


IgA nephropathy is a common pattern of glomerulonephritis defined by mesangial IgA deposits. Rapidly progressive renal failure is unusual in IgA nephropathy; it may result from acute tubular necrosis or superimposed crescentic nephritis. In this uncommon situation, the risk–benefit balance is most strongly in favour of intense immunosuppressive therapy because if crescentic IgA nephritis is not treated, there will almost inevitably be rapid progression to end-stage renal disease. We report the clinical and histological features of a patient with crescentic IgA nephropathy treated successfully with intensive immunosuppression.
La nefropatía por IgA es un tipo frecuente de glomerulonefritis, definida por los depósitos mesangiales de IgA. En esta nefropatía es excepcional una insuficiencia renal rápidamente progresiva; puede ser consecuencia de una necrosis tubular aguda o una nefritis crescéntica superpuesta. En esta situación excepcional, el cociente riesgo:beneficio favorece firmemente un tratamiento intensivo con inmunosupresores porque, si la nefritis crescéntica por IgA no se trata, casi de modo inevitable, el paciente progresa rápidamente hasta una insuficiencia renal terminal. Describimos las características clínicas e histológicas de un paciente con esta entidad, que fue tratado satisfactoriamente con inmunosupresión intensiva.
IgA nephropathy is one of the most common causes of glomerulonephritis in the world and is characterized histologically by the deposition of polymeric forms of IgA within the mesangium and along glomerular capillary walls.1 The binding of IgA to putative Fc receptors on the surface of mesangial cells leads to mesangial hypercellularity. These IgA complexes stimulate cell proliferation and mesangial matrix deposition. In addition, endocapillary proliferation, karyorrhexis and crescents can also be seen on histopathology.2 It has been found that the presence of crescents in IgA nephropathy increased the risk of renal failure almost 1.5-fold and that 50% of patients with crescents and diffuse mesangial proliferation reached end-stage renal disease within five years.3 In the present case study, we successfully treated a patient of crescentic IgA nephropathy with pulse methyl prednisolone, oral steroids and intravenous cyclophosphamide.
Case reportA 27-year-old-man was referred to our hospital because of rapid renal function deterioration. Normal renal function (serum creatinine 0.9mg/dl) had been detected three months earlier to this admission. Eight days prior to admission, the patient experienced nausea, headache, oliguria, and swelling of the lower extremities. He had no history of haemoptysis, arthralgia, or skin rashes. He had no other significant past medical history. On admission, slight bilateral pretibial oedema was noted and her blood pressure was 140/72mmHg, pulse 76/min with a regular rhythm, while body temperature was normal. Body mass index (BMI) was 25.5kg/m2. His physical examination was unremarkable. Urinalysis showed 3+ for protein with numerous red blood cells in the sediment. Haemoglobin was 12.3g/dl; white blood cell count was 10,600/mm3 with 90% neutrophils, 8% lymphocytes, 1% monocytes, 0% eosinophils, and 1% basophils; platelet count was 253,000/mm3 and erythrocyte sedimentation rate was 108mm/h. Blood urea nitrogen was 64mg/dl, serum creatinine 7.8mg/dl, total serum protein 6.8g/dl (albumin 3.3g/dl), and cholesterol 175mg/dl. Serum electrolytes were within normal limits. Chest radiography showed cardiomegaly and lung congestion. An electrocardiogram was normal. On ultrasonography, both kidneys were of normal size, but increased parenchymal echogenicity with preserved cortico-medullary differentiation. Screening for hepatitis B, hepatitis C and HIV (human immunodeficiency virus) was negative. Titres of antistreptolysin-O, antistreptokinase, and serum complement were within normal range. P-anti neutrophil cytoplasmic antibody (P-ANCA), C-anti neutrophil cytoplasmic antibody (C-ANCA), antinuclear antibody (ANA), and anti-double stranded DNA (dsDNA) antibody, anti-glomerular basement membrane (GBM) antibody were negative.
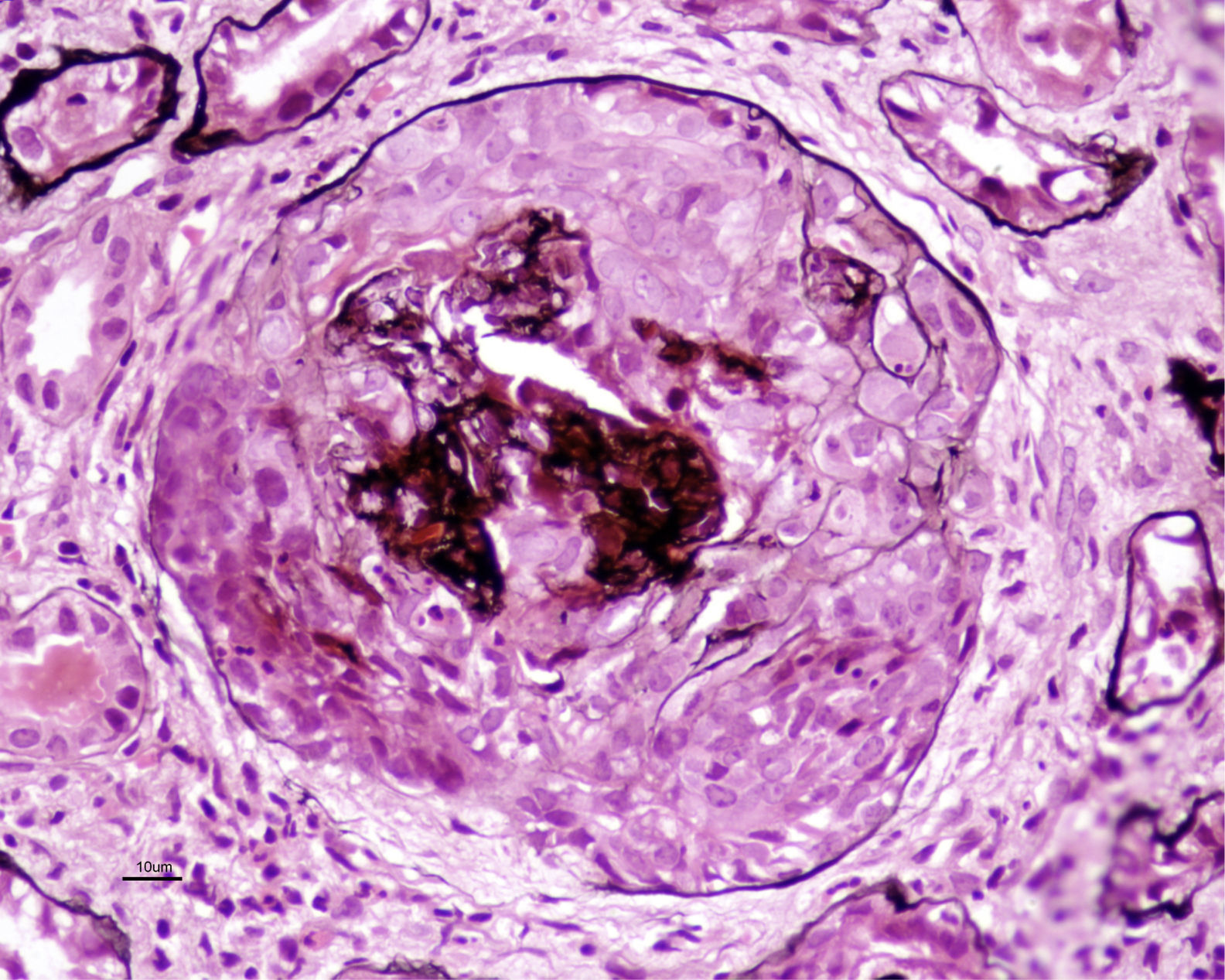
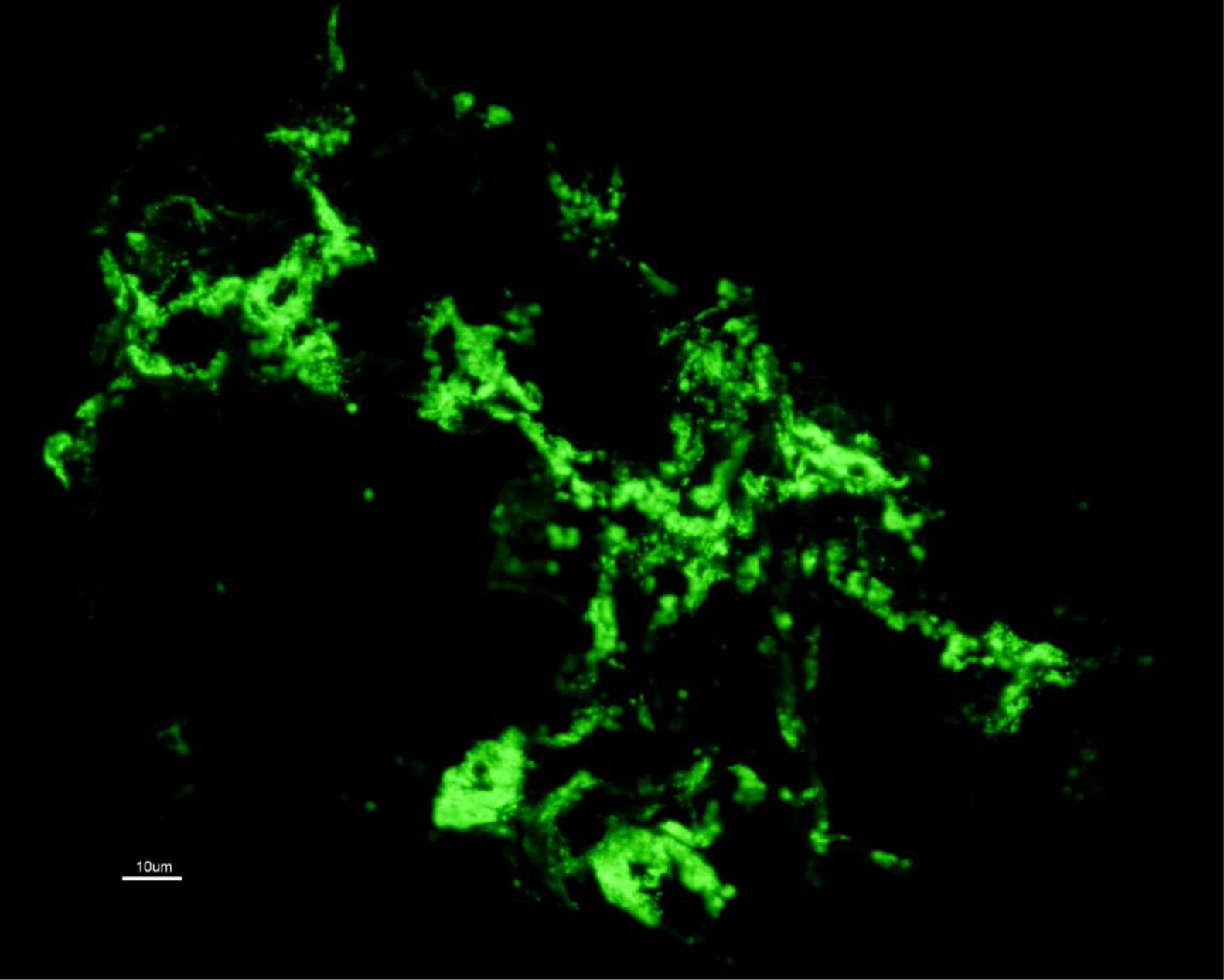
On his first hospital day, haemodialysis was initiated because of uraemia. Percutaneous renal biopsy was performed on the second day. Light microscopy revealed crescentic glomerulonephritis (Fig. 1). The number of glomeruli in the biopsy specimen was 16. Among 16 glomeruli, eleven of them show active cellular crescents occupying circumferentially. There were no necrotizing lesions in the underlying tufts. However, there was mild increase in the mesangial matrix and mesangial cellularity. Capillary walls did not show double contoured appearance. Tubules showed few RBCs in the lumen. Interstitium showed lymphocytic infiltration. Vessels showed moderate hyperplasia of tunica media without any evidence of vasculitis. Immunofluorescence demonstrated diffuse global granular deposits with IgA (3+) (Fig. 2) and C3 (1+) in mesangium. Others including IgG, IgM and C1q were negative. Kappa and lambda chain stains did not show restrictions. There were no extraglomerular deposits. Based on these histological findings, a diagnosis of crescentic glomerulonephritis secondary to IgA nephropathy was reached.


The patient was treated with intravenous methylprednisolone of 1g for 3 days during the early phase of the disease, followed by tapering dose of oral prednisolone. Intravenous cyclophosphamide was given at 0.5g/m2 body surface area monthly for 6 months. Cyclophosphamide dosages were titrated to achieve a nadir while blood cell count was between 2500 and 3000cells/ml. Omega-3 fatty acid fish oil supplementation was initiated after completion of six courses of cyclophosphamide at 12g/day. Patient's systolic and diastolic blood pressures were maintained at 120–130 and 60–70mm Hg, respectively. Patient's renal function gradually improved from serum creatinine of 7.8–1.2mg/dl at the end of twelve months. Urine protein excretion reduced from 3+ at admission to traces during follow-up. However, there was persistence of microscopic hematuria.
DiscussionWe encountered a case of crescentic IgA nephropathy. Several studies have documented a higher incidence of hypertension and nephrotic range proteinuria in patients with the crescentic form of IgA nephropathy.4,5 These features suggest that patients with this variant of the disease may have a worse prognosis. Hogg et al. observed 218 paediatric patients with IgA nephropathy and found that 20% of them had crescents on initial biopsy, and these crescents were often associated with intense glomerular inflammation.6 Abe et al. studied the clinicopathological outcome of 205 patients with IgA nephropathy and noted that patients with >25% crescents on initial biopsy had <50% renal survival after 4 years.7 Dias et al. found that the presence of crescents in IgA nephropathy were associated with increased initial serum creatinine, proteinuria and progression to end-stage renal disease.8
There is lack of uniform consensus on effective treatment for proliferative forms of IgA nephropathy. Initial trails with pulse steroids have given conflicting results. Pozzi et al. in his prospective control study demonstrated that pulse steroids slowed the progression of renal failure compared to controls.9 Julian et al. reviewed the trails assessing the efficacy of glucocorticoids in the treatment of IgA nephropathy and concluded that for patients with preserved renal function, prolonged therapy (>2years) with corticosteroids effectively slows the loss of renal function.10 Lai et al. prospectively studied the efficacy of short term steroid therapy and found that 4 months of treatment with oral prednisolone stabilized renal function only in those patients with >20% crescents on initial biopsy.11 Ballardie et al. demonstrated that combination of steroids and oral cyclophosphamide showed a 72% 5-year renal survival compared to 6% for matched controls.12 Tumlin et al. investigated clinical and histological response to methylprednisolone and intravenous cyclophosphamide in patients with crescentic, proliferative IgAN, and found significant decreases in serum creatinine and proteinuria.13 To determine the long-term effect of their therapy, they calculated the rate of progression to end stage renal disease in the treated patients compared to matched controls and found that only 8.5% in the treatment group reached end stage renal disease within 36 months of therapy as compared to 42% in the control group.
Our patient presented with rapidly progressive renal dysfunction in clinical aspects. Treatment with prednisolone and cyclophosphamide reduced proteinuria and decreased serum creatinine to 1.2mg/dl. Lack of chronicity in the kidney biopsy in the form of absence of fibrous crescents, glomerular sclerosis, interstitial fibrosis and tubular atrophy helped him to regain his renal function.
In summary, we found that steroid and short-term intravenous cyclophosphamide therapy significantly reduces proteinuria and stabilizes serum creatinine in patients with crescentic IgA nephropathy. A randomized controlled trial of immunosuppressive treatments in crescentic IgA nephropathy would be recommended.