


The gum elastic bougie or Eschmann stylet is a tool designed to guide intratracheal intubation that is underutilised in our setting, despite scientific information confirming that it is highly useful in difficult intubation. This case report describes the clinical use of a simple and practical device that is seldom used on our setting, especially in patients with difficult airways.
Clinical findingsThe case presented is that of a 63-year-old female patient with a history of rheumatoid arthritis and diagnosed with abcesses in the elbow and gluteal region requiring surgical drainage. After the induction of general anesthesia, when laryngoscopy with a conventional laryngoscope was attempted, it was impossible to visualise any of the laryngeal structure (Cormack IV). With the help of the bougie, tracheal intubation was possible on first attempt.
TreatmentThe bougie is a highly useful tool in cases of difficult intubation in anesthesiology services and intensive or emergency care units. However, its use is still not widespread in our setting.
ConclusionThe bougie or “tactile stylet” is a low-cost, easy-to-use device that is useful as a first choice in the management of anticipated and unanticipated difficult airways.
El gum elastic bougie o estilete de Eschmann es una herramienta diseñada para guiar la intubación endotraqueal, subutilizada en nuestro medio a pesar de la información científica que sustenta su gran utilidad en casos de intubación difícil. Este reporte de caso describe el uso clínico de un dispositivo sencillo y práctico, poco utilizado en nuestro medio, especialmente en pacientes que presentan una vía aérea difícil.
Hallazgos clínicosSe presenta el caso de una paciente de 63 años con antecedente de artritis reumatoidea y diagnóstico de abscesos en codo y región glútea, quien requirió drenaje quirúrgico. Luego de la inducción de la anestesia general, al intentar practicar la laringoscopia con laringoscopio convencional, no fue posible visualizar ninguna estructura laríngea (Cormack IV). Con la ayuda del bougie se logró practicar la intubación traqueal al primer intento.
TratamientoEl bougie es una herramienta de gran utilidad en casos de intubación difícil, en servicios de anestesiología, cuidados intensivos o urgencias, pero su uso aun no se ha generalizado en nuestro medio.
ConclusiónEl bougie o estilete tactil es un dispositivo económico, de fácil manejo y útil como primera elección en el manejo de la vía aérea difícil anticipada y no anticipada.
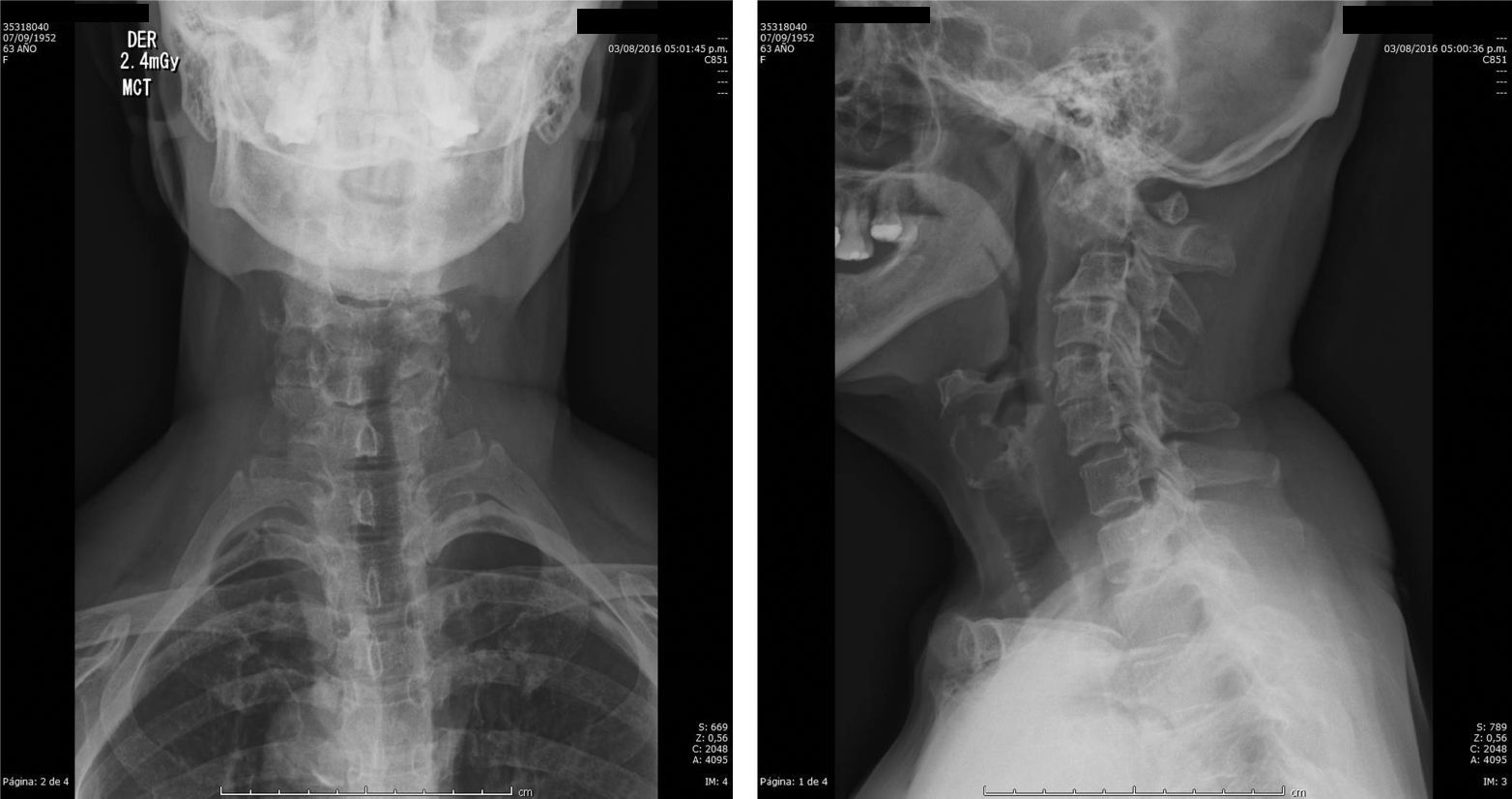
63-Year-old female patient, 49kg with an history of rheumatoid arthritis and osteoporosis, receiving multiple disease-modifying treatments, corticoids and biological medications. During a follow-up visit in rheumatology, a radiography of the cervical spine revealed evidence of subluxation of C1–C2 and C2–C3. Fig. 1 The patient presented with a clinical picture of chronic osteomyelitis of the elbows and pelvis that required a surgical procedure consisting of surgical cleaning and debridement of the left elbow and drainage of the gluteal abscess.

Significant findings during the pre-anesthetic assessment included limited oral opening (2.5cm), a thyromental distance of 5cm, severe limitation of cervical extension, and two unstable dental structures. The patient was haemodynamically stable upon arriving at the operating room, with BP 125/85mm Hg, HR 78bpm, BR 14, SpO2 95% FiO2 0.21. After confirmation of pre-operative fasting, signed informed consent, and non-invasive monitoring, induction was initiated with 70mg IV of propofol, 100mg IV of fentanyl, and 2.5mg IV of rocuronium followed by 100mg IV of succinylcholine. Laryngoscopy was performed with great difficulty due to the limited oral opening and without next extension. Given that laryngeal structures could not visualised (Cormack IV) the decision was made to insert a bougie while moving and holding the oropharyngeal structures forward with the laryngoscope. The angulated flexible tip was slid upward until the contact of the device with the carina could be felt after it had advanced approximately 25cm. There was no tactile sensation of the tracheal cartilage. Next, a No. 7 tracheal tube was inserted through the device, and the bougie was removed. The patient was connected to an anesthesia machine, uniform pulmonary ventilation was assured, and the tracheal tube was connected. Ventilation parameters were adjusted, and balanced general anesthesia was administered. The patient was in prone position during the surgical procedure. Awake extubation was performed, and there were no complications. During the immediate post-operative period, the patient did not report pharyngeal pain, dysphonia or pharyngeal bleeding.
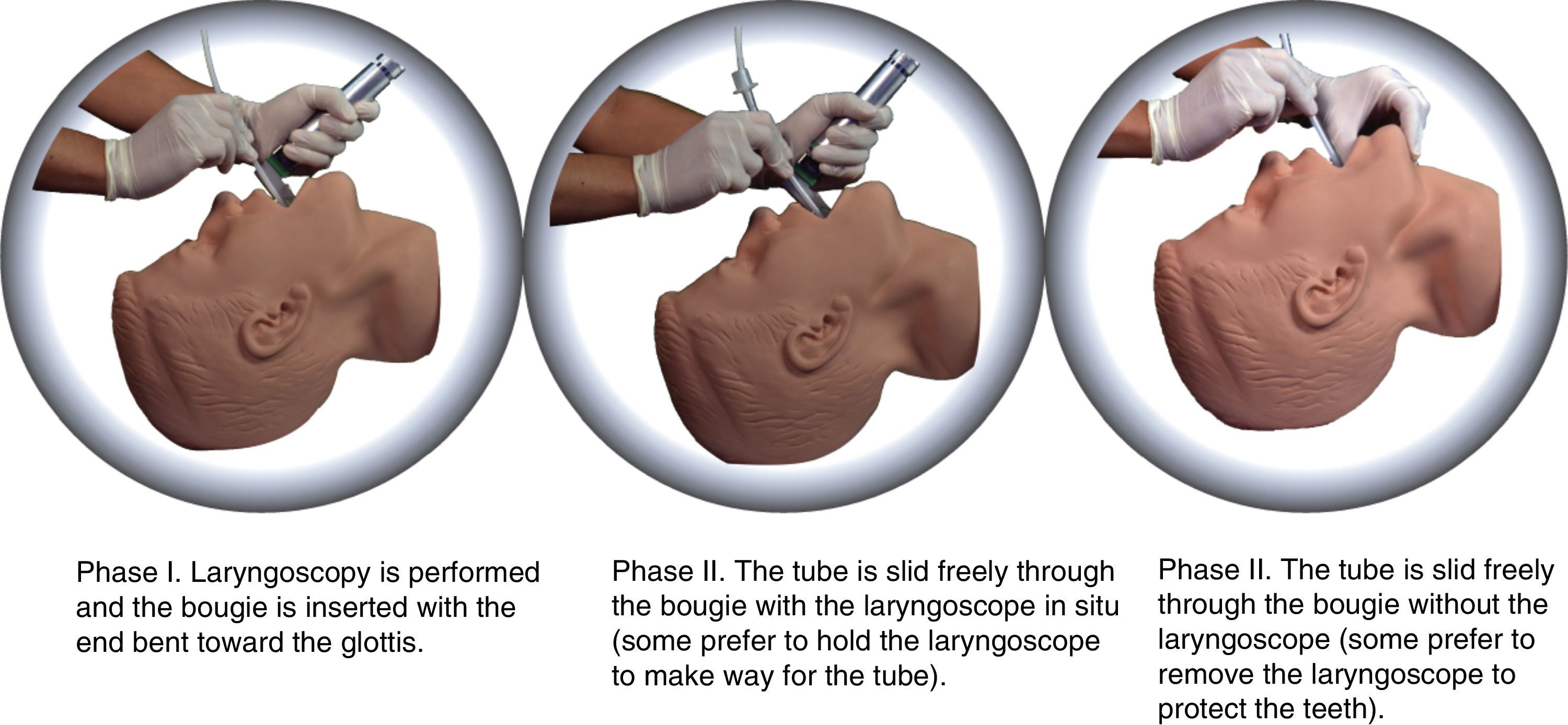
DiscussionThe gum elastic bougie (GEB), or Eschmann endotracheal introducer, is a rescue device used for rescues in cases of difficult airway, especially anticipated ones.1 It is important in operating rooms as a tool for the anaesthetist, and in emergency departments, where it has proven to be of vital importance. Despite its name, the GEB is neither made of gum, nor is it elastic, or a bougie for tracheal dilatation. For this reason, the authors believe that the term that best describes its features is that of “Tactile stylet”: when taken between the right index finger and thumb, it provides tactile sensation of the tracheal cartilages, and when advanced beyond 20cm, the distal end touches the carina, as was previously described (Fig. 2).2–4

The incorporation of the bougie into anesthesiology was thanks to Sir Robert Macintosh (1949), who is credited with using it as a guide for tracheal intubation. Duckworth gave it the name of stylet, and Paul Venn (1973) introduced it in clinical practice. The latter worked as an anesthesiology consultant for Eschmann Brothers & Walsh Ltd., and introduced the following modifications: a 35° curve in the distal end, a length of 60cm, a diameter of 5mm, and two-layer construction — an internal polyester layer and the outer resin lining. This made it rigid (semi-rigidity) but also flexible so that it could work as a true introducer in the trachea with minimal risk of damaging soft tissues.5,6
In 2014, in an editorial of the Anaesthesia journal entitled “The humble bougie… forty years and still counting?”,7 Rai reports that the device is more widely used in the United Kingdom for difficult intubation conditions and is available in more than 90% of difficult airway carts. The bougie is a priority resource in the “Plan A” of the Difficult Airway Society's (DAS) Guidelines for the management of unanticipated difficult intubation.8
Several studies and algorithm reviews from Australia, the United States of America, Singapore and France regarding the management of difficult airways and intubation describe the bougie as the most commonly used, most useful and most effective device for difficult airway management.9–12
Reports about bougie use, even by non-anaesthetists, show high success rates, ranging from 89% on the first attempt to 94%–100% in the second attempt.13,14 Complications are rare and have been mostly associated with the incorrect use of the device.15,16 The bougie has also been incorporated into video laryngoscopes, as is the case of the CoPilot VL, that has a port through which the bougie is passed to facilitate tracheal intubation.17
The Latin American experience with this device is minimal in comparison with its use in Europe and especially in the United Kingdom, not only in patients with a difficult airway (when the vocal cords cannot be visualised, Cormack III–IV) but also because of the reported reduction in the incidence of failed intubation and cricothyroidotomy.18–20 It is striking noting that in more developed countries, such as the United Kingdom, bougie use is so wide-spread among anaesthetists, and paradoxically, it is only seldom used in countries with low economic resources where great efforts go into the acquisition of much more costly equipment and technologies that require more training and are not always effective.
Insertion techniqueThe technique is very simple. It consists of advancing the device through the trachea so that the tracheal tube can be then be inserted through it, similar to the Seldinger technique used for other cannulations.2 The process consists two phases. First, the bougie is slid posterior to the epiglottis, with the distal end bent forward.21 The device must be held between the right index finger and thumb so that the movement across the tracheal rings or, failing this, contact with the carina or the bronchi can be felt. To facilitate the second phase, which is where most obstacles occur, some recommend rotating the orotracheal tube 90 degrees counter-clockwise, keeping the tube bevel pointing backward.22,23 There is controversy about maintaining the laryngoscope in place to mobilise the oropharyngeal structures forward while the tracheal tube is inserted since it has been reported that this hinders the sliding of the tube (Fig. 2).24,25
RecommendationsOf crucial importance are the recommendations of never forcing the bougie and, it being a “Tactile stylet”, to pay attention to the “clicks” caused by the end of the device hitting the tracheal rings, the feeling of standstill when it reaches the carina or even a small bronchus (at approximately 40cm), and, finally, the coughing (the least perceptible of the three) that can occur in some patients without muscle relaxation. When the patient is not adequately induced (semi-unconscious) there may be a risk of bronchospasm when the tip of the bougie hits the carina. That said, when it moves toward the esophagus, where the mucous membrane is smooth, it does not hit any structure and can advance the whole length of it, beyond 45cm.3,26
Regarding the above, it has been empirically observed in the population of patients undergoing surgery at the National University Hospital of Colombia (Hospital Universitario Nacional de Colombia), that the “tactile stylet” can also be useful as a first approach during a Cormack II or IV laryngoscopy without producing adverse effects in the patient or prolonging the process of securing the airway, just as was demonstrated in this case. Additional studies are required to evaluate the efficacy of bougie use compared to other supraglottal devices in terms of the success of orotracheal intubation and the time required to complete it.
ConclusionAlthough the incidence of difficult airway is relatively low,27 the bougie has been shown to be a useful, effective, low-cost and very easy-to-use device for facilitating intubation when the vocal cords cannot be completely visualised. Given the medical implications and the serious consequences when faced with a patient with a difficult airway, this article proposes reflecting on rescuing the use of the bougie and making it available in airway carts so that it may become the first choice for the management of anticipated and unanticipated difficult airways.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that no patient data appears in this article.
Right to privacy and informed consentThe authors declare that no patient data appears in this article.
FundingAuthors’ own resources.
Conflict of interestAuthors declare that there is no conflict of interest.
The authors thank Jorge Humberto Reyes Pimiento, industrial designer, for the creation of Fig. 2.
Please cite this article as: Navarro-Vargas JR, Becerra-Orjuela RM, Gutiérrez-León M. El Bougie o “Estilete Tactil”, una alternativa clásica útil en la intubación moderna. A propósito de un caso clínico en el Hospital Universitario Nacional de Colombia. Rev Colomb Anestesiol. 2017;45:262–266.