






Carcinoid crisis (CC) has classically been considered the extreme end of the spectrum of carcinoid syndrome (CS). However, this presumption and other aspects of CC remain poorly understood. Consequently, current clinical guidelines are based on a low quality of evidence. There is no standard definition of CC and its incidence is unknown. Patients with florid CS and elevated serotonin (or its derivatives) which develop CC have been reported during decades. Nevertheless, the hypothesis that CC is due to the sudden massive release of serotonin or other vasoactive substances is unproven. Many triggers of CC (surgery, anaesthesia, peptide receptor radionuclide therapy, tumour biopsy or liver-directed treatments) have been proposed. However, data from studies are heterogeneous and even contradictory. Finally, the role of octreotide in the prevention of CC has been questioned. Herein, we report a clinical case and perform a critical review of the evidence available today on this topic.
La crisis carcinoide (CC) se ha considerado clásicamente el espectro clínico extremo del síndrome carcinoide (SC). Sin embargo, esta presunción y otros aspectos de la CC siguen siendo poco conocidos. En consecuencia, las guías clínicas actuales se basan en una evidencia de baja calidad. No existe una definición estándar de CC y se desconoce su verdadera incidencia. Pacientes con SC florido y niveles elevados de serotonina (o sus derivados) que han desarrollado CC han sido reportados durante décadas. Sin embargo, la hipótesis de que la CC se deba a la súbita liberación de serotonina u otras sustancias vasoactivas no ha sido probada. Se han propuesto diferentes desencadenantes de la CC (cirugía, anestesia, radionúclidos, biopsias o tratamientos dirigidos de las metástasis hepáticas). Sin embargo, los datos de los diferentes estudios son heterogéneos e incluso contradictorios. Finalmente, el papel del octreótide en la prevención de la CC ha sido seriamente cuestionado. A continuación presentamos un caso clínico no publicado y realizamos una revisión crítica de la evidencia disponible sobre este tema.
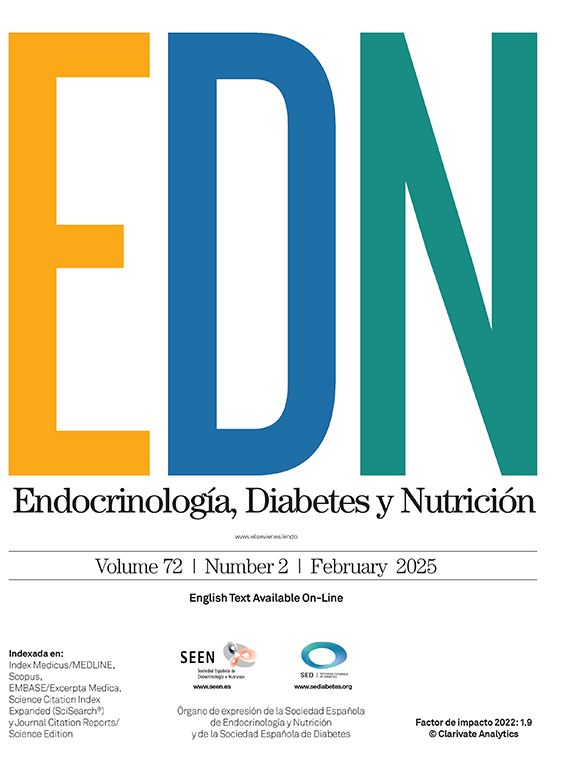
A 65-year-old female patient with previous good health complained of diarrhoea and flushing that began 6 months earlier. 24-h urine 5-hydroxyindoleacetic acid (5-HIAA) was 1129μmol/d (normal<52) and chromogranin A was 592μ/L (normal<76). Abdominal computed tomography (CT) showed enlarged mesenteric lymph nodes and multiple hepatic lesions suggestive of metastasis (Fig. 1). A biopsy of the largest hepatic mass was performed and the histologic evaluation was consistent with a well-differentiated neuroendocrine tumour (NET) with a Ki-67 index of 15%. The immunostaining was positive for synaptophysin, chromogranin A, cytokeratin CAM and CD 56. A subcutaneous long-acting (LA) somatostatin analogue (SSA) (lanreotide 120mg) was started monthly and the patient was referred to our hospital.
![Top row: Contrast-enhanced computed tomography (CT). Arterial phase (A)+portal phase (B). Enlarged liver due to multiple hepatic metastases. Bottom row: PET/CT with [68Ga]Ga-DOTA-TOC (C)+with [18F]FDG (D). C. Multiple liver metastases showing moderate overexpression of somatostatin receptors. D. Normal glucose metabolism is observed.](https://static.elsevier.es/multimedia/25300180/0000007100000006/v1_202407090532/S2530018024000751/v1_202407090532/en/main.assets/gr1.jpeg?xkr=ue/ImdikoIMrsJoerZ+w997EogCnBdOOD93cPFbanNf23BlP/DWEpPOpuWlfofnyqxn4xVHcGY2cyFujnbUAmKt+99q3UYCZ5iGU3rj+iPBO7uy2A7pmGdkKHvVxSlNpSuffwK1GzC+aB3CChDKtLp4sBhD1NsaIqS6xoyAASfrYjpPkH6R59Tw2s1DCiHmULjV1L9KJuOOEGVwpVMTdIdrRPo1oL++T/ZYPNuCeejNy3CWdcrxYdkfLmz8+C9MUfTGi1bMBkmoJ1RgTi7CaaudFGbPi0KlFRww3r5bvodnx0eXUEatHp6wkFVMrkPTD "Top row: Contrast-enhanced computed tomography (CT). Arterial phase (A)+portal phase (B). Enlarged liver due to multiple hepatic metastases. Bottom row: PET/CT with [68Ga]Ga-DOTA-TOC (C)+with [18F]FDG (D). C. Multiple liver metastases showing moderate overexpression of somatostatin receptors. D. Normal glucose metabolism is observed.")
Top row: Contrast-enhanced computed tomography (CT). Arterial phase (A)+portal phase (B). Enlarged liver due to multiple hepatic metastases. Bottom row: PET/CT with [68Ga]Ga-DOTA-TOC (C)+with [18F]FDG (D). C. Multiple liver metastases showing moderate overexpression of somatostatin receptors. D. Normal glucose metabolism is observed.
Her physical and cardiovascular examination was unremarkable. Plasma N-terminal pro-brain natriuretic peptide (NT-proBNP) was normal and echocardiography ruled out heart valve abnormalities. Carcinoid symptoms had improved but the patient continued to have 4–6 bowel movements and 3–4 flushing episodes per day so lanreotide 120mg was prescribed every two weeks.
[18F]FDG whole-body positron emission tomography (PET)/CT showed normal glucose metabolism while [68Ga]Ga-DOTA-TOC PET/CT demonstrated a moderate uptake in the mesentery and the hepatic lesions (Fig. 1). In order to control the disease progression and carcinoid symptoms, peptide receptor radionuclide therapy (PRRT) was elected. The patient received an intravenous infusion of octreotide (50μg/h) 24h before PRRT with 200mCi [177Lu]Lu-DOTA-TATE. Tolerance to treatment was adequate and a second 200-mCi dose was administrated 8 weeks later. The carcinoid symptoms showed slight improvement but the patient continued having 3–4 bowel movements, 2–3 flushing episodes per day, asthenia and anorexia. Consequently, a short-acting (SA) SSA (octreotide 100μg subcutaneously every 12h) was added.
An abdominal CT performed one month after the second dose of PRRT revealed an increase in hepatic metastasis size, then bland hepatic transarterial embolisation (TAE) was considered. Carcinoid symptoms were partially controlled, whereby the patient had 24-h preparation with an intravenous SA-SSA (octreotide 50μg/h) before TAE, and the infusion was maintained after the procedure. Within 4h after TAE, the patient experienced various and more prolonged flushing episodes, nausea, vomiting and 3 watery diarrhoeas. In addition, changes in blood pressure (BP) and heart rate (HR) were documented (Fig. 2). Therefore, intravenous fluid and a 500μg bolus of octreotide was administrated; the octreotide infusion was initially increased to 100μg/h and subsequently to 200μg/h. Over the following 4h, the carcinoid symptoms improved, BP returned to normal and the octreotide infusion was gradually reduced and then suspended. The patient was discharged under treatment with an SA-SSA (octreotide 100μg every 8h) and an LA-SSA (lanreotide 120mg every two weeks).

Did our patient have a carcinoid crisis?
Was octreotide useful?
Management and guideline recommendationsThe recent European Neuroendocrine Tumour Society (ENETS) guideline identifies carcinoid crisis (CC) as a potentially life-threatening condition, classically viewed as a complication of uncontrolled carcinoid syndrome (CS) and caused by the sudden release of serotonin and other vasoactive substances from an NET.1 It can occur spontaneously, but more frequently as a result of surgical tumour manipulation, anaesthesia, sympathomimetic drugs, biopsy or various cytolytic therapies (PRRT, hepatic embolisation). It is defined by abrupt flushing, severe shifts in BP with haemodynamic instability, profuse diarrhoea, and distressing bronchospasm.1
There are two main approaches in the management of CS: (1) direct inhibition of hormonal secretion using an SSA or (2) control of the tumour burden using cytoreductive surgery, liver-directed therapies, PRRT, chemotherapy or targeted therapy agents.2 While some tumour control approaches can act as precipitant factors for CC, SSAs are considered the cornerstone for its treatment and prevention.1
For CC management, the ENETS 2022 guideline recommends the intravenous use of octreotide, fluids, corticosteroids and vasopressors without giving further details.1 Moreover, the North American Neuroendocrine Tumor Society (NANETS) 2020 guideline and the National Comprehensive Cancer Network (NCCN) 2023 clinical practice guideline for neuroendocrine and adrenal tumours, say nothing about the treatment of CC.3,4 By contrast, these guidelines give recommendations for CC prevention. The ENETS guideline recommends prophylactic SA octreotide prior to and during invasive procedures (100–500μg subcutaneously every 6–8h or infused at a starting dose of 50μg/h, increased to 100–200μg/h if necessary).1 Furthermore, the NANETS and NCCN guidelines suggest “to consider” an SSA for patients with functional NETs as a perioperative preparation to prevent CC, but these guidelines provide no information about which patients or which procedures entail a high risk for CC development.3,4
Areas of uncertaintyThe definition, epidemiology, pathophysiology, precipitating factors and management of CC are all areas of uncertainty. While the term “carcinoid crisis” was proposed by Kahil et al.5 60 years ago for patients with CS who develop acute episodes of haemodynamic instability, the guidelines mentioned above do not provide a precise definition of CC and there is no general consensus in this regard today. Appellations such as “prolonged”, “significant”, “clinically important” or “sudden” to describe the haemodynamic instability and many different criteria for CC definition have been used (Table 1).6–12 The true incidence of CC is unknown, which is mostly due to the inconsistency in its definition across studies.13 A retrospective study with 81 patients who underwent resection of intestinal NETs (all patients received preoperative octreotide infusion) found no intraoperative CC.11 Another retrospective series that included 169 patients who had partial hepatic resection for metastatic NETs (77% received octreotide 500μg prophylactically) also found no perioperative CC.9 Woltering et al.8 also retrospectively, reported intraoperative CC in 3.4% of 150 patients who underwent 179 surgeries for metastatic NETs. In this study, all patients received octreotide 500μg/h infusions. In contrast, in two prospective series published by Condron et al.10,12 with 127 and 46 participants (patients were treated preoperatively with octreotide), CC was documented in 30% and 35%, respectively. In another prospective study, of 171 patients who underwent 195 surgeries (none received perioperative octreotide) 25% had CC.14 In this context, it is important to mention that causes of intraoperative hypotension other than CC (not always apparent) such as relative fluid deficit, anaesthetic induction agents (propofol, fentanyl), bleeding or thromboembolism events are common in oncology patients.15
Carcinoid crisis criteria, prophylaxis and treatment used in different studies.
| Definition | Study population | CS prevalence (%) | CC incidence (%) | Prophylaxis | Treatment | |
|---|---|---|---|---|---|---|
| Condron et al., 201910 | Significant HDI not attributable to other factors (vena cava compression or blood loss)SBP<80 or >180mmHg and HR>120bpm or if the patient was displaying physiology that, if sustained, would be expected to cause end organ dysfunction (ventricular arrhythmias or bronchospasm causing difficulty with ventilation) | 46 | 65 | 34 | Octreotide 500μg bolus followed by 500μg/h intraoperative infusion | Additional octreotide 500μg bolus, crystalloid boluses, vasopressors, histamine blockers and steroids as needed |
| Kwon et al., 20196 | Defined subjectively by treating physician (anaesthesiologist, surgeon or radiologist) | 75 | 47 | 32 | No previously defined (retrospective study) | Not previously defined (retrospective study) |
| Fouché et al., 201811 | “Highlyprobable”: rapid (≤5min) haemodynamic changes with HR or BP≥40% (not explained by surgical or anaesthetic management) and regressive≥20% within 5min after the octreotide bolus injection“Probable” rapid (5–10min) haemodynamic changes with HR or BP≥20–40% (not explained by surgical or anaesthetic management) and regressive or not ≥20% within 5min after the octreotide bolus injection or when confounding factors related to anaesthetic were present | 81 | 60 | 55 | 12–48h preoperative octreotide infusion 40–80μg/h, continued during the intra-and postoperative periods | Additional intraoperative octreotide boluses (0.5–2μg/kg) |
| Kinney et al., 20189 | Sudden onset of at least 2 of the following:*Flushing or urticarial not explained by an allergic reaction*Bronchospasm or bronchodilator administration *SBP<80mmHg>10min and treated with pressors not explained by volume status/haemorrhage*Dysrhythmia not explained by volume status/haemorrhage*HR≥120bpm | 169 | 28 | 0 | Octreotide 500μg subcutaneously (77% of patients) | No patient developed CC |
| Woltering et al., 20168 | SBP<80mmHg for >10minIntraoperative HDI (hypotension, hypertension, tachycardia) or when “crisis” appeared in operative notes | 150 | 85 | 3.4 | Octreotide 500μg/h pre-, intra- and postoperatively | Not previously defined (retrospective study) |
| Condron et al., 201612 | Clinically important HDI not attributable to other factors (vena cava compression or blood loss)SBP<80 or >180mmHg and HR>120bpm or if the patient was displaying physiology that, if sustained, would be expected to cause end organ dysfunction (ventricular arrhythmias or bronchospasm causing difficulty with ventilation). Consensus of the surgeon and anaesthesiologist was necessary | 127 | 74 | 30 | Octreotide 500μg bolus before anaesthesia induction followed by 500μg/h continuous infusion | Additional octreotide 500μg bolus, crystalloid boluses, vasopressors, histamine blockers and steroids as needed |
| Massimino et al., 20137 | SBP<80mmHg for >10min or Report of HDI (hypotension, sustained hypertension or tachycardia) not attributed to “obvious causes” or When anaesthesiologist or surgeon “noted” CC | 97 | 59 | 19g | VariableOctreotide 100–1100μg (median 500μg) | VariableOctreotide 350–800μg, Vasopressor agents |
BP, blood pressure; Bpm, beat per minute; CC, carcinoid crisis; CS, carcinoid syndrome, H, hours; HDI, haemodynamic instability; HR, heart rate; Min, minutes; SBP, systolic blood pressure.
In the first report from Kahil et al.5 they assumed that CC could be related to excessive amounts of serotonin. Since this earlier report, many cases of CC in patients with florid CS and elevated plasma serotonin or 24-h 5-HIAA have been described.16–19 However, the hypothesis that CC is due to the sudden massive release of serotonin or other vasoactive substances remains unproven.20 In this sense, it is worth pointing out that in the aforementioned series by Condron et al.12 11% of patients with CC had no previous symptoms of CS. One important physiologic issue is that serotonin is a potent vasoconstrictor. Therefore, it does not seem to make sense that a massive release of serotonin into the systemic circulation would cause profound hypotension.20
In an attempt to determine the pathophysiology of CC, Condron et al.10 carried out a prospective study analysing haemodynamic parameters and serum levels of some hormones classically thought to be the most likely triggers of CC. Of 46 patients with NETs and liver metastasis, 16 had intraoperative hypotensive crises. Although serotonin levels before surgery were higher in those patients who had crises, there were no significant increases of serotonin, histamine, kallikrein or bradykinin levels during the crisis. Moreover, cardiac function on transoesophageal echocardiography during the crisis was normal, but intracardiac hypovolaemia and decreased pulmonary artery pressure were observed.10 They conclude that CC seems to be consistent with a distributive shock. Thus, serotonin, histamine, kallikrein or bradykinin are not directly involved.10 Consequently, they suggest that CC could be an entirely separate pathophysiologic entity from CS, rather than the extreme end of a spectrum of CS.10
Traditional triggers of CC include surgical procedures, anaesthesia, PRRT, tumour biopsy, liver-directed therapy or even abdominal palpation.1,13 Perioperative CC (anaesthesia and surgical tumour manipulation) was evaluated in a recently published meta-analysis.21 Among 943 operations, CC occurred in 19% of surgeries. The risk was higher in patients with liver metastasis and lower in males. Impressively, classical thought-to-be risk factors such as CS or carcinoid heart disease were not significantly associated with an increased risk of CC.21
PRRT improves CS,22 but at the same time has been proposed as a precipitating factor for CC.17,23–25 In two studies with 479 and 504 patients treated with 177Lu-octreo-tate, both series reported 6 patients with CC (1.2%).26,27 Note that, in both studies, the definition used for CC was not specified. One study using 90Y-DOTA-TATE in 60 patients had a single case that required hospitalisation due to carcinoid symptoms. Here too, there is insufficient data to consider this case to be a CC.28 Similarly, a retrospective analysis conducted on 57 patients treated with 90Y-DOTA-peptides reported no CCs following the treatment.29 In the same vein, the most recent SEPTRALU study conducted in our country which evaluated the efficacy and safety of [177Lu]Lu-DOTA-TATE in 522 patients with metastatic NETs in various locations, also failed to report any CCs.30 Thus, CC caused by PRRT is exceedingly rare and seems to be confined to individual case reports.
Tumour biopsy has also been considered a trigger procedure for CC. There are several reports of patients who developed crises after hepatic, bronchial or lung NET biopsies, some of them with fatal results.31–34 In view of these 4 reported patients, a study was carried out to investigate the incidence of CC during percutaneous biopsy of NETs in a contemporary cohort.35 Among 106 CT or ultrasound guided biopsies of lung and liver NETs in 95 consecutive patients (34% had pre-existing CS and 12% received octreotide prior to the procedure), no patients experienced CC. The changes in pre-biopsy versus post-biopsy SBP, HR and oxygen saturations were −1.6mmHg (p=0.390), 0.6bpm (p=0.431), and −0.3% (p=0.113), respectively.35
CC has been reported after hepatic arterial embolisation.36,37 In a retrospective analysis of 72 patients with NETs who underwent 174 hepatic arterial embolisations, 2 patients developed CC (1.2% of treatments).38 Another series with 25 patients who received 66 sessions of radiofrequency ablation for NET liver metastases reported one CC (1.5% of treatments).39 Individual cases of CC after transoesophageal echocardiography40 and more rarely non-invasive procedures like mammography41 or repeated abdominal palpation42 can be found in the medical literature.
The use of β-adrenergic agonists has been associated with flushing and paradoxical hypotension in patients with CS,43,44 and there have been concerns regarding the use of these drugs in the anaesthetic management of patients with NETs. However, one study conducted to examine the use of vasoactive medications in patients with intraoperative CC found no significant differences in the incidence of paradoxical hypotension in patients who received β-adrenergic agonists compared to those without β-adrenergic agents.45 Based on these findings, authors recommend the use of β-adrenergic agonists to treat refractory hypotension in CC when phenylephrine and vasopressin are insufficient.45
The role of octreotide in CC is the most relevant clinical issue on the topic. The above mentioned current guidelines point to octreotide as the major player in the prevention and treatment of CC.1,3,4 The rationale that octreotide is useful for CC comes from the observation that this medication reduces flushing episodes and 5-HIAA excretion.13 Thus, this approach presupposes that CS and CC share a common pathogenesis – a fact which has not yet been proven.13 Whatever the case, the role of octreotide in the prevention and treatment of CC has been seriously questioned.13
Prophylactic periprocedural treatment with octreotide is not supported by vigorous data and no randomised studies exist in this regard.13 In the retrospective analysis of 81 patients operated on for small-bowel NETs (all patients received a preventive octreotide infusion), Fouché et al.11 reported no CC, suggesting the clinical benefit of an octreotide prophylaxis protocol. In the same vein, the previously cited series by Woltering et al.8 reported intraoperative CC in only 3.4% of 179 surgeries for metastatic NETs (all patients received a 500-μg/h infusion intra- and postoperatively). They therefore conclude that octreotide minimised the incidence of CC and, on account of their low cost and excellent safety profile, that SSAs should be used prophylactically before NET procedures.8 In contrast, the earlier mentioned series by Condron et al.12 (all patients were treated with a high dose of octreotide before surgery) with 35% CC and Wonn et al.14 (no perioperative octreotide) with 25% CC, lead the author to believe that octreotide does not prevent intraoperative CC.12,14 Similarly, the aforementioned meta-analysis which analysed perioperative CC in 943 NET surgeries also concluded that the use of prophylactic octreotide was not associated with a lesser risk of CC.21 In the same vein, a retrospective study in 161 patients showed that preprocedural use of octreotide did not affect the haemodynamic course during ablation and selective hepatic artery embolisation for NET liver metastasis.46 Other measures such as glucocorticoids, H1/H2 antihistamines, antiemetics or anxiolytic agents have been proposed for periprocedural CC prevention.23 However, these recommendations are not supported by high-evidence-level studies.
Regarding CC treatment, a crucial question is how octreotide is able to solve (or improve) CC. Of interest in this respect, is the commentary published by Pommier20 where the author asks, how might octreotide treat CC? Assuming the prevailing theory that CC is caused by the sudden and massive release of carcinoid hormones and considering that octreotide is incapable of blocking (octreotide is it not a hormone receptor blocker) or reversing the effects of hormones already released, is difficult to explain the rapid (in some cases immediate) improvement of CC after octreotide use reported in some cases.20 The author says that it could be argued that the crisis requires a continued release of hormones in order to be sustained and octreotide administration could inhibit the release of those additional hormones. In this case, it would take some time for the released hormones to be metabolised and this model does not explain the rapid improvement of CC using octreotide.20 Nevertheless, it needs to be pointed out once again that the hypothesis that CC is due to the sudden massive release of hormones continues to be unproven.20 Instead, octreotide is a well-known splanchnic vasoconstrictor that could raise systemic vascular resistance as well as squeezing blood out of the viscera, thereby improving cardiac return, cardiac output and subsequently SBP. Thus, octreotide could ameliorate CC by improving the distributive shock proposed by Condron et al.10 as the pathophysiologic mechanism of CC.20
A recent prospective study compares the outcomes in abdominal NET surgeries using an “octreotide protocol” (500μg octreotide bolus followed by infusion at 500μg per hour, plus an additional 500μg bolus as first-line treatment for CC) in 127 patients who underwent 150 operations with a “vasopressor protocol” (no perioperative octreotide and intravenous administration of vasopressors as first-line treatment for CC) in 171 patients who had 195 interventions.47 CC occurred in 30% and 25% of the octreotide and vasopressor groups, respectively. Also, despite patients in the vasopressor group being older and CS more prevalent, duration of CC, anaesthesia time, aborted operations, and hospital stay were significantly lower in this group.47 The authors conclude that vasopressors are more effective than octreotide for the treatment of intraoperative CC.47
ConclusionsCC has been and presumably will continue to be a major clinical challenge. Many important aspects of the entity (pathophysiology, management) remain poorly understood and current clinical guidelines are based on a very low quality of evidence. A consensus on the definition of CC is essential. This would be the first step in designing prospective studies that permit us to understand which patients and which circumstances increase the risk of CC. Moreover, conducting pathophysiological studies is the only way to find truly effective treatments for the prevention and management of the disease. Until further evidence becomes available, we should continue using the SA octreotide, but also intravenous fluids and vasopressor agents (including β-adrenergic agonists) to treat CC.
Ethical approvalWritten informed consent was obtained from the patient for publication of this case report.
Consent for publicationConfidentiality was protected according to National and European standards and the patient signed an informed consent form.
Grants and fundsNo author has received any grant for this research.
Conflict of interestAuthors declare that they have no conflict of interests (financial or non-financial).
Georgina Sapriki for the linguistic review of the paper.
