


Degludec is the most recent molecule of the ultra-long-acting basal insulin analogs approved for human use. It forms soluble multihexamers which after subcutaneous injection are converted into monomers, and are thus slowly and continuously absorbed into the bloodstream. This absorption mechanism confers degludec an ultra-long and stable action profile, with no concentration peaks. This paper discusses the most recent studies in patients with type 1 and 2 diabetes mellitus, which showed degludec to be non inferior in decreasing HbA1c, ensuring optimum glycemic control similar to that achieved with insulin glargine or detemir. Degludec also had an improved safety profile, as it was associated to a significantly lower rate of nocturnal hypoglycemia in both types of diabetes and to a potentially lower overall hypoglycemia rate in type 2 DM. Degludec also opens the possibility to use more flexible regimens.
Degludec es la última molécula de las insulinas basales de acción ultra-lenta aprobada para su uso en humanos. Forma multihexámeros solubles que tras la inyección subcutánea se transforman en monómeros que son absorbidos lenta y continuamente por la circulación sanguínea. Este mecanismo de acción le confiere un perfil de acción ultra-lento y estable, sin picos de concentración. En este trabajo se han recogido los últimos ensayos en pacientes con diabetes mellitus tipo1 y 2, en los que degludec demostró no-inferioridad en la disminución de la HbA1c asegurando un control óptimo de la glucemia de forma similar a como lo hicieron glargina o detemir. Además, presentó un perfil de seguridad mejorado, al estar asociado a una tasa significativamente inferior de hipoglucemias nocturnas en ambos tipos de diabetes y potencialmente de hipoglucemias globales en el tipo2. Degludec abre, además, la posibilidad de utilizar pautas con mayor flexibilidad.
Because of the high prevalence of diabetes mellitus (DM), estimated in 2011 at 366million people, or 8.3% of the worldwide population,1 this disease has acquired the characteristics of an epidemic. Insulin isolation in 1921 represented one of the most significant advances of the 21st century and opened up a wide field of research into the treatment of DM. The clinical use of purified insulins of animal origin in humans gave way to human insulin obtained by recombinant DNA techniques. These molecules have a wide pharmacokinetic variability, mainly in the absorption and duration of action, which causes concentration peaks that may contribute to the occurrence of hypoglycemia. Physiological insulin secretion has two components, a continuous basal component occurring between intakes and an acute component triggered by increased blood glucose. Ultra-long-acting basal insulin analogs, intended to produce a sustained blood glucose control, so reducing the risk of hypoglycemia, have been developed in recent years. The first insulins of this type, glargine and detemir, are today an essential tool in the management of patients with both type 1 (T1DM) and type 2 (T2DM) diabetes mellitus. They have been shown to provide optimum glucose control similar to that achieved with neutral protamine Hagedorn (NPH) insulin, with significantly less risk of hypoglycemia, particularly at night.2–4 These compounds are also characterized by a lower day-to-day variability in fasting plasma glucose levels.5–7 However, these insulins are not able to accurately mimic the basal secretion of endogenous insulin for longer than 24h, as would ideally be required in patients with T1DM. Insulin degludec has been formulated to form soluble multihexamer complexes which after subcutaneous injection produce monomer deposits which are slowly absorbed by the bloodstream.8 This unique mechanism of action confers on insulin degludec a flat, stable pharmacokinetic profile with an elimination half-life longer than 25h and a duration of action longer than 40h.8,9 This review article discusses the most recent studies supporting the non-inferiority of insulin degludec as compared to the standard treatment for blood glucose control in patients with T1DM and T2DM, as well as confirming its benefits for reducing the risk of hypoglycemia. The safety profile of insulin degludec seen in phase III of the clinical development of this new ultra-long-acting basal insulin analog is also reported on.
Clinical advances in the study of degludec in type 1 diabetesIn T1DM, in addition to sustained exogenous insulin support to ensure the achievement of basal levels, a bolus of fast-acting insulin is required to manage hyperglycemia generated during meals. The complexity and lack of flexibility of insulin regimens, patient resistance to the administration of multiple insulin doses, and the fear of hypoglycemia often have an impact on treatment adherence and efficacy, and also on health-related quality of life.10–12 In a phase II exploratory study, combined therapy with degludec and fast-acting insulin aspart achieved a 28% greater reduction in the risk of hypoglycemia and up to a 58% greater reduction in nocturnal hypoglycemia as compared to the combination of degludec with glargine, while blood glucose control was similar with both insulin regimens at 16 weeks of treatment.13,14 The safety profile was also similar, even when weight increase was studied. A substudy of the above study assessed quality of life of patients based on the SF-36 health survey and found a significant improvement in the everyday social life and mental health of patients who had been administered the combination containing degludec. Although additional studies are needed, these results may be related to the reduction of the risk of hypoglycemia.15
Based on these results, phase II of the clinical development of this new basal insulin analog with an ultra-long-action in T1DM was started. The efficacy results and the hypoglycemia rate found with degludec are shown in Tables 1 and 2 respectively. A randomized, controlled, parallel, open label, multicenter study BEGIN Basal-Bolus Type 1 assessed the efficacy and safety of the administration of insulin degludec or glargine during 52 weeks of follow-up.16 A total of 629 adult patients with T1DM were randomized in a 3:1 ratio to receive the new insulin analog or insulin glargine once daily, both combined with insulin aspart during meals. Insulin doses were adjusted to achieve a control goal of fasting blood glucose (FBG) of 70–90mg/dL. The primary study objective was a reduction in HbA1c at week 52. The results showed the non-inferiority of degludec in glucose control, with a difference of 0.40% for degludec and 0.39% for glargine (−0.01%; 95% confidence interval (CI): −0.14 to 0.11; p<0.0001 for the non-inferiority trial). In addition, no significant differences were found regarding decreases in FBG, with an estimated difference between the treatments of −5.94mg/dL) (95% CI: −18.54 to 6.48; p=0.35). The decrease in glycemic profiles by 9 points detected during the 52 weeks of treatment was also similar between both insulin therapies, and blood glucose was significantly lower before breakfast with degludec only (−9.9mg/dL; 95% CI: −18.54 to −1.44; p=0.023). The overall confirmed hypoglycemia rate was similar between the groups both in the first phase of follow-up and during the maintenance period (from week 16 to week 52). However, a decrease was seen in the nocturnal hypoglycemia rate, which was significantly lower in the experimental group with degludec throughout the study follow-up (rate by patient-year of exposure: 4.41 vs 5.86; estimated rate ratio [ERR]: 0.75; 95% CI: 0.59–0.96; p=0.021). The incidence of serious and non-serious adverse effects was very similar for both insulin regimens.
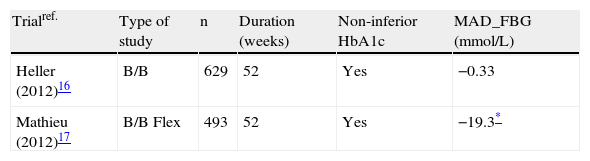
Efficacy of degludec vs glargine in phase III clinical development in patients with type 1 diabetes mellitus.
| Trialref. | Type of study | n | Duration (weeks) | Non-inferior HbA1c | MAD_FBG (mmol/L) |
| Heller (2012)16 | B/B | 629 | 52 | Yes | −0.33 |
| Mathieu (2012)17 | B/B Flex | 493 | 52 | Yes | −19.3* |
B/B: basal-bolus; MAD_FBG: mean adjusted difference in fasting blood glucose [degludec–glargine]; Flex: degludec Flex (8–40h intervals) vs glargine; Yes: the hypothesis of the non-inferiority of degludec vs glargine is confirmed (Δ≤4%).
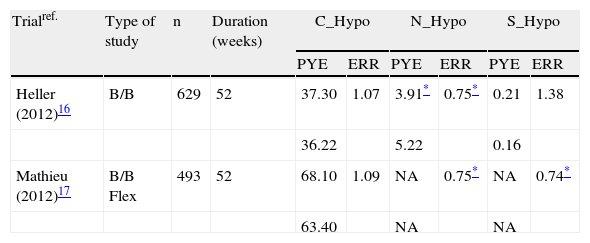
Hypoglycemia rate with degludec vs glargine in phase III clinical development in patients with type 1 diabetes mellitus.
| Trialref. | Type of study | n | Duration (weeks) | C_Hypo | N_Hypo | S_Hypo | |||
| PYE | ERR | PYE | ERR | PYE | ERR | ||||
| Heller (2012)16 | B/B | 629 | 52 | 37.30 | 1.07 | 3.91* | 0.75* | 0.21 | 1.38 |
| 36.22 | 5.22 | 0.16 | |||||||
| Mathieu (2012)17 | B/B Flex | 493 | 52 | 68.10 | 1.09 | NA | 0.75* | NA | 0.74* |
| 63.40 | NA | NA | |||||||
B/B: basal-bolus; Flex: degludec Flex (8–40h intervals); C_Hypo: confirmed hypoglycemia; N_Hypo: nocturnal hypoglycemia; S_Hypo: severe hypoglycemia; NA: information not available: PYE: rate of episodes by patient-year of exposure; ERR: estimated rate ratio [degludec/glargine].
To date, maintaining a fixed time for the daily injection of basal insulin has been considered indispensable for ensuring stable blood glucose control. An increased flexibility in basal insulin administration may be an added advantage for diabetic patients by allowing them to adapt the injection time to their individual daily needs. The results of a multicenter, randomized, open-label, 52-week study, BEGIN Flex Type 1, comparing the efficacy and safety of degludec, administered in a flexible regimen, and glargine administered according to the prescribing information were recently reported at a congress.17 In the first phase of 26weeks of the study, the patients self-administered degludec once daily at the same time of day (n=165) or in a flexible regimen with dosing intervals ranging from 8 to 40h (n=164). In the extension phase of this study, all the patients were pooled in a single group on a flexible regimen of degludec (n=329) to be compared to glargine (n=164). The results at 52weeks demonstrated non-inferiority, with decreases in basal HbA1c of 0.13% and 0.21% in the group given degludec on a flexible regimen and the glargine group respectively (estimated difference between the groups: 0.07%; 95% CI: −0.05 to 0.19). The decrease in FGB was significantly greater with degludec in a flexible regimen, with an estimated difference from glargine of −19.3mg/dL) (−32.7 to −5.8; p=0.005). The overall hypoglycemia rate (patient-year of exposure) was similar for degludec and glargine (68.1 vs 63.4 respectively). ERR: 1.09; 95% CI: 0.91–1.29; p=not significant [NS]). However, the group on degludec in a flexible regimen showed a statistically significant 25% decrease in nocturnal hypoglycemia (ERR: 0.75; 95% CI: 0.58–0.97; p=0.025) and 26% less severe hypoglycemic episodes (ERR: 0.74; 95% CI: 0.38–1.42; p=NS). A similar adverse effect rate was reported for both study groups.
Clinical advances in the study of degludec in type 2 diabetesIn patients with T2DM, initial drug treatment usually consists of oral antidiabetic drugs (OADs), in addition to the recommendations regarding exercise and diet which are standard in DM. However, because of progressive cell dysfunction β, insulin therapy is required if control goals are not achieved. Some studies suggest that insulin therapy is usually required in these patients approximately 9 years after diagnosis.18 In a phase II trial, the addition of insulin degludec administered once daily together with oral metformin therapy achieved adequate blood glucose control in patients with T2DM and was associated with a lower incidence of hypoglycemia as compared to glargine therapy (although the difference was not statistically significant).19
The phase III studies in patients with T2DM, which are summarized in Tables 3 and 4, started with a multicenter, randomized, controlled, open label study with 52weeks of follow-up enrolling patients with T2DM not previously receiving insulin but who could be treated with OADs (metformin±dipeptidyl-peptidase-4 [DPP-4] inhibitors).20 The results showed the non-inferiority in efficacy of degludec as compared to glargine, with an estimated difference in HbA1 decrease between both groups of 0.09% (95% CI: −0.04–0.22) and an estimated statistically significant difference in FBG between the groups of −7.74mg/dL (p=0.005) favoring degludec. The overall confirmed hypoglycemia rate was similar in both groups. However, the risk of severe nocturnal hypoglycemia was significantly lower with degludec (rate of nocturnal episodes by patient-year of exposure: 0.25 vs 0.39; ERR: 0.64; 95% CI: 0.42–0.98; p=0.038, and by rate of severe episodes: 0.003 vs 0.023; ERR: 0.14; 95% CI: 0.03–0.70; p=0.017). No significant differences were seen in adverse event rate or weight gain between the two treatments.
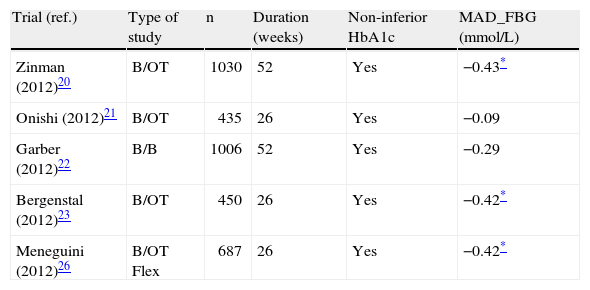
Efficacy of degludec vs glargine in phase III clinical development in patients with type 2 diabetes mellitus.
| Trial (ref.) | Type of study | n | Duration (weeks) | Non-inferior HbA1c | MAD_FBG (mmol/L) |
| Zinman (2012)20 | B/OT | 1030 | 52 | Yes | −0.43* |
| Onishi (2012)21 | B/OT | 435 | 26 | Yes | −0.09 |
| Garber (2012)22 | B/B | 1006 | 52 | Yes | −0.29 |
| Bergenstal (2012)23 | B/OT | 450 | 26 | Yes | −0.42* |
| Meneguini (2012)26 | B/OT Flex | 687 | 26 | Yes | −0.42* |
B/B: basal-bolus; B/OT: basal-oral therapy; MAD_FBG: mean adjusted difference in fasting blood glucose [degludec–glargine]; Flex: degludec Flex (8–40h intervals) vs glargine; HbA1c: glycosylated hemoglobin; Yes: the hypothesis of the non-inferiority of degludec vs glargine is confirmed (Δ≤4%).
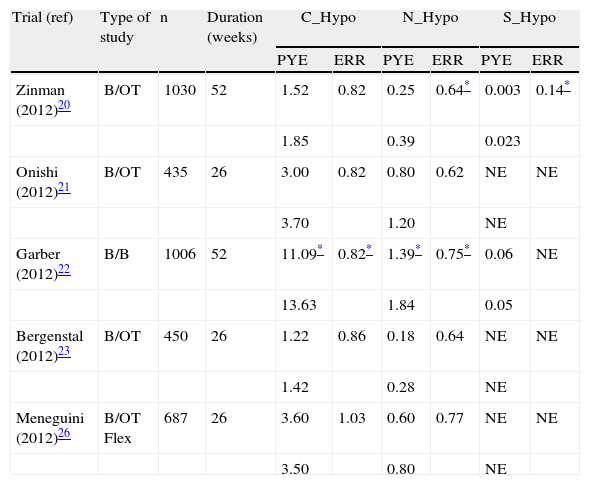
Hypoglycemia rate recorded with degludec vs glargine in phase III clinical development in patients with type 2 diabetes mellitus.
| Trial (ref) | Type of study | n | Duration (weeks) | C_Hypo | N_Hypo | S_Hypo | |||
| PYE | ERR | PYE | ERR | PYE | ERR | ||||
| Zinman (2012)20 | B/OT | 1030 | 52 | 1.52 | 0.82 | 0.25 | 0.64* | 0.003 | 0.14* |
| 1.85 | 0.39 | 0.023 | |||||||
| Onishi (2012)21 | B/OT | 435 | 26 | 3.00 | 0.82 | 0.80 | 0.62 | NE | NE |
| 3.70 | 1.20 | NE | |||||||
| Garber (2012)22 | B/B | 1006 | 52 | 11.09* | 0.82* | 1.39* | 0.75* | 0.06 | NE |
| 13.63 | 1.84 | 0.05 | |||||||
| Bergenstal (2012)23 | B/OT | 450 | 26 | 1.22 | 0.86 | 0.18 | 0.64 | NE | NE |
| 1.42 | 0.28 | NE | |||||||
| Meneguini (2012)26 | B/OT Flex | 687 | 26 | 3.60 | 1.03 | 0.60 | 0.77 | NE | NE |
| 3.50 | 0.80 | NE | |||||||
B/B: basal-bolus; B/OT: basal-oral therapy; Flex: degludec Flex (8–40h intervals); C_Hypo: confirmed hypoglycemia; N_Hypo: nocturnal hypoglycemia; S_Hypo: severe hypoglycemia; NE: not sufficient events for analysis; PYE: rate of episodes by patient-year of exposure; ERR: estimated rate ratio [degludec/glargine].
An additional study in an Asian population enrolled patients with T2DM not previously given insulin therapy but who could be on stable OAD treatment (n=435).21 The patients in both groups showed similar decreases in HbA1c (degludec: 1.24%; glargine: 1.35%) and FBG (99.9 and 101.8mg/dL respectively). The overall confirmed hypoglycemia rate was 18% lower in the degludec group at 26weeks of follow-up and 37% lower in the maintenance phase (after week 16 of the study), but the difference was not statistically significant. With degludec, the confirmed nocturnal hypoglycemia rate also decreased by 38%. There were 0.8 episodes by patient-year with degludec, as compared to 1.2 episodes with glargine (p=NS). This reduction increased to 48% in the maintenance phase (from week 16), but this increase was not statistically significant. The safety profile of both insulin regimens was similar, including weight increase.
Treatment intensification by administering a basal-bolus regimen was assessed in the BEGIN Basal-Bolus Type 2 study in a population of 1.006 adult patients with T2DM. This study analyzed the efficacy and safety of a once daily administration of degludec or glargine (in a 3:1 ratio) for 52weeks. An oral regimen with metformine and/or pioglitazone could be maintained.22 Basal insulin was adjusted based on a FBG value of 70–90mg/dL. An analysis of the primary study endpoint confirmed the non-inferiority of degludec in HbA1c reduction at 52weeks, with mean differences from baseline of −1.10% for degludec and −1.18% for glargine (0.08%; 95% CI: −0.05 to 0.21; p=NS). No significant differences were seen in the proportion of patients who achieved an HbA1c<7% (degludec 49% vs glargine 50%), in the decrease in FBG levels, or in the reduction in nine-point blood glucose profiles. By contrast, the overall confirmed hypoglycemia rate (expressed as rate by patient-year of exposure) was significantly lower in the degludec as compared to the glargine group (11.1 vs 13.6 respectively. ERR: 0.82: 95% CI: 0.69–0.99; p=0.0359; 18% risk reduction). A lower confirmed nocturnal hypoglycemia rate was also found (1.4 vs 1.8 respectively. ERR: 0.75: 95% CI: 0.58–0.99; p=0.0399; 25% risk reduction). These data were confirmed in the analysis of the maintenance period (weeks 16–52). The incidence of severe hypoglycemic episodes was low in both groups, with no significant differences between them. On the other hand, degludec had a safety profile similar to glargine, with similar rates of serious and non-serious adverse events between both groups. In addition, data from the SF-36 health survey showed an improvement in the bodily pain component after treatment with degludec (p=0.032).
Current insulin administration systems allow maximum doses of 80IU of insulin to be given, but up to 20–30% of patients have been seen to require higher doses. Therefore, in order to be able to administer higher insulin doses as a single injection (up to 160IU), a formulation containing degludec 200IU/mL was tested in an open label, controlled, intention-to-treat study lasting 26weeks.23 Combined treatment with degludec and OAD was non-inferior in efficacy to glargine and OAD, with a similar 1.3% decrease in HbA1c. By contrast, the reduction in FBG values was significantly higher in the degludec group (−7.59mg/dL; p=0.02). Overall and nocturnal confirmed hypoglycemia rates by patient and year of exposure were also lower for degludec, but the difference was not statistically significant. The incidence of adverse events was similar with the 200IU/mL formulation of degludec and glargine. A substudy of the previous study assessed health-related quality of life with the 200IU/mL formulation of degludec compared to glargine in patients with T2DM treated with OADs.24 Based on the changes recorded in the results of the SF-36 questionnaire after the 26weeks of the study, the physical and mental health components were overall similar for both treatments. However, significant improvements in the bodily pain and vitality domains were only seen with degludec (1.6 [0.1–3.2] and 1.5 [0.1–3.0 respectively).
The possibility of implementing a flexible dosing regimen of degludec, with an 8–40h interval between injections, was also assessed in patients with T2DM. A phase II study concluded that the flexible dosing regimen of degludec ensured optimum blood glucose control (non-inferiority in the study of HbA1c reduction at 16weeks of treatment) and a similar hypoglycemia rate as compared to degludec once daily or glargine.25 A phase III multicenter, randomized, controlled, parallel, open label trial with 26weeks of follow-up recruited 459adult patients with T2DM who were administered insulin degludec in a fixed or flexible regimen or glargine in a 1:1:1 ratio.26 Treatment with OADs (metformin, pioglitazone, or sulfonylureas) was also allowed at the discretion of the physician. The basal insulin dose was adjusted to achieve a FBG value of 70–90mg/dL. The experimental group on a flexible degludec regimen showed non-inferiority to the fixed regimen at 26weeks of treatment. The estimated difference between the treatments in FBG at study end was significantly lower for the degludec flexible regimen as compared to glargine (−7.56mg/dL; p<0.05); by contrast, no significant differences were seen between flexible or fixed dosing. The overall confirmed hypoglycemia rate was similar in all three groups. A 23% decrease was only seen in the nocturnal hypoglycemia rate in the group on a flexible degludec regimen as compared to the glargine group (event rate by patient-year: 0.6 vs 0.8; ERR: 0.77; 95% CI: 0.44–1.35; p=NS), but this rate was 18% higher than that seen in the group on a fixed degludec regimen (p=NS). Safety data showed a similar adverse event rate in all three groups, as well as a similar weight gain.
Future of degludec: ongoing studiesThe new ultra-long-acting basal insulin analog, degludec, is being tested in several ongoing studies as part of an extensive clinical development program. One of the greatest limitations currently faced by patients and clinicians in DM is the occurrence of hypoglycemic episodes, usually associated with insulin therapy. Based on the potential advantages with regard to the risk of hypoglycemia provided by the pharmacological characteristics of degludec, a number of clinical trials have been started to accumulate greater experience and to verify the safety profile of degludec. These trials are planned to be completed in 2013. Ongoing studies include a study on the risk of hypoglycemia during exercise and evaluation of the effect of hypoglycemia on sleep quality, cognitive function, or brain activation in patients treated with degludec. The US Food and Drug Administration (FDA) has also requested the conduct of a study assessing the cardiovascular safety of degludec.
At the time of publication, degludec has been approved in Japan and Europe for the treatment of patients with T1DM and T2DM.
ConclusionsBased on the results of the most recent phase III clinical trials available, treatment with degludec, a new ultra-long-acting basal insulin analog, has additional safety benefits over the already available therapeutic agents. A lower nocturnal hypoglycemia rate has been seen in patients with both types of DM, and there is evidence of a decreased overall confirmed hypoglycemia rate in patients with T2DM. It should be noted, however, that these were open label studies which mainly used glargine as comparator and were sponsored by the manufacturing company.
Degludec has a flat pharmacokinetic profile and a long half-life which implies less variability, a significant reduction in the risk of hypoglycemia, and flexible dosing. These characteristics may promote treatment compliance and improve the efficacy of insulin regimens in patients with T1DM and T2DM: The possibility of combined formulations with fast-acting analogs is an added advantage that is being evaluated in clinical trials.
Conflicts of interestThe author has participated in counseling to Novo Nordisk, Lilly, AMGEN, AbbVie, and MSD, has been an investigator in clinical trials on degludec and degludec plus (Novo Nordisk), and has received fees for lectures organized by Lilly-Boehringer Ingelheim, Novo Nordisk, MSD, FAES, Novartis, and GSK.
The author thanks Irantzu Izco-Basurko and Teresa Hernando (COCIENTE S.L.) for their support in the writing of this manuscript. This assistance was funded by Novo Nordisk Pharma S.A., which also reviewed the accuracy of the information provided in this manuscript.
Please cite this article as: Muñoz Torres M. Degludec, una nueva insulina basal de acción ultra-lenta para el tratamiento de la diabetes tipo 1 y 2: avances en investigación clínica. Endocrinol Nutr. 2014;61:153–159.
