether excess body mass is fat or muscle.
To conclude, we were able to make the assessment that overweight is associated with body dissatisfaction and a low PREDIMED score (Mediterranean diet adherence test) in people aged 16–50 in the Region of Murcia who participated in this study. In addition, it was found that the women’s concerns about their body were greater than those of the men (59.3 vs. 31%). The authors highlight that awareness campaigns are also needed to warn of the adverse health effects of inappropriate eating habits and low levels of physical activity. At the same time, more prospective cohort studies are needed to better clarify the relationship between adherence to the Mediterranean diet, physical activity, and other health-related parameters.
FundingNo funding.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Guillén Alcolea F, López-Gil JF, Tárraga López PJ. Adherencia a la dieta mediterránea, nivel de actividad física e insatisfacción corporal en sujetos de 16 a 50 años de la Región de Murcia. Clin Investig Arterioscler. 2021;33:10–18.