


Several studies have shown that low cardiorespiratory fitness (CRF) is a significant independent risk factor for future cardiometabolic disease in adult life. The aim of this study was to examine the relationship between CRF and health status in children and adolescents in Bogotá, Colombia.
MethodsA cross-sectional study was conducted in 921 children and adolescents aged 9–17 years living in the metropolitan area of the District of Bogotá, Colombia (2480m asl). CRF was assessed with the 20m shuttle run test (Course-Navette) according to ALPHA-FITNESS and FITNESSGRAM standards. Blood pressure, waist circumference, hip circumference, body composition (body fat percentage, fat body mass, and fat-free mass by bioimpedance), skin fold calipers, body mass index, and sexual maturity (Tanner) were used as indicators of physical health.
ResultsAfter adjusting for sex, age, and sexual maturity, significant inverse relationships were seen between CRF and body mass index (r=−0.107), body fat percentage (r=−0.197), fat body mass (r=−0.159), skin fold (r=−0.246), and waist circumference (r=−0.169); P<.001. Schoolchildren with low CRF levels showed OR 6.06 (95% CI 3.98–9.24) increase in body fat by bioimpedance; OR 4.04 (95% CI 1.83–9.11) risk of overweight/obese by body mass index and OR 2.47 (95% CI 1.14–5.37) abdominal obesity due to increased waist circumference.
ConclusionApproximately two thirds of participants had a CRF level suggesting future cardiovascular disease. Early identification of children and adolescents with low CRF levels will allow for implementing interventions to prevent cardiometabolic disease in adulthood.
Varios estudios han mostrado que un bajo nivel de condición física aeróbica (CFA) en la infancia se asocia con un mayor riesgo de enfermedad cardiometabólica en la edad adulta. El objetivo del presente estudio fue examinar la relación entre la CFA con el estado de salud de niños y adolescentes de Bogotá, Colombia.
MétodosEstudio descriptivo y transversal, realizado en 921 niños y adolescentes en edad escolar entre 9 y 17 años, residentes en el área metropolitana del Distrito de Bogotá, Colombia (2.480msnm). La CFA se midió siguiendo las recomendaciones del componente cardiorrespiratorio de la batería ALPHA-FITNESS y FITNESSGRAM con la prueba de ida y vuelta de 20m (Course-Navette). La tensión arterial, las circunferencias de cintura y cadera, la composición corporal (porcentaje de grasa, masa grasa y masa libre de grasa por bioimpedancia), los pliegues cutáneos, el índice de masa corporal y la maduración sexual (Tanner) fueron usados como indicadores de la salud física.
ResultadosDespués de ajustar por sexo, edad y maduración sexual, relaciones inversas fueron observadas entre la CFA y el índice de masa corporal (r=−0,107), el porcentaje de grasa (r=−0,197), la masa grasa (r=−0,159), los pliegues cutáneos (r=−0,246) y la circunferencia de cintura (r=−0,169); p<0,001. Los escolares con bajos niveles de CFA mostraron un incremento de 6,06 veces (IC 95% 3,98-9,24) de la grasa corporal por bioimpedancia; 4,04 veces (IC 95% 1,83-9,11) de riesgo de sobrepeso/obesidad por índice de masa corporal y 2,47 veces (IC 95% 1,14-5,37) de presencia de obesidad abdominal por incremento en la circunferencia de cintura.
ConclusiónAproximadamente dos tercios de los participantes tuvieron un nivel de CFA indicativo de riesgo cardiovascular futuro. La identificación temprana de niños y adolescentes con bajos niveles de CFA permitirá implementar intervenciones para promover comportamientos saludables a fin de prevenir el riesgo cardiometabólico en la edad adulta.
Data from the 2010 National Survey on Nutritional Status in Colombia1 and the World Health Organization2 from 2004 show a high prevalence of obesity and physical inactivity among schoolchildren. Both conditions are risk factors for the development of chronic diseases characteristic of adulthood but occurring increasingly earlier in adolescents and young adults.3 The presence of these risk factors significantly increases the chance of developing cardiovascular diseases, type 2 diabetes mellitus, osteoarthritis, depression, and even some malignancies such as colon, rectum, prostate, ovary, breast, and endometrial cancer.3,4
Physical fitness–especially the cardiorespiratory component–is considered to be an important indicator of health in both children and adolescents.5 Studies reported by Janz et al.6 and Castillo-Garzón et al.7 show that a low cardiorespiratory fitness (CRF) in childhood is associated with a greater risk of cardiovascular and metabolic disease in adult life. Moreover, lower cardiorespiratory fitness in childhood is considered to be an independent factor of physical and mental well-being in adult life.8 The inclusion of this health indicator in epidemiological monitoring systems in the educational setting is therefore clearly warranted.9
To measure CRF, several authors10–13 have proposed assessment batteries which have the following advantages, among others: the concurrent evaluation of several subjects, the short administration times, safety, easy application, and low cost. The most commonly used tools include EUROFIT,10 FITNESSGRAM,11 AAHPERD,12 and the recently published ALPHA-FITNESS.13 The latter was developed on a sound scientific basis and has been shown to correlate with both the current and future health of children and adolescents.14
School is an ideal setting for intervention with population-based physical activity, particularly for those with no or limited access to play areas.15 Although most schools include physical education in their curricula, children and adolescents are usually relatively inactive in them.16 In addition, there is no agreement regarding the most effective strategies for promoting behavior leading to the long-term maintenance or improvement of healthy CRF.9,15,16
In order to allow for the early identification of schoolchildren with low CRF levels and for implementing interventions to promote healthy behavior to prevent future cardiometabolic risk, a study was undertaken to explore the association between CRF and health status in children and adolescents from Bogotá, Colombia.
MethodsStudy type and populationThis study is a secondary analysis of the project Association of grip strength with early signs of cardiovascular risk in Colombian children and adolescents (FUPRECOL). A cross-sectional study was conducted of 4000 schoolchildren and adolescents aged 9–17 living in the metropolitan area of the District of Bogotá, Colombia (2480m above sea level). The 546,000 registrations of 2013, provided by the educational department of the district, were used as reference for the population. For this calculation, the following equation was used: N (αc×0.5)/1+(e2×[N−1]), where N=546,000; e precision=1%; confidence level (1−α)=99%; α=0.05. After performing a descriptive study5,11,13,14 of the physical components, the variable which showed a significant variance was CRF by VO2max. The sample size was therefore calculated to estimate a difference between the estimated and actual proportion of 5% for a sample size of 3131, which was adjusted to 4000 subjects due to potential losses in the enrollment process. Convenience sampling by order of arrival to the data collection point was used. To decrease the risk associated with a non-probabilistic sample, a sample weight was assigned–a posteriori–to each participant, calculated from stratification by age groups (±2 years). For this, «N» was considered as the population size and «n» as sample size, with probabilities of enrollment of πi=n/N and sampling weights of ωi=n/N. It was decided to intentionally select for this study a subsample of 930 participants (49% girls) at three public education centers located in urban areas of Bogotá to assess the feasibility and relevance of the fitness battery of the FUPRECOL project. Schoolchildren with a clinical diagnosis of physical, sensory and intellectual disability, non-transmissible diseases such as type 1 or 2 diabetes, cardiovascular disease, autoimmune disease, cancer, pregnancy, alcohol or drug abuse and, in general, diseases not directly related to nutrition were excluded. Effective exclusion was done a posteriori (1%, n=9 children) and was not made known to those participants, to respect their dignity.
ProceduresBefore any study measurements were made, investigators and physical education teachers did 10 theoretical and practical sessions to standardize the evaluation process. Two measurements were taken of each variable, except for the Course-Navette test, which was performed only once, as recommended by the authors of the ALPHA-FITNESS battery.13 After obtaining written informed consent from parents and guardians of the children and the assent of the participants in the presence of two witnesses, two components of the ALPHA-FITNESS were administered.13
Morphological componentWeight, height, and circumferences were measured using the established procedures.13 Participants were weighed without shoes using a portable Tanita® model TBF-410GS™ electronic scale (Arlington Heights, IL, USA) with a resolution of 0.100kg. Height was measured with a portable SECA 206® stadiometer (Seca gmbh, Hamburg) with a range of 0–220cm and a precision of 1mm. The body mass index (BMI) was used to relate weight with height. The formula proposed by Quetelet (BMI=weight [kg]/height [m]2) was used for this purpose. The cut-off points used for classification into the categories (low, normal, overweight, and obesity) adopted were based on the proposal by Cole et al.17 for children of both sexes.
Cardiorespiratory componentAn indirect and submaximal 20m shuttle run field test performed until exhaustion was used to assess CRF. The running pace was marked by a beep. Initial speed was 8.5km/h, with subsequent increases by 0.5km/h at 1min intervals, called stages. Subjects had to run between the 20m lines keeping time to when the beeps were heard. The test ended when the subject stopped due to fatigue or when he/she could not reach the line in time with the beep. Aerobic capacity was measured through maximum oxygen consumption by VO2max, estimated from the Léger equation18: VO2max (mL/kg/min−1)=31.025+3.238×S−3.248×A+0.1536×S×A, where S is the speed (in km/h) of the last complete stage and A is age (in years) of the participant.
Health statusCardiometabolic risk criteria for children and adolescents reported by the American Heart Association were used.19,20 For this, waist (WC) and hip circumference were measured using a non-stretchable anthropometric tape (Holtain Ltd., Crymych Dyfed, United Kingdom) with the anatomical landmarks described in the ALPHA-FITNESS battery.13 Systolic and diastolic blood pressure was measured after a 5min rest using a digital oscillometer OMRON™ M10-IT (OMRON Healthcare Co. Ltd., Japan). Tricipital and subscapular skinfolds (in mm) and their sum (Σ folds=tricipital+subscapular) were measured, following the cleavage lines, using a Harpenden Skinfold Caliper® (John Bull, British Indicators Ltd., United Kingdom) which exerts a constant pressure of 10g/mm2. Body composition was estimated with a body composition analyzer BC-420 MA (Tanita Corp., Tokyo, Japan) of 4 electrodes under controlled temperature and humidity conditions after voiding and a resting period of at least 15min, with the participant in light clothes, without shoes, and with arms away from the chest. This device uses dual energy X-ray absorptiometry as a reference method and calculates body composition in percent fat, fat mass, lean mass, and muscle mass based on estimates derived from regression analysis with the height, weight, and sex variables. The body adiposity index (BAI) was also estimated using the equation proposed by Bergman et al.21: BAI=([hip circumference in cm]/[height m2]1.5−18). As no cut-off points for elevated levels of adiposity, fat distribution, and body composition (percent fat, BAI, WC, tricipital fold, subscapular fold) and blood pressure (systolic and diastolic) were available for Colombian schoolchildren, the criteria of the Expert Panel of the National Cardiovascular Health Education Program of the American Heart Association19,20 were used, and values of the 95th percentile of the current population or higher were taken as reference.
Sexual maturation was assessed using the different maturation stages as described by Tanner22 by self-reports of sexual maturation staging using standard drawings differentiating the characteristics of genital development and pubic hair in males and breast development and pubic hair in females. In the Latin population, the report by Maheca Matsudo and Rodrigues Matsudo23 shows coefficients of agreement higher than 0.60 (Cohen's kappa) between direct measurement by pediatricians and the self-report for breasts and pubic hair in girls (69.7–71.3%) and for genitalia combined with pubic hair in boys (60%).
Ethical issuesThe study was conducted in compliance with ethical standards recognized by the Declaration of Helsinki and Decision 008439 in 1993 of the Colombian Ministry of Health regulating clinical research in humans. A detailed explanation of the study was given before the start of the study, and prior written consent was requested from each child or adolescent and from his/her father/mother or guardian. The managers of the schools participating in the study also gave their consent. The FUPRECOL project was submitted for evaluation to the Committees for Human Research of the participating universities (UMB No. 02-1902-2014 and UR No CEI-ABN026-000262) and was approved by them.
Statistical analysisInformation processing and analysis was performed using the Statistical Package for Social Science®, version 22 (SPSS; Chicago, IL, USA). A Kolmogorov–Smirnov test was used to verify normal data distribution. Continuous values were expressed as mean±standard deviation and proportions were given as percentages. Tests for homogeneity of variance were used, with a one-way ANOVA test for differences between continuous variables and a Chi-square test for differences between proportions. A Pearson's correlation coefficient was used to examine the relationship between health status variables and CRF levels. Finally, odds ratios and 95% confidence intervals (95% CIs) adjusted for age, sex, and sexual maturation were calculated using stepwise forward selection and step by step methods. The variable inclusion procedure was terminated when the p significance provided by a variable upon entry into the regression exceeded 0.05 between healthy or risk levels, depending on the CRF value. The participants were categorized as having a healthy aerobic capacity level if VO2max was ≥42mL/kg/min−1 for males and ≥35–40mL/kg/min−1 for females, depending on age. Participants with values lower than the above were categorized as having an unhealthy aerobic capacity level or as being at future cardiovascular risk, as established in the 2011 FITNESSGRAM battery.11,24 A value of p<0.05 was considered statistically significant.
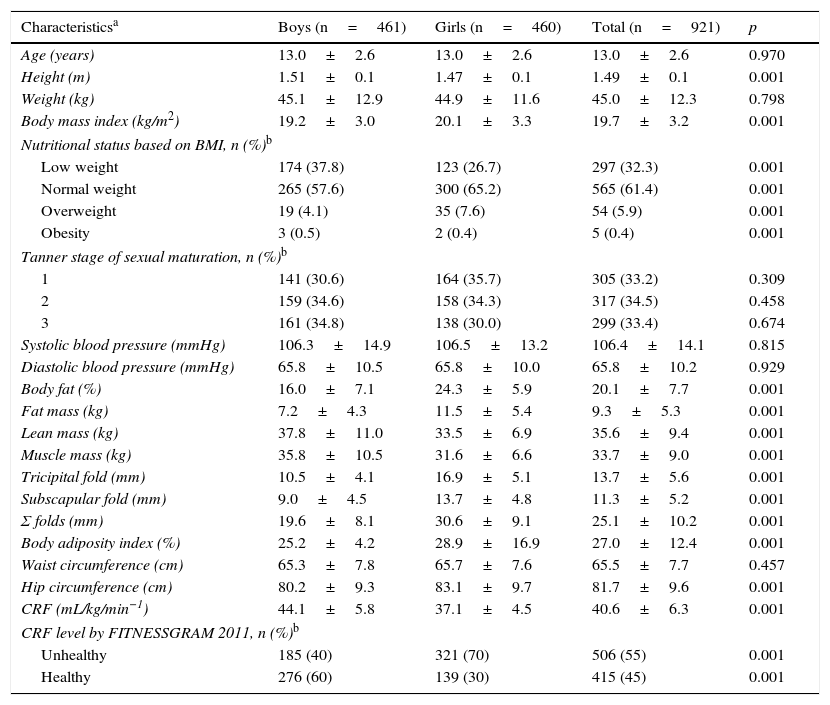
ResultsCharacteristics of the populationTable 1 summarizes the general characteristics of the participants. Boys had higher height, lean mass, muscle mass, and CRF values as compared to girls (p<0.001). An unhealthy CRF was found in a significantly higher proportion of girls (70%) as compared to boys (40%) (p<0.001). As regards body composition, girls had higher levels of fatty tissue components and distribution (percent body fat, lean mass, skinfolds, Σ folds, BAI, and hip circumference); p<0.001. No sex differences were found in age, body weight, sexual maturation, blood pressure values, and WC.
Characteristics of health status of children and adolescents from Bogotá, Colombia.
| Characteristicsa | Boys (n=461) | Girls (n=460) | Total (n=921) | p |
|---|---|---|---|---|
| Age (years) | 13.0±2.6 | 13.0±2.6 | 13.0±2.6 | 0.970 |
| Height (m) | 1.51±0.1 | 1.47±0.1 | 1.49±0.1 | 0.001 |
| Weight (kg) | 45.1±12.9 | 44.9±11.6 | 45.0±12.3 | 0.798 |
| Body mass index (kg/m2) | 19.2±3.0 | 20.1±3.3 | 19.7±3.2 | 0.001 |
| Nutritional status based on BMI, n (%)b | ||||
| Low weight | 174 (37.8) | 123 (26.7) | 297 (32.3) | 0.001 |
| Normal weight | 265 (57.6) | 300 (65.2) | 565 (61.4) | 0.001 |
| Overweight | 19 (4.1) | 35 (7.6) | 54 (5.9) | 0.001 |
| Obesity | 3 (0.5) | 2 (0.4) | 5 (0.4) | 0.001 |
| Tanner stage of sexual maturation, n (%)b | ||||
| 1 | 141 (30.6) | 164 (35.7) | 305 (33.2) | 0.309 |
| 2 | 159 (34.6) | 158 (34.3) | 317 (34.5) | 0.458 |
| 3 | 161 (34.8) | 138 (30.0) | 299 (33.4) | 0.674 |
| Systolic blood pressure (mmHg) | 106.3±14.9 | 106.5±13.2 | 106.4±14.1 | 0.815 |
| Diastolic blood pressure (mmHg) | 65.8±10.5 | 65.8±10.0 | 65.8±10.2 | 0.929 |
| Body fat (%) | 16.0±7.1 | 24.3±5.9 | 20.1±7.7 | 0.001 |
| Fat mass (kg) | 7.2±4.3 | 11.5±5.4 | 9.3±5.3 | 0.001 |
| Lean mass (kg) | 37.8±11.0 | 33.5±6.9 | 35.6±9.4 | 0.001 |
| Muscle mass (kg) | 35.8±10.5 | 31.6±6.6 | 33.7±9.0 | 0.001 |
| Tricipital fold (mm) | 10.5±4.1 | 16.9±5.1 | 13.7±5.6 | 0.001 |
| Subscapular fold (mm) | 9.0±4.5 | 13.7±4.8 | 11.3±5.2 | 0.001 |
| Σ folds (mm) | 19.6±8.1 | 30.6±9.1 | 25.1±10.2 | 0.001 |
| Body adiposity index (%) | 25.2±4.2 | 28.9±16.9 | 27.0±12.4 | 0.001 |
| Waist circumference (cm) | 65.3±7.8 | 65.7±7.6 | 65.5±7.7 | 0.457 |
| Hip circumference (cm) | 80.2±9.3 | 83.1±9.7 | 81.7±9.6 | 0.001 |
| CRF (mL/kg/min−1) | 44.1±5.8 | 37.1±4.5 | 40.6±6.3 | 0.001 |
| CRF level by FITNESSGRAM 2011, n (%)b | ||||
| Unhealthy | 185 (40) | 321 (70) | 506 (55) | 0.001 |
| Healthy | 276 (60) | 139 (30) | 415 (45) | 0.001 |
Data are given as mean±standard deviation except as indicated.
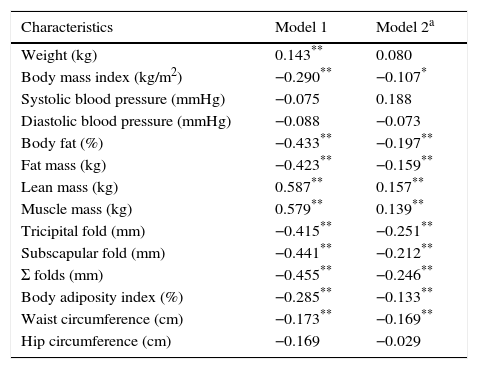
As a supplemental analysis, and to verify that higher CRF values are related to healthier values in the health status variables evaluated, a Pearson's correlation analysis was performed. After adjusting for sex, age, and sexual maturation (model 2), better CRF levels were seen to inversely and significantly relate to measures related to the risk of obesity including the BMI (r=−0.107), percent body fat (r=−0.197), lean mass (r=−0.159), tricipital fold (r=−0.251), subscapular fold (r=−0.212), Σ folds (r=−0.246), BAI (r=−0.133), and WC (r=−0.169). In this same model of analysis, lean mass and muscle mass had a linear and significant relationship with CRF levels: r=0.157 and r=0.139 respectively (Table 2).
Partial correlation between CRF levels by VO2max (mL/kg/min−1) and health status characteristics in children and adolescents from Bogotá, Colombia.
| Characteristics | Model 1 | Model 2a |
|---|---|---|
| Weight (kg) | 0.143** | 0.080 |
| Body mass index (kg/m2) | −0.290** | −0.107* |
| Systolic blood pressure (mmHg) | −0.075 | 0.188 |
| Diastolic blood pressure (mmHg) | −0.088 | −0.073 |
| Body fat (%) | −0.433** | −0.197** |
| Fat mass (kg) | −0.423** | −0.159** |
| Lean mass (kg) | 0.587** | 0.157** |
| Muscle mass (kg) | 0.579** | 0.139** |
| Tricipital fold (mm) | −0.415** | −0.251** |
| Subscapular fold (mm) | −0.441** | −0.212** |
| Σ folds (mm) | −0.455** | −0.246** |
| Body adiposity index (%) | −0.285** | −0.133** |
| Waist circumference (cm) | −0.173** | −0.169** |
| Hip circumference (cm) | −0.169 | −0.029 |
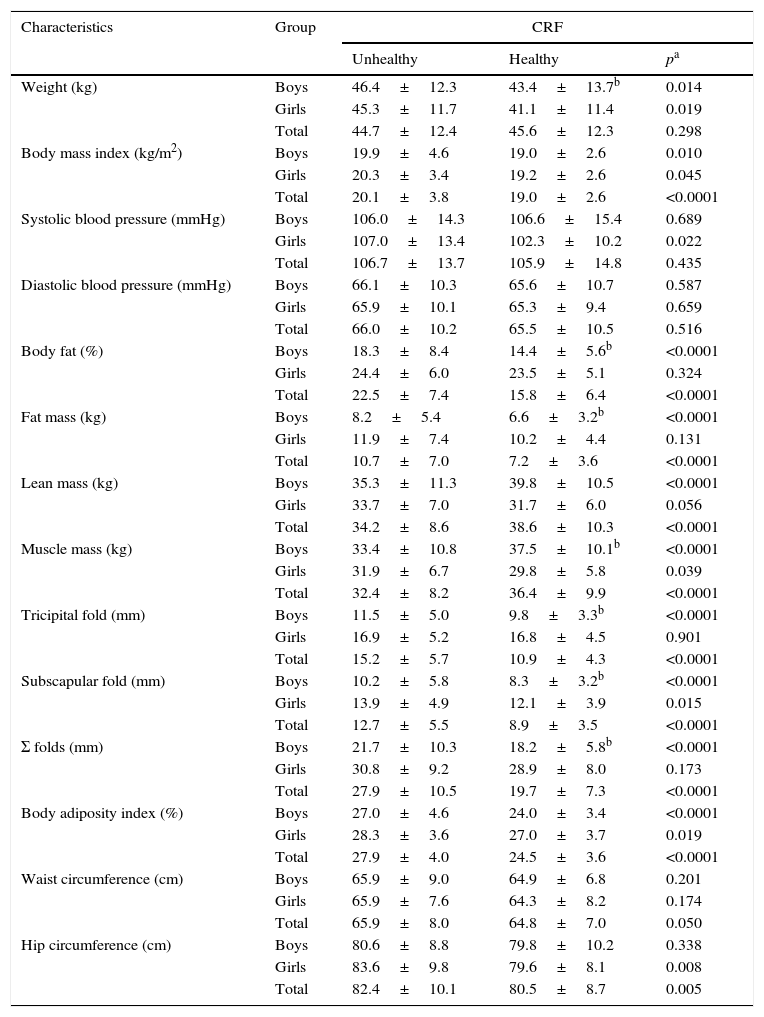
Table 3 shows that the total population with healthy aerobic capacity had significantly lower values in morphological and health components such as the BMI, percent body fat, skinfolds, BAI, and waist and hip circumferences. After separating by sex, boys located in the healthy CRF category had lower values than girls in the variables of percent body fat (14.4±5.6 vs 23.5±5.1), fat mass (6.6±3.2 vs 10.2±4.4), tricipital fold (9.8±3.3 vs 16.8±4.5), subscapular fold (8.3±3.2 vs 12.1±3.9), and Σ skinfolds (8.3±3.2 vs 12.1±3.9); p<0.001. By contrast, boys with healthy CRF levels had higher lean mass (39.8±10.5 vs 31.7±6.0) and muscle mass (37.5±10.1 vs 29.8±5.8) levels than girls (p<0.001).
Differences in health status variables between the groups of children and adolescents from Bogotá, Colombia with unhealthy and healthy CRF.
| Characteristics | Group | CRF | ||
|---|---|---|---|---|
| Unhealthy | Healthy | pa | ||
| Weight (kg) | Boys | 46.4±12.3 | 43.4±13.7b | 0.014 |
| Girls | 45.3±11.7 | 41.1±11.4 | 0.019 | |
| Total | 44.7±12.4 | 45.6±12.3 | 0.298 | |
| Body mass index (kg/m2) | Boys | 19.9±4.6 | 19.0±2.6 | 0.010 |
| Girls | 20.3±3.4 | 19.2±2.6 | 0.045 | |
| Total | 20.1±3.8 | 19.0±2.6 | <0.0001 | |
| Systolic blood pressure (mmHg) | Boys | 106.0±14.3 | 106.6±15.4 | 0.689 |
| Girls | 107.0±13.4 | 102.3±10.2 | 0.022 | |
| Total | 106.7±13.7 | 105.9±14.8 | 0.435 | |
| Diastolic blood pressure (mmHg) | Boys | 66.1±10.3 | 65.6±10.7 | 0.587 |
| Girls | 65.9±10.1 | 65.3±9.4 | 0.659 | |
| Total | 66.0±10.2 | 65.5±10.5 | 0.516 | |
| Body fat (%) | Boys | 18.3±8.4 | 14.4±5.6b | <0.0001 |
| Girls | 24.4±6.0 | 23.5±5.1 | 0.324 | |
| Total | 22.5±7.4 | 15.8±6.4 | <0.0001 | |
| Fat mass (kg) | Boys | 8.2±5.4 | 6.6±3.2b | <0.0001 |
| Girls | 11.9±7.4 | 10.2±4.4 | 0.131 | |
| Total | 10.7±7.0 | 7.2±3.6 | <0.0001 | |
| Lean mass (kg) | Boys | 35.3±11.3 | 39.8±10.5 | <0.0001 |
| Girls | 33.7±7.0 | 31.7±6.0 | 0.056 | |
| Total | 34.2±8.6 | 38.6±10.3 | <0.0001 | |
| Muscle mass (kg) | Boys | 33.4±10.8 | 37.5±10.1b | <0.0001 |
| Girls | 31.9±6.7 | 29.8±5.8 | 0.039 | |
| Total | 32.4±8.2 | 36.4±9.9 | <0.0001 | |
| Tricipital fold (mm) | Boys | 11.5±5.0 | 9.8±3.3b | <0.0001 |
| Girls | 16.9±5.2 | 16.8±4.5 | 0.901 | |
| Total | 15.2±5.7 | 10.9±4.3 | <0.0001 | |
| Subscapular fold (mm) | Boys | 10.2±5.8 | 8.3±3.2b | <0.0001 |
| Girls | 13.9±4.9 | 12.1±3.9 | 0.015 | |
| Total | 12.7±5.5 | 8.9±3.5 | <0.0001 | |
| Σ folds (mm) | Boys | 21.7±10.3 | 18.2±5.8b | <0.0001 |
| Girls | 30.8±9.2 | 28.9±8.0 | 0.173 | |
| Total | 27.9±10.5 | 19.7±7.3 | <0.0001 | |
| Body adiposity index (%) | Boys | 27.0±4.6 | 24.0±3.4 | <0.0001 |
| Girls | 28.3±3.6 | 27.0±3.7 | 0.019 | |
| Total | 27.9±4.0 | 24.5±3.6 | <0.0001 | |
| Waist circumference (cm) | Boys | 65.9±9.0 | 64.9±6.8 | 0.201 |
| Girls | 65.9±7.6 | 64.3±8.2 | 0.174 | |
| Total | 65.9±8.0 | 64.8±7.0 | 0.050 | |
| Hip circumference (cm) | Boys | 80.6±8.8 | 79.8±10.2 | 0.338 |
| Girls | 83.6±9.8 | 79.6±8.1 | 0.008 | |
| Total | 82.4±10.1 | 80.5±8.7 | 0.005 | |
Cardiorespiratory fitness level (unhealthy and healthy) was grouped according to the FITNESSGRAM reference criteria11. Data are given as mean±standard deviation.
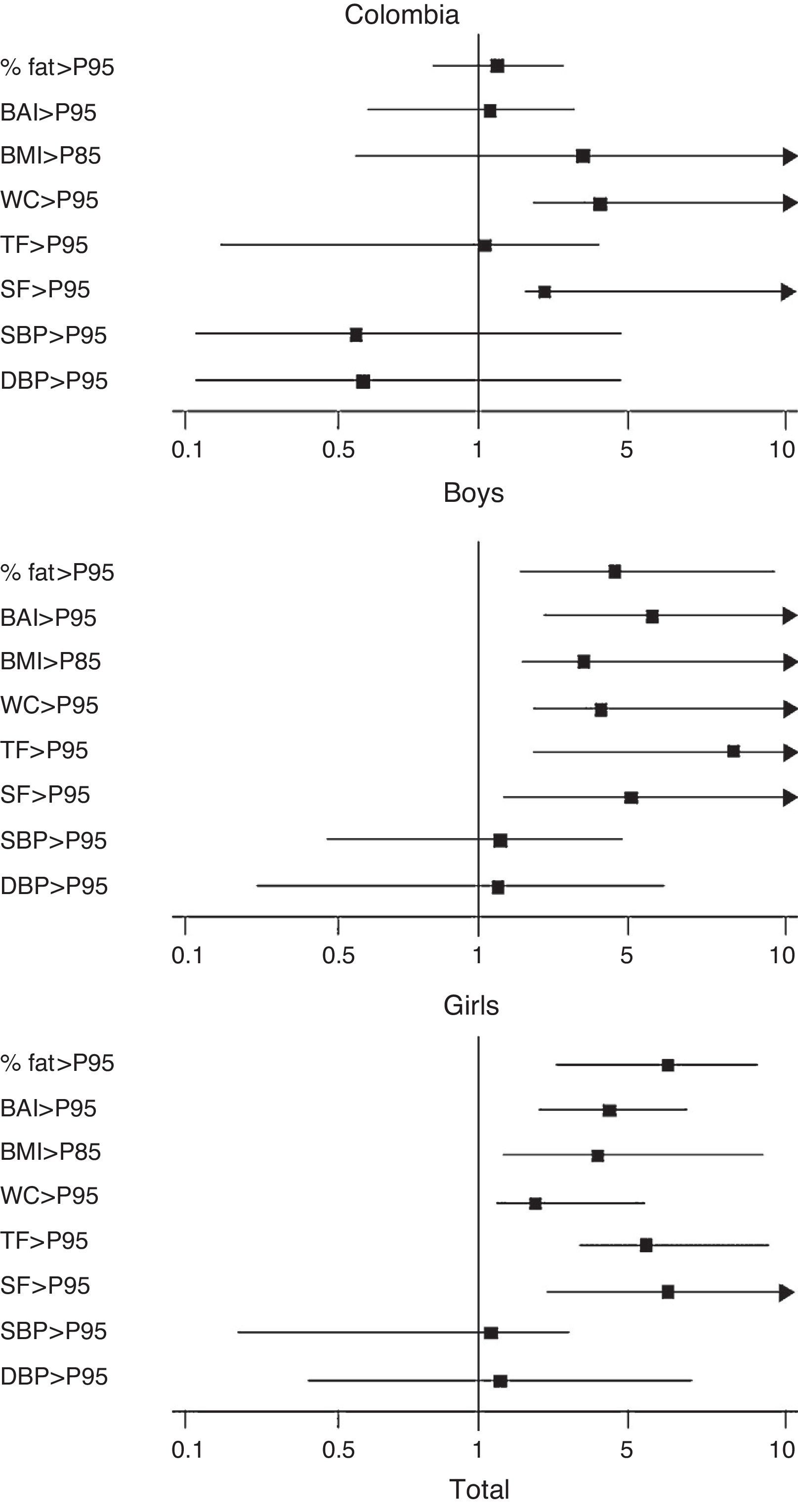
In the general population, after adjusting for age, sex, and maturation stage, schoolchildren with unhealthy CRF values according to the 2011 FITNESSGRAM classification had a 6.06-fold higher (95% CI 3.98–9.24) chance of showing an elevated percent body fat by bioimpedance, and 6.65-fold (95% CI 3.95–9.53) and 6.13-fold (95% CI 2.43–15.47) increases in subcutaneous body fat in the tricipital and subscapular folds respectively. They also had a 4.04-fold (95% CI 1.83–9.11) greater risk of overweight/obesity from elevated BMI, a 4.36-fold (95% CI 2.79–6.81) greater risk of high BAI, and 2.47 times (95% CI 1.14–5.37) more abdominal obesity as shown by increased WC. This observation was also made in girls, after adjusting for age and sexual maturation in the abovementioned variables, while in boys this only occurred in the variables of body composition and fat distribution by central obesity (odds ratio 4.18; 95% CI 1.62–10.80) and subscapular skinfold (odds ratio 5.03; 95% CI 1.82–13.89) (Fig. 1).

Predictive capacity of cardiorespiratory fitness with changes in variables of health status in schoolchildren from Bogotá, Colombia, by sex and overall. WC: waist circumference; BAI: body adiposity index; BMI: body mass index; SF: subscapular fold; TF: tricipital fold; P95: 95th percentile; DBP: diastolic blood pressure; SBP: systolic blood pressure; % fat: percent body fat.
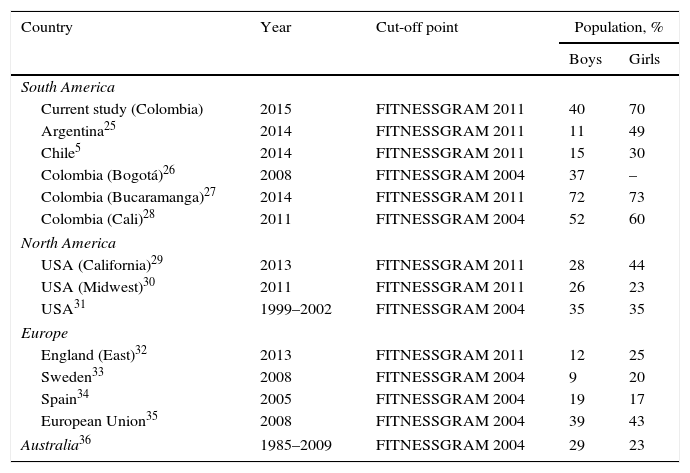
In this study, 66% of schoolchildren had low CRF levels based on FITNESSGRAM criteria (2011).11,24 A higher proportion (70%) was seen in girls. This is much higher than the proportions reported in South America by Garber et al.5 (30%) in Chilean schoolchildren and by Secchi et al.25 (49%) in Argentina, and similar to those reported by Cohen et at.27 (73%) and Aguilar et al.28 (60%) in Bucaramanga and Cali, Colombia, respectively. This value is also higher than those reported by Welk et al.30 (23%) and Pate et al.31 (35%) in North America, by Voss et al.32 (25%) in England, and by Ortega et al.35 (23%) in the European Union (Table 4). Based on these findings, it may be stated that approximately two thirds of the participants had an aerobic capacity level suggesting future cardiovascular risk.
Prevalence of unhealthy CRF among schoolchildren from Bogotá, Colombia, and in the quoted studies.
| Country | Year | Cut-off point | Population, % | |
|---|---|---|---|---|
| Boys | Girls | |||
| South America | ||||
| Current study (Colombia) | 2015 | FITNESSGRAM 2011 | 40 | 70 |
| Argentina25 | 2014 | FITNESSGRAM 2011 | 11 | 49 |
| Chile5 | 2014 | FITNESSGRAM 2011 | 15 | 30 |
| Colombia (Bogotá)26 | 2008 | FITNESSGRAM 2004 | 37 | – |
| Colombia (Bucaramanga)27 | 2014 | FITNESSGRAM 2011 | 72 | 73 |
| Colombia (Cali)28 | 2011 | FITNESSGRAM 2004 | 52 | 60 |
| North America | ||||
| USA (California)29 | 2013 | FITNESSGRAM 2011 | 28 | 44 |
| USA (Midwest)30 | 2011 | FITNESSGRAM 2011 | 26 | 23 |
| USA31 | 1999–2002 | FITNESSGRAM 2004 | 35 | 35 |
| Europe | ||||
| England (East)32 | 2013 | FITNESSGRAM 2011 | 12 | 25 |
| Sweden33 | 2008 | FITNESSGRAM 2004 | 9 | 20 |
| Spain34 | 2005 | FITNESSGRAM 2004 | 19 | 17 |
| European Union35 | 2008 | FITNESSGRAM 2004 | 39 | 43 |
| Australia36 | 1985–2009 | FITNESSGRAM 2004 | 29 | 23 |
However, the high overall prevalence–particularly in girls–of unhealthy CRF in this study is consistent with the growing body of evidence of epidemiological transition,37 built environment,38 and the double burden of malnutrition39 in the Colombian population. Changes in nutritional habits and physical activity levels are the most significant characteristics related to the accelerated economic transition experienced by developing countries in recent years. Urbanization is related to energy expenditure in activities of daily life due to the mechanization of such activities in the urban environment, but especially because of the mechanization of leisure activities, particularly in children, who have replaced traditional games requiring a lot of physical activity and energy expenditure with sedentary activities using electronic devices or just sitting in front of the TV set.40
In addition, the prevalence of sedentary lifestyles has increased. In the Americas, 43% of the population is sedentary. The prevalence of physical inactivity ranges from 17.0% in Guatemala to 70.9% in Argentina in women, and from 15.3% to 65.8% in men in these same countries.41 In Colombia, the prevalence of compliance with recommendations to perform moderate physical activity for 150min weekly was 53.5% in 2010.1
In 2007, according to the Global School-based Student Health Survey42 conducted in five Colombian cities, only 15% of adolescents aged 13–15 years were physically active. In all cities, the physical activity levels reported were higher in males. This is a consistent finding in international and national surveys on physical activity in schoolchildren, and has also been reported in adults in Bogotá.1,41 It also agrees with the results reported by Pate et al.31 in schoolchildren from North America. These authors considered four determinant levels–the physiological, psychological, sociocultural, and ecological–influencing physical activity. For example, the physiological determinants of physical activity among children and adolescents include age, sex, and ethnic group. Specifically, girls have been found to be less active than boys, older children and adolescents are less active than younger children, and girls of African descent are less active than those of European descent.9,15,16 Potential sex and sociocultural differences may in part explain the high prevalence of unhealthy CRF seen in girls in this study. Studies including the perceived barriers for physical activity, the ecological determinants of physical activity such as access to play spaces, facilities, equipment availability, dietary intake, smoking, and socioeconomic level are, however, needed if we are to fully understand the multitude of factors that may influence physical activity models in the schoolchildren evaluated.
As noted above, low CRF is considered to be a strong predictor of cardiovascular diseases, not only in overweight and obese subjects, but also in those with a healthy weight.5,9,25 In terms of health promotion and the prevention of cardiometabolic disease, low CRF is potentially pathological and represents for the subject a true independent risk of non-transmissible disease.5 In this regard, the coexistence of other cardiovascular risk factors was assessed in our study to show the predictive ability of CRF.
Data from this study showed that children and adolescents with healthy aerobic capacity had better overall values in the morphological and health components studied (Tables 3 and 4). They also had lower values in body adiposity markers such as percent fat, fat mass, and skinfolds, which are factors related to a better lipid and metabolic profile.25 As regards this finding, the Ortega et al. study33,34 showed an inverse correlation between CRF and changes in lipid metabolism, irrespective of physical activity levels, in the Feeding and nutritional status assessment in adolescents study (the AVENA study) conducted at five Spanish centers (Granada, Madrid, Murcia, Santander, and Saragossa), thus supporting the measurement of aerobic fitness as a potential additional measurement for predicting cardiometabolic risk in the school setting. This evidence assigns to physical education teachers the responsibility for promoting the health of their students. School is therefore a privileged space where healthy exercise habits can be encouraged and cardiovascular health preserved.25
This study has some limitations. For example, sample size, population characteristics, study design, and type of sampling may be considered as potential sources of bias. On the other hand, other variables that may be associated with a cardiometabolic risk profile, such as ethnicity, socioeconomic, nutritional and social aspects, and physical activity levels, were not included. Self-reporting of Tanner stage, despite its good correlation with direct measurement, can be considered another limitation of the study.22,23 Despite these limitations, there are no reasons for thinking that the relations described only occur in the population from which our sample comes, as the results were seen to agree with data reported in other national and international studies.3,5,6,8,13,14,25,27 Thus, we believe that these limitations do not compromise the results obtained in our study.
A strength of the study was the predictive capacity of the cut-off point proposed by the FITNESSGRAM group of the Cooper Institute11 used in the study, starting from well established cardiovascular risk thresholds for schoolchildren, estimating the impairment rate in the VO2max from childhood and adolescence, as well as the coexistence with other variables related to childhood obesity that could represent a cardiovascular risk at a later age. It should also be noted that this is one of the first studies conducted to date of a Latin population explicitly describing the conceptual framework in which the ALPHA-FITNESS battery may be applied13 (the motor and morphological components), together with measurements of adiposity and body fat components.
As a strategy for the epidemiological monitoring of fitness at school, this study showed a high prevalence of low CRF levels in schoolchildren according to FITNESSGRAM criteria.11 Despite its significance, this marker of metabolic and cardiovascular risk is not yet part of the evaluation protocol for schoolchildren and adolescents in the different regions of Colombia.
In conclusion, the authors recommend that the evaluation of CRF should be added to the standard measurement of other traditional risk factors in the prevention and treatment of risk factors associated with cardiometabolic disease at educational institutions in the Bogotá district. It is important that national programs and future interventions to promote higher physical activity levels in Colombia take into account the role of gender inequality, as well as its associated factors, in contributing to differences in health between the sexes. Observational studies with larger sample sizes, and especially longitudinal and prospective studies, are needed to confirm the results of this study.
FundingThis study is part of the FUPRECOL project (Association of Grip Strength with Early Manifestations of Cardiovascular Risk in Colombian Children and Adolescents) funded by the Administrative Department of Science, Technology, and Innovation Colciencias, Contract No. 122265743978.
Conflicts of interestThe authors state that they have no conflicts of interest.
Our special thanks to researchers from Universidad del Rosario (Center for Studies on the Measurement of Physical Activity) and Universidad Santo Tomás (Grupo CICAEDS) for technical support, training for the tests, and advice on field measurements. We thank the Vice-chancellorship of Universidad Manuela Beltrán for funding for field measurement equipment and for administrative support.
Please cite this article as: Gualteros JA, Torres JA, Umbarila-Espinosa LM, Rodríguez-Valero FJ, Ramírez-Vélez R. Una menor condición física aeróbica se asocia con alteraciones del estado de salud en niños y adolescentes de Bogotá, Colombia. Endocrinol Nutr. 2015;62:437–446.
