

Inner speech is a familiar experience for us but, in general, few systematic studies have been done on the subject. Recent studies have included this phenomenon in the development of auditory hallucinations. The purpose of this article is to propose and validate the Spanish version of the Varieties of Inner Speech Questionnaire (VISQ), to which we have added a new factor called Dialogues with Self-Positions in Inner Speech. It is further intended to test the relationship between this scale, dissociation, and proneness to hallucinations. For this purpose, 318 students completed the VISQ, plus a dissociation scale and another one for hallucination proneness. The results show the scale's good psychometric reliability and validity. Dissociation was found to mediate between the VISQ scale and hallucination proneness. The implications for hallucination models and future lines of research are discussed.
El habla interna [inner speech] es una experiencia familiar para nosotros pero que ha sido en general poco estudiada de manera sistemática. Recientes estudios han incluido este fenómeno en el desarrollo de las alucinaciones auditivas. En el presente artículo se pretende revisar y validar la escala Varieties of Inner Speech Questionnaire (VISQ) en castellano, añadiendo además una quinta escala denominada Posiciones del Yo en el Lenguaje Interno. Además, se pretende comprobar la relación entre las diferentes escalas, la disociación y la propensión a las alucinaciones verbales. Para ello 318 estudiantes completaron la VISQ-R más una medida de disociación y otra de propensión a las alucinaciones. Los resultados muestran unas buenas propiedades psicométricas de fiabilidad y validez en la escala VISQ-R. Los modelos de mediación, por su parte, indican un papel de mediación de las medidas de disociación entre todas las escalas del VISQ-R menos el lenguaje interno dialógico y la propensión a las alucinaciones verbales. Se discuten las implicaciones para los modelos de las alucinaciones verbales y futuras líneas de investigación.
The phenomenon of inner speech is familiar to us all. It is a type of experience which constitutes and characterizes thought. When we think, we talk to ourselves. Plato, for example, in the Theaetetus (Plato, 1987), said that thought is “…a discourse that the mind carries on with itself” (Plato, 198e), so when people think, “they are just conversing and they themselves suggest the questions and answers, sometimes agreeing and others denying” (Plato, 190a).
Our own daily experience shows how internal speech is also present in the form of dialogue. When, for example, we think about a problem, we can take the point of view of another and we can anticipate an answer. After a meeting at work in which we participated actively, we may continue the discussion in our minds and imagine answers we did not propose at the time. These are examples of how internal speech is present in our daily lives. Psychology research has also provided data about it. Since the pioneering work by Piaget (1962) and Vygotsky (1987) on egocentric speech, empirical studies have been done on inner speech and self-regulation (e.g., Fernyhough & Fradley, 2005), on their neurological correlates (e.g., Ehrich, 2006), and on inner speech impairments and auditory verbal hallucinations (Fernyhough, 2004). In all of them, the importance of inner speech as a mediator in psychological processes is emphasized. One common element in all those lines of research is understanding inner speech as talking silently to oneself. As such, it is a specific type of verbal practice which is far from the typical interaction between partners in a conversation, because in this case there is only one partner performing both the roles of speaker and listener at the same time.
As already emphasized by Vygotsky (1987), this particular way of talking to oneself has a dialogic quality. This author suggested that inner speech represents the end point of an evolutionary process in which external discourse is gradually internalized as a form of verbal thought. As demonstrated in other studies (e.g., Wertsch, 1980), inner speech reflects the dialogic structure of verbal interpersonal exchanges. Therefore, mental dialogue may be an internal version of interactions between perspectives that occur between individuals in the social world.
In this study we were interested in the important implications that the study of inner speech has for understanding auditory hallucinations. From this point of view, inner speech is understood to be the basis of auditory verbal hallucinations (AVHs). Recently, Perona-Garcelán, Pérez-Álvarez, García-Montes, and Cangas (2015), in the framework of the Dialogic Self Theory (Hermans, 2014), proposed that AVHs are in themselves dialogic experiences. From this viewpoint, the self is considered a complex experience made up of the interiorization of the values and perspectives of reality with which a person is confronted during his life. This author calls the interiorization of these perspectives self-positions (Hermans, 2014). The self, from this approach, is made up of all those self-positions which interact with each other from an integrated position which provides coherence to the person's psychological world.
In the proposal by Perona-Garcelán et al. (2015), the relationship a person maintains with his/her voices is the core facet of AVHs. For these authors, the voices in themselves have pragmatic, dialogic properties (Leudar, Thomas, McNally, & Glinski, 1997), and persons who have this type of experiences relate to their voices in a manner similar to what they do in their settings (Hayward, Berry, McCarthy-Jones, Strauss, & Thomas, 2013). From this perspective, AVHs are caused by the different self-positions that make up the person's self at any given time, becoming dissociated from each other in such a way that they are experienced as “significant others.” Therefore, the phenomenology of inner speech would provide body to the hallucinatory experience, in which inner dialogues among the self-positions would be experienced as voices.
In recent years several methods have been developed to study inner speech: questionnaires (Morin, Uttl, & Hamper, 2011) and experience sampling (Hurlburt, Heavey, & Kelsey, 2013). However, few have included any of Vygotsky's phenomenological characteristics, such as dialogicity, condensation, or the function of self-regulation of inner speech (Alderson-Day et al., 2014). The only questionnaire for this purpose is the Varieties of Inner Speech Questionnaire (VISQ) by McCarthy-Jones and Fernyhough (2011). The VISQ is a scale which measures inner speech in four dimensions: (i) dialogicity, the communicative and conversational quality of inner speech; (ii) condensation, or the extent to which inner speech is syntactically and semantically abbreviated; (iii) evaluative/motivational inner speech, such as saying “I should do this” to oneself; and (iv) the presence of other people's voices in inner speech. The English version shows good construct reliability and validity.
McCarthy-Jones and Fernyhough (2011) showed that the “evaluative/motivational inner speech” and “the presence of other people's voices in inner speech” factors were positively associated with anxiety. Proneness to Auditory Hallucinations was also positively correlated with Dialogic Inner Speech. In a later study, Alderson-Day et al. (2014), in a sample of healthy subjects, found that the VISQ factor “evaluative/motivational inner speech” was associated with low self-esteem and more frequent dissociative experiences. Using a structural equation model, they found that dissociation mediated between specific components of inner speech (evaluative and other people in inner speech) and proneness to auditory hallucinations.
The purposes of our study were first, to adapt the VISQ scale to Spanish, including another variety of inner speech which we call “Dialogue with self-positions in inner speech.” From our viewpoint, the VISQ defines the different factors that make it up depending on the person's relationship with himself. The “Dialogic Inner Speech” and “Evaluative/Motivational Inner Speech” factor items, for example, refer to the neutral dialogic relationship (in the first case) and affectively loaded dialogue (in the second) of the person with himself. But it does not include another form of inner dialogue: the person conversing with other people in his imagination, in which he takes the initiative. We think the VISQ factor which includes the presence of “Other people in Inner Speech” does not span the phenomenological characteristics of the type of variety of inner speech we are proposing. Careful reading of the items for this factor proposed by McCarthy-Jones and Fernyhough (2011) reveals that it does not express this relationship of dialogue with the “other inside”, but limits the person to listening passively to that other. This dimension is more like the one proposed by Hurlburt et al. (2013) called inner hearing.
In the second place, we systematically replicated the study by Alderson-Day et al. (2014) to examine the relationship of the various VISQ factors in the Spanish version, including this new factor, with dissociation and proneness to hallucinations in healthy subjects. Starting out from the model by Perona-Garcelán et al. (2015), we hypothesized that the dissociation variable mediates between the dialogic varieties of inner speech and hallucination proneness. However, this mediation will not occur in the relationship between condensed inner speech and hallucination proneness.
MethodParticipantsThe original sample was comprised of 318 students at the University of Seville School of Psychology. Participants were sent a request by e-mail to participate in the study, offering them an academic incentive for doing so. The answers were given anonymously, and students only filled in their sociodemographic data and an informed consent for participating in the study. In the end, 23 students were disqualified because they were foreign students or did not have a completely adequate understanding of the language, had been diagnosed with some mental health disorder, or had been prescribed psychopharmacological treatment at the time of the study. In the end, 295 participants remained, 233 women and 62 men, with a mean age of 21.7 (SD=4.7), a minimum age of 18, and maximum of 56.
InstrumentsVarieties of Inner Speech Questionnaire (VISQ; McCarthy-Jones & Fernyhough, 2011). The Varieties of Inner Speech Questionnaire is an 18-item self-report scale measuring four dimensions of inner speech. Participants endorse items about their experience of inner speech in relation to dialogicity (“I talk back and forward to myself in my mind about things”), evaluative and motivational characteristics (“I talk silently to myself telling myself not to do things”), condensation (“I think to myself in words using brief phrases and single words rather than full sentences”), and the presence of other voices (“I experience the voices of other people asking questions in my head”). Answers are on a 6-point Likert scale ranging from certainly does not apply to me (1) to certainly applies to me (6). Each subscale of the VISQ has high internal consistence (Cronbach's α>.80) and moderate to high test–retest reliability (> .60).
Dissociative Experiences Scale (DES-II; Carlson & Putnam, 1993). This consists of a 28-item self-report questionnaire designed to measure dissociative symptoms in clinical and non-clinical populations. It provides a total score and scores on three different subscales: dissociative amnesia, absorption, and depersonalization/derealization (Carlson & Putnam, 1993). The items are answered on a percentage scale that measures the frequency at which the item occurs in daily life, where 0% is it has never occurred and 100% is it occurs very frequently. The Spanish version was adapted by Icaran, Colom, and Orengo-García (1996) and has a Cronbach's α of .91.
Launay-Slade Hallucination Scale-revised (LSHS-R; Bentall & Slade, 1985). This is a scale for measuring hallucination proneness in normal and psychiatric populations. The LSHS-R was developed based on the assumption that hallucinatory experiences are part of a continuum of normal to psychotic functioning. This study used the 12-item Spanish version (Fonseca-Pedrero et al., 2010) which is answered on a four-point Likert-type scale (1=does not apply to me, 2=may possibly not apply to me, 3=may possibly apply to me, and 4=applies to me). The score varies from 12 to 48, with higher scores showing more proneness to hallucinations. Internal consistence of the questionnaire has a Cronbach's alpha of .90.
ProcedureThe participants who signed their informed consent were assigned a study participation code and were emailed a link to a form created with Google Drive with questions related to sociodemographic data, medical and psychological history, use of psychopharmaceuticals, participation code, and the VISQ-R. In the email, they were asked to fill in the test in a quiet place under optimum lighting conditions and with plenty of time, and to return it within one week. Two weeks after each participant had filled in the pretest, he was emailed a new Google Drive link for participation, filling in the VISQ-R scale for the second time so test-retest reliability, the DES-II, and the LSHS-R tests could be calculated. A limit of one week was set for participation in the second part, and at the end of this period research was closed and all the data were downloaded from Google Drive in a CSV file format and transferred to the SPSS 21 program.
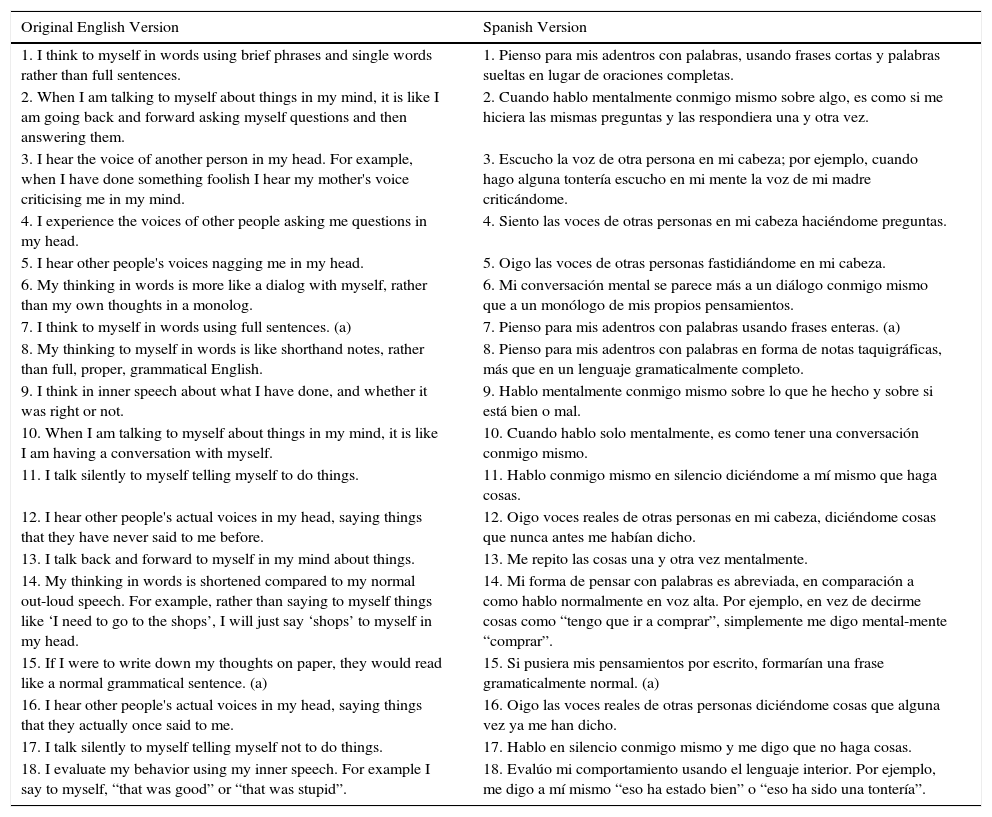
ResultsSpanish adaptation of the VISQThe items on the original version of the VISQ were translated into Spanish following the recommendations of Muñiz, Elosua, and Hambleton (2013), using the “back-translation” method, with two translators, one familiar with the Spanish culture and another familiar with the USA. The first translator translated the questionnaire into Spanish, and this translation was then translated back into English. This version was then compared with the original English version for accuracy (see Table 1).
Comparison of the Spanish Translation of the VISQ and the Original English Version.
| Original English Version | Spanish Version |
|---|---|
| 1. I think to myself in words using brief phrases and single words rather than full sentences. | 1. Pienso para mis adentros con palabras, usando frases cortas y palabras sueltas en lugar de oraciones completas. |
| 2. When I am talking to myself about things in my mind, it is like I am going back and forward asking myself questions and then answering them. | 2. Cuando hablo mentalmente conmigo mismo sobre algo, es como si me hiciera las mismas preguntas y las respondiera una y otra vez. |
| 3. I hear the voice of another person in my head. For example, when I have done something foolish I hear my mother's voice criticising me in my mind. | 3. Escucho la voz de otra persona en mi cabeza; por ejemplo, cuando hago alguna tontería escucho en mi mente la voz de mi madre criticándome. |
| 4. I experience the voices of other people asking me questions in my head. | 4. Siento las voces de otras personas en mi cabeza haciéndome preguntas. |
| 5. I hear other people's voices nagging me in my head. | 5. Oigo las voces de otras personas fastidiándome en mi cabeza. |
| 6. My thinking in words is more like a dialog with myself, rather than my own thoughts in a monolog. | 6. Mi conversación mental se parece más a un diálogo conmigo mismo que a un monólogo de mis propios pensamientos. |
| 7. I think to myself in words using full sentences. (a) | 7. Pienso para mis adentros con palabras usando frases enteras. (a) |
| 8. My thinking to myself in words is like shorthand notes, rather than full, proper, grammatical English. | 8. Pienso para mis adentros con palabras en forma de notas taquigráficas, más que en un lenguaje gramaticalmente completo. |
| 9. I think in inner speech about what I have done, and whether it was right or not. | 9. Hablo mentalmente conmigo mismo sobre lo que he hecho y sobre si está bien o mal. |
| 10. When I am talking to myself about things in my mind, it is like I am having a conversation with myself. | 10. Cuando hablo solo mentalmente, es como tener una conversación conmigo mismo. |
| 11. I talk silently to myself telling myself to do things. | 11. Hablo conmigo mismo en silencio diciéndome a mí mismo que haga cosas. |
| 12. I hear other people's actual voices in my head, saying things that they have never said to me before. | 12. Oigo voces reales de otras personas en mi cabeza, diciéndome cosas que nunca antes me habían dicho. |
| 13. I talk back and forward to myself in my mind about things. | 13. Me repito las cosas una y otra vez mentalmente. |
| 14. My thinking in words is shortened compared to my normal out-loud speech. For example, rather than saying to myself things like ‘I need to go to the shops’, I will just say ‘shops’ to myself in my head. | 14. Mi forma de pensar con palabras es abreviada, en comparación a como hablo normalmente en voz alta. Por ejemplo, en vez de decirme cosas como “tengo que ir a comprar”, simplemente me digo mental-mente “comprar”. |
| 15. If I were to write down my thoughts on paper, they would read like a normal grammatical sentence. (a) | 15. Si pusiera mis pensamientos por escrito, formarían una frase gramaticalmente normal. (a) |
| 16. I hear other people's actual voices in my head, saying things that they actually once said to me. | 16. Oigo las voces reales de otras personas diciéndome cosas que alguna vez ya me han dicho. |
| 17. I talk silently to myself telling myself not to do things. | 17. Hablo en silencio conmigo mismo y me digo que no haga cosas. |
| 18. I evaluate my behavior using my inner speech. For example I say to myself, “that was good” or “that was stupid”. | 18. Evalúo mi comportamiento usando el lenguaje interior. Por ejemplo, me digo a mí mismo “eso ha estado bien” o “eso ha sido una tontería”. |
Note. (a): reverse scored item.
The new VISQ factor items were developed based on the theoretical framework of Hermans (2014) and Perona-Garcelán et al. (2015). All of them were proposed by the members of the research group, who are experts in treatment and approach to persons with psychotic disorders, based on their own clinical experience. The VISQ factor item structure was analyzed over Dialogic Inner Speech and Evaluative/Motivational Inner Speech, where the common characteristic was the description of internal speech as the individual's dialogues with himself. The task consisted of composing a set of items that would describe internal speech dialogues, not with oneself but with other imaginary persons, as described by Hurlburt et al. (2013) and by Hermans (2014). We believe this characteristic of inner speech was not covered in the original version of the VISQ.
In the first stage, items were generated in a brainstorming meeting, at which the goals of the scale were specified first and then items were proposed. Fifteen items were chosen by consensus. In the second stage, the items proposed were sent to four clinical psychologists with over 10 years of experience in treatment and research of psychosis in Spain. In an email, they were each explained the purposes of the study and asked to evaluate the validity of the items proposed for measuring this variety of inner speech, eliminating or modifying those items which they did not think were valid, or contributing other new items more pertinent for the construction of the scale.
This group of experts eliminated eight items and rewrote the others so they fit the goal proposed better. With the contributions and corrections of the group of experts, seven items were selected which were considered to best describe inner speech as a dialogue with imaginary others. They were:
- -
Cuando hablo conmigo mismo es como si hablase con otra persona.
- -
Cuando hablo conmigo mismo tengo la sensación de atender al punto de vista de otro.
- -
Cuando hablo conmigo mismo me vienen de pronto a la cabeza preguntas o comentarios que parecen que no son míos, pero sí lo son.
- -
Me parece que cuando pienso es como si hablara o conversara con más gente (familiares, amigos, conocidos, etc.).
- -
Cuando pienso en algo tengo la impresión de que hay partes de mi que no están de acuerdo con lo que pienso.
- -
Cuando pienso tengo la sensación de que me dirijo a otra persona.
- -
Cuando hablo conmigo mismo es como si discutiese con un conocido.
Following Hermans (2014), we have called this factor Dialogue with Self-Positions in Inner Speech. These items were included along with the items on the original scale in random order. The final version of the VISQ Scale was made up of the following factors:
- -
Dialogic Inner Speech: 4 items.
- -
Condensed Inner Speech: 5 items.
- -
Other People in Inner Speech: 5 items.
- -
Evaluative/Motivational Inner Speech: 4 items.
- -
Dialogue with the Self-positions in Inner Speech: 7 items.
As a last step, to find out whether the scale would be properly understood, it was administered to a group of five patients with psychiatric diagnoses (two with borderline personality and three with a psychotic disorder), so any corrections could be made for the final version. The final name of the scale was the VISQ-R.
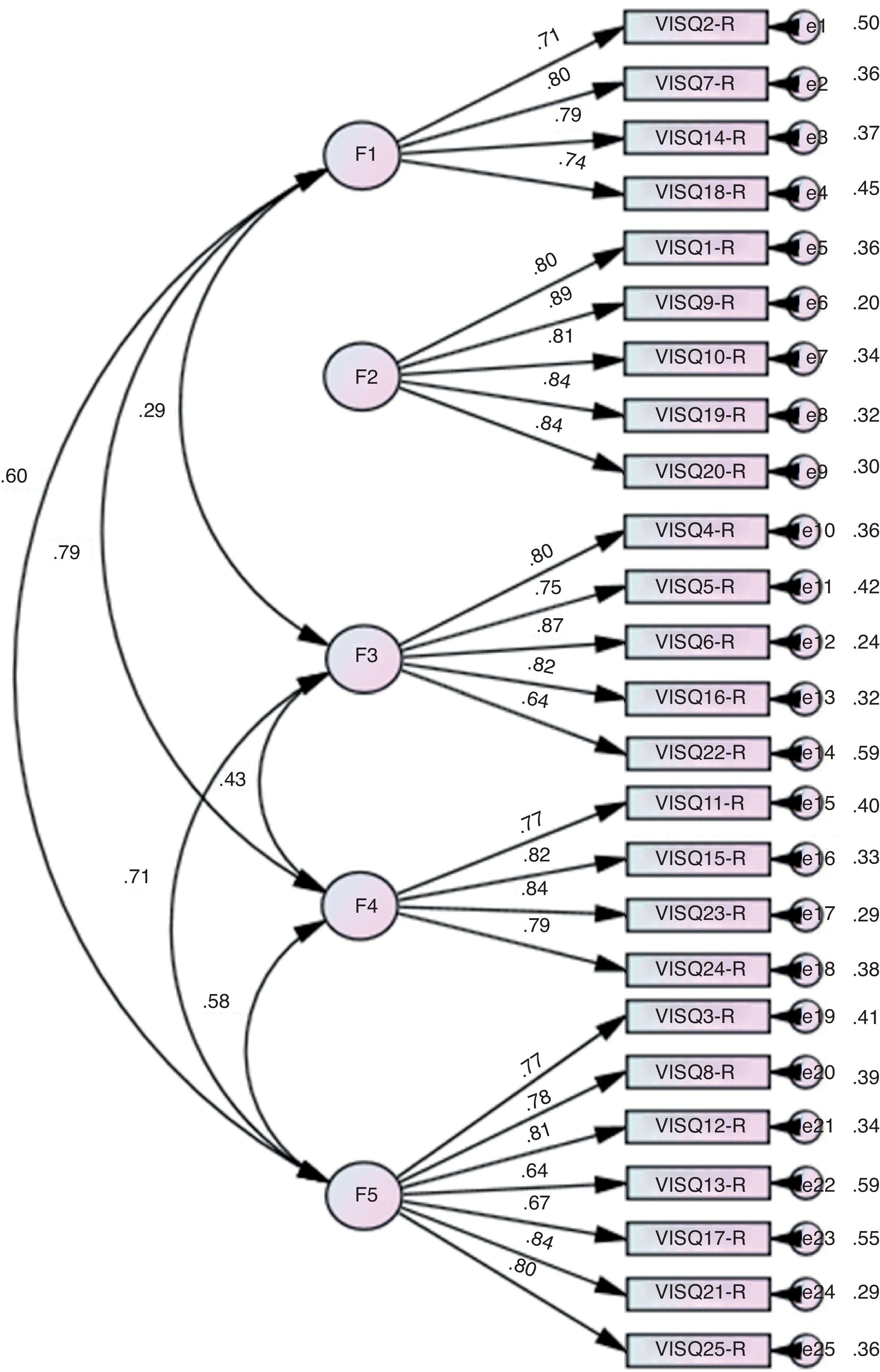
Confirmatory Factor Analysis of the VISQ-RA Confirmatory Factor Analysis (CFA) was done to evaluate the suitability of the VISQ-R scale structure with the new fifth factor items using Robust Diagonally Weighted Least Squares (RDWLS), as the multivariate normality assumption was not met. Mardia's test yielded 42.73, p<.001. The goodness-of-fit indices of this model were adequate, χ2(265)=605.95, p<.01, Comparative Fit Index (CFI)=.97, Normed Fit Index (NFI)=.95, Non-Normed Fit Index (NNFI)=.97, Goodness of Fit Index (GFI)=.96, and Root Mean Square Error of Approximation (RMSEA) and its 90% confidence interval=0.066 (0.059-0.073). Factor loadings ranged from .64 to .89. The Dialogic Inner Speech factor with both the Evaluative/Motivational Inner Speech (r=.79) and Dialogue with the Self-Positions in Inner Speech factors (r=.60) were strongly correlated. A high correlation was found between Other People in Inner Speech and Dialogue and the Self-Positions in Inner Speech (r=.71). However, correlations between the Condensed Inner Speech factor and the rest of the factors were very low (see Figure 1).

Results of Confirmatory Factor Analysis of the VISQ-R scale, in which F1 is the Dialogic Inner Speech factor, F2 is Condensed Inner Speech, F3 is Other People in Inner Speech, F4 is Evaluative/Motivational Inner Speech and F5 is the new Dialogue with Self-Positions in Inner Speech factor. Correlations of F2 with the other factors have been omitted because they were not significant.
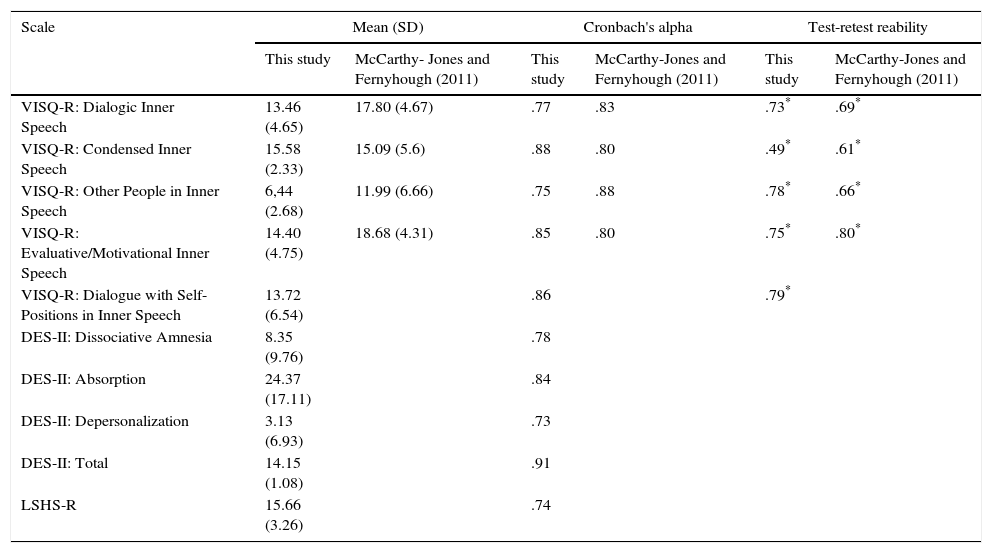
Table 2 shows the means and standard deviations of the factors in the Spanish version of the VISQ-R, the DES-II, and LSHS-R. The Cronbach's alpha for the overall 25-item scale was α=.87. Table 2 shows the Cronbach's alpha for each of the factors in the VISQ-R in the Spanish and English versions.
Means and Standard Deviations of the Five VISQ-R, DES-II and LSHS-R Factors. Cronbach's α and test-retest reliability for VISQ-R compared to the McCarthy-Jones and Fernyhough's (2011) study are also shown.
| Scale | Mean (SD) | Cronbach's alpha | Test-retest reability | |||
|---|---|---|---|---|---|---|
| This study | McCarthy- Jones and Fernyhough (2011) | This study | McCarthy-Jones and Fernyhough (2011) | This study | McCarthy-Jones and Fernyhough (2011) | |
| VISQ-R: Dialogic Inner Speech | 13.46 (4.65) | 17.80 (4.67) | .77 | .83 | .73* | .69* |
| VISQ-R: Condensed Inner Speech | 15.58 (2.33) | 15.09 (5.6) | .88 | .80 | .49* | .61* |
| VISQ-R: Other People in Inner Speech | 6,44 (2.68) | 11.99 (6.66) | .75 | .88 | .78* | .66* |
| VISQ-R: Evaluative/Motivational Inner Speech | 14.40 (4.75) | 18.68 (4.31) | .85 | .80 | .75* | .80* |
| VISQ-R: Dialogue with Self-Positions in Inner Speech | 13.72 (6.54) | .86 | .79* | |||
| DES-II: Dissociative Amnesia | 8.35 (9.76) | .78 | ||||
| DES-II: Absorption | 24.37 (17.11) | .84 | ||||
| DES-II: Depersonalization | 3.13 (6.93) | .73 | ||||
| DES-II: Total | 14.15 (1.08) | .91 | ||||
| LSHS-R | 15.66 (3.26) | .74 | ||||
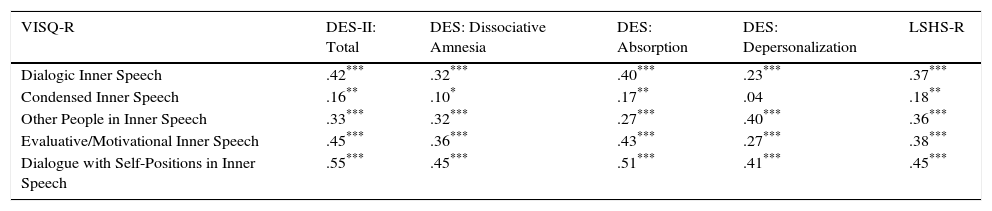
Table 3 shows the correlations between VISQ-R factors, the different dissociation dimensions and hallucination proneness. As may be observed in this table, all the VISQ-R factors correlated significantly with Proneness to Hallucinations and Dissociation except for the relationship between Condensed Inner Speech and Depersonalization, which was not significant.
Correlations between the VISQ-R, the DES-II Dissociation Scale and its Three factors (Dissociative Amnesia, Depersonalization and Absorption) and the Hallucination Proneness Scale (LSHS-R) (N=295).
| VISQ-R | DES-II: Total | DES: Dissociative Amnesia | DES: Absorption | DES: Depersonalization | LSHS-R |
|---|---|---|---|---|---|
| Dialogic Inner Speech | .42*** | .32*** | .40*** | .23*** | .37*** |
| Condensed Inner Speech | .16** | .10* | .17** | .04 | .18** |
| Other People in Inner Speech | .33*** | .32*** | .27*** | .40*** | .36*** |
| Evaluative/Motivational Inner Speech | .45*** | .36*** | .43*** | .27*** | .38*** |
| Dialogue with Self-Positions in Inner Speech | .55*** | .45*** | .51*** | .41*** | .45*** |
Finally, to study the mediating role of dissociation, and specifically, of the Dissociative Amnesia, Absorption, and Depersonalization factors between the different types of inner speech and proneness to hallucinations, a multiple mediation analysis was done. For this we followed the Hayes (2013) procedure using a 95% confidence interval (CI) and 5,000 bootstrap samples. According to these authors, if the 95% CI does not include zero, then the effect is said to be significant with p<.05.
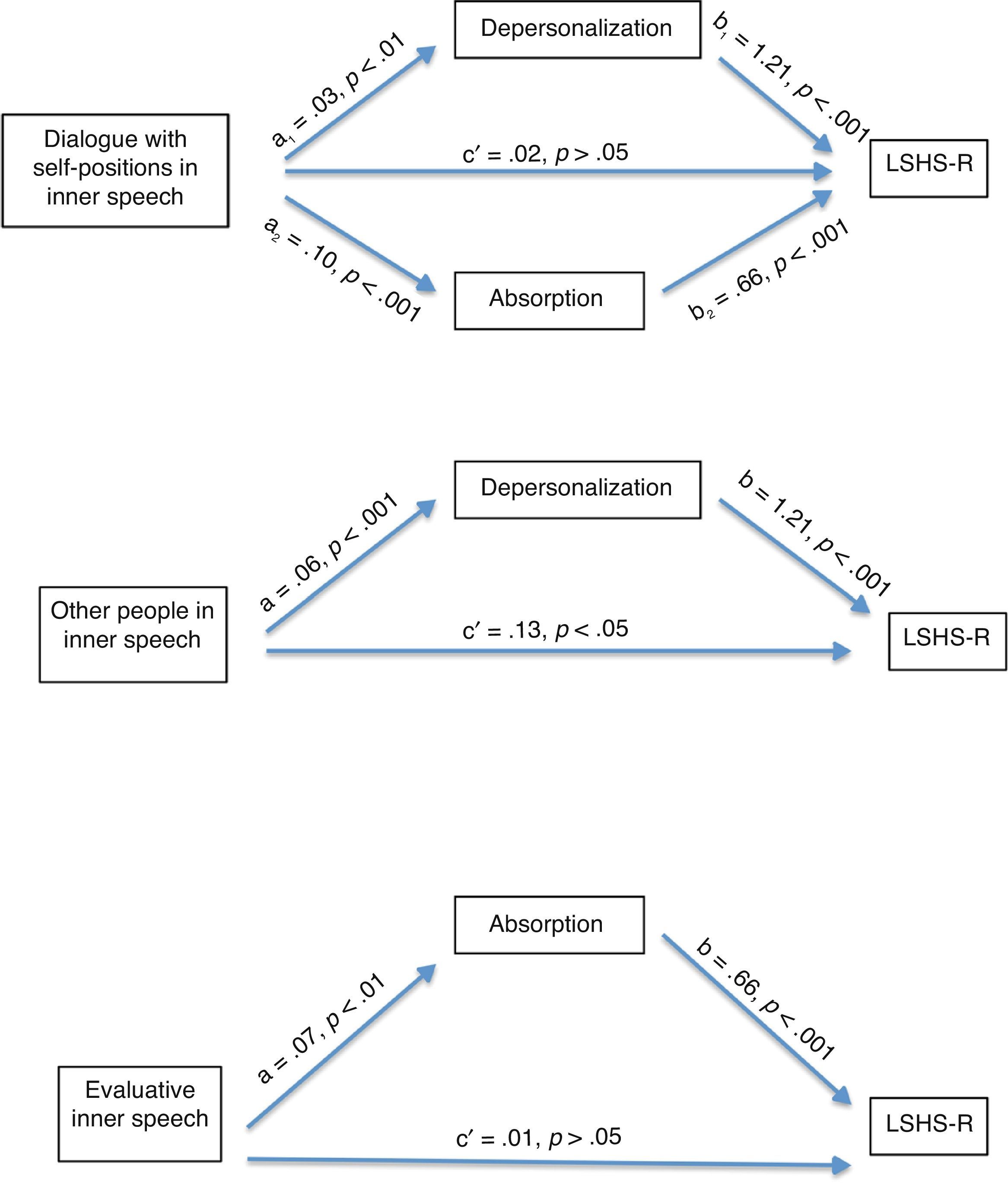
As shown in Figure 2, Dissociation (Absorption and Depersonalization) mediates between the different varieties of inner speech and hallucination proneness, except in condensed speech and Dialogic Inner Speech. More specifically, we found partial mediation of Depersonalization between Other People in Inner Speech and hallucination proneness, a x b=0.08 (IC: 0.012-0.220); c′=.127, p<.05; c=.22, p<.01. There was full mediation of Absorption between Evaluative/Motivational Inner Speech and hallucination proneness, a x b=0.05 (IC: 0.017-0.101) c′=.019, p>.05; c=.08, p>.05. Finally, we found full mediation of Absorption and Depersonalization between Dialogue with Self-Positions and hallucination proneness: Absorption, a x b=.06 (IC: 0.033-0.112); Depersonalization: a x b=.03 (IC: 0.012-0.076); c′=.023, p>.05; c=.12, p<.01. Dissociative Amnesia did not mediate between any of the variables studied.
 in which the mediators are absorption and depersonalization. The Dissociative Amnesia variable was omitted as it showed no significant mediation.")
Graphic representation of mediation analyses of the VISQ-R Dialogue with Self-Positions in Inner Speech subscales, Other People in Inner Speech and Evaluative Inner Speech and proneness to hallucinations (LHSH-R) in which the mediators are absorption and depersonalization. The Dissociative Amnesia variable was omitted as it showed no significant mediation.
The purpose of this study was to validate the Spanish version of the Varieties of Inner Speech Questionnaire scale, with a new additional factor called Dialogue with Self-Positions in Inner Speech. In the second place, we intended to examine the relationship between the varieties of inner speech and dissociation, and observe how these two factors are associated with hallucination proneness.
CFA confirmed that the factor structure of the new version of the VISQ was made up of the four factors in the English version and the new factor, which we have called Dialogue with Self-Positions in Inner Speech. The entire new version of the scale was made up of 25 items, all five factors showing good internal consistency and good test-retest reliability.
Inclusion of the new Dialogue with Self-Positions in Inner Speech factor enriches and broadens the coverage of varieties of internal speech, by enabling identification of a variety of inner speech which the English version of the VISQ does not take into account, a person's internal dialogue with imaginary others.
This type of inner speech was described by Hermans (2014) in their conception of the dialogical self, and is grounded in authors such as G. H. Mead (1934), who said that a child can internalize the reactions of significant persons with whom he lives, and integrates them in what this author called the “generalized other”. Vygotsky (1987) showed that social dialogues are interiorized forming internal speech, in which the different perspectives of reality with which the child is in contact throughout his development are integrated, and Fernyhough (2004) stated that mature internal speech would be the result of continuous dialogue among those internalized perspectives which the person keeps up simultaneously.
With respect to the relationship between inner speech, dissociation, and hallucination proneness, the hypothesis that dissociation mediates the relationship between inner speech and proneness to experiencing hallucinations was confirmed. This relationship is different for each of the VISQ-R factors. Specifically, there was full mediation of Absorption and Depersonalization between Dialogue with Self-Positions and Hallucination Proneness, as well as full mediation of Absorption between Evaluative/Motivational inner Speech and Hallucination Proneness. There was also partial mediation of Depersonalization between Other People in Inner Speech and hallucination proneness. This is in agreement with those found by Alderson-Day et al. (2014). However, the dissociative variables did not mediate between Dialogic Inner Speech or Condensed Inner Speech and Hallucination Proneness.
These results are coherent with the theoretical proposal by Perona-Garcelán et al. (2015), in the sense that auditory hallucinations would come about when the different self-positions that make up the person's self at any given moment become dissociated from each other, so that they are experienced as “significant others”. This result also confirms the need to have entered this factor, representing one of the variations of inner speech that was not included in the original version of the VISQ-R, as an independent factor in the VISQ-R scale. From the perspective of this theoretical framework, our results are coherent. Hermans (2014) proposed two types of self-positions. One inner self-position, which refers to facets of the experience itself perceived as part of the self (I as professional, as father, as friend, etc.), and another external self-position, symbolizing all the people and values that make up the person's social setting, which are internalized and perceived as significant (e.g., my mother/father, my peers, my neighbors, etc.). In this sense, the Evaluative/Motivational Inner Speech and Dialogic Inner Speech subscales would have to do with the first type proposed by Hermans, and the second type would have to do with the Dialogues with Self-Positions factor.
An important limitation of this study is the type of design used. As this was a correlational study, we could not arrive at conclusions with respect to causality between the variables studied. Furthermore, the Spanish version of the LSHS we used in this study does not discriminate between auditory and visual hallucinations, so the conclusions from our results are approximate for hallucinations in general and should be replicated with specific tests which measure the frequency or severity of auditory verbal hallucinations. Another limitation of our study has to do with the type of instruments that we have used to measure the varieties of inner speech. Obviously, the difficulty with using a pencil and paper scale like the VISQ-R is that the information acquired is retrospective. This might bias the information acquired and might not cover all the varieties of inner speech there are. It would be desirable in future studies to use alternative measures such as the Experience Sampling Methods (ESM; Bolger & Laurenceau, 2013) or the Descriptive Experience Sampling (DES; Hurlburt et al., 2013), which enable a more ecological approach to the subject of study, because questionnaires representing the experience of inner speech, a complex phenomenological experience, may be more complicated. Moreover, in future studies with clinical populations, it would be desirable to acquire evidence of decision validity of the instrument by comparing the typology of inner speech derived from the application of the instrument proposed with the presence or not of hallucinatory experiences or other types of psychotic symptoms.
Finally, it seems that precisely due to the complexity of this phenomenon, various authors (Hurlburt et al., 2013; McCarthy-Jones & Fernyhough, 2011) have suggested that many facets and dimensions still remain to be explored and that they could be related to other psychopathological phenomena. It would be desirable for future studies to replicate these results in persons with a psychiatric pathology who hear voices, using specific instruments for measuring the whole phenomenological variety of hallucinations with instruments such as the PSYRATS (Haddock, McCarron, Tarrier, & Faragher, 1999). It would also be of interest to study the relationship of the varieties of inner speech with auditory hallucinations to compare patients with different pathologies, such as psychosis versus borderline personality disorder.
In conclusion, the VISQ-R, which fits another additional factor, Dialogues with Self-Positions in Inner Speech, has good psychometric properties. This new factor has been shown to be another independent dimension of inner speech, and could be relevant for the study of certain psychopathological phenomena such as voices.
Conflict of InterestThe authors of this article declare no conflict of interest.
