


The relationship of vitamin D deficiency to bone problems of rickets and osteomalacia has been known for decades. There is, however, increasing scientific evidence associating vitamin D deficiency with other pathological conditions such as different tumor types (mainly colon, breast, and prostate tumors), immune conditions (especially multiple sclerosis), metabolic syndrome-insulin resistance, cardiovascular disease, infections (particularly tuberculosis), muscle changes, and falls.1–5 An increasing number of authors, therefore, recommend the monitoring of vitamin D levels and the maintenance of adequate levels in order to prevent such associations.
The question remains, however, as to what the adequate levels required to prevent such associations actually are. While 25(OH)D3 levels less than 10ng/mL are known to be associated with known bone problems, the recommended 25(OH)D3 levels for protection against the previously listed associations have not been established with any exactitude. Some authors recommend 30ng/mL,6 but the Institute of Medicine recently stated that 20ng/mL levels could be considered adequate, based on current evidence.7
Vitamin D levels are influenced by latitude and the season of the year, and also by race, but irrespective of this, it is obvious that levels are increasingly lower in widely studied populations such as the US population.8 In Spain, as with neighbouring countries, there is a large population with decreased vitamin D levels.9
The purpose of our study was to ascertain vitamin D levels in a small population in Galicia and their relationship with obesity.
Ninety-five patients attending the outpatient clinics of a tertiary hospital in the summer of 2010 (from June to August) were studied. The study was approved by the ethics committee of the hospital and data were accessed in agreement with hospital protocols. The patients attended for different reasons, but none of them had parathyroid disease, absorption disorders, renal disease, or any other underlying disease that could affect vitamin D metabolism. They were not taking supplements or drugs that could influence calcium/vitamin D metabolism. Measurements included 25(OH)D3, PTH, and body mass index (BMI), calculated as weight in kilograms divided by height in meters squared, in order to test vitamin D levels, the proportion of patients with vitamin D deficiency and insufficiency, and the relationship between vitamin D and BMI. SPSS software was used. The correlation coefficient was determined using a linear regression test (Pearson) between vitamin D levels and BMI.
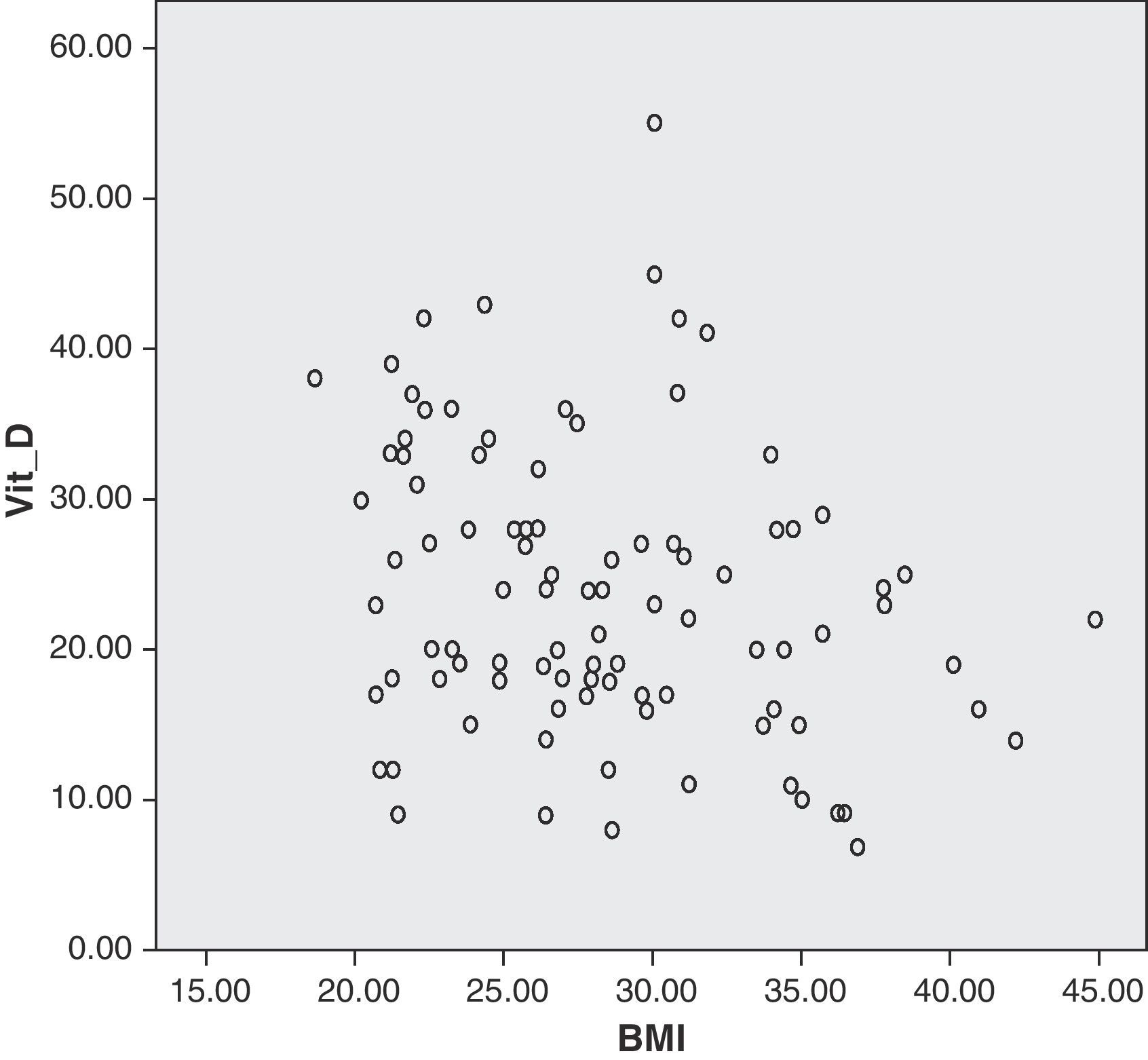
Mean patient age was 48.67 years (15–77 years), mean vitamin D level was 23.77ng/mL (7–55ng/mL), and mean BMI was 25.77kg/m2 (18.65–44.9kg/m2). Seventy-three patients (76.8%) had levels less than 30ng/mL, and 41 patients (44%) had levels less than 20ng/mL. This means that at least almost half the patients (or three quarters of them, depending on the cut-off point considered) had vitamin D deficiency.
There was a statistically significant negative correlation (R=−0.254, Pearson's test) between vitamin D levels and BMI (Fig. 1).

Although this was a small sample, a substantial vitamin D deficiency was found in this population. Multiple factors are involved in vitamin D levels. Vitamin D levels are higher in summer months due to greater exposure to ultraviolet rays as the result of exposure to the sun. Our population had a significant deficiency despite the fact that the data were collected in summer. These results are similar to those reported by larger and more significant studies8, and should be taken into account in our daily clinical practice.
The potential reasons for the current endemic vitamin D deficiency/insufficiency may include a lifestyle in which people spend more hours in closed spaces, live more frequently in urban rather than open spaces, use sun protection creams, and are increasingly obese.8 A statistically significant inverse correlation exists between vitamin D deficiency and overweight and obese patients. This is a situation already known and reported in other studies, particularly in patients with morbid obesity.10
Considering the benefits of adequate vitamin D levels for bone health and the fact that life expectation is increasingly longer, we should be aware of this situation. We, therefore, think that because of the prevalent and increasingly common occurrence of vitamin D deficiency in the general population, we should be more alert in its detection, particularly in populations which are more likely to have this deficiency because of their lifestyles and which are more prone to it, such as overweight and obesity patients.
ConclusionsVitamin D deficiency occurred in this population just as in other Caucasian populations and also in relation to obesity. It should be taken into consideration in our daily clinical practice.
Conflicts of interestThe authors state that they have no conflicts of interest.
Please cite this article as: Lorenzo J, et al. Déficit de vitamina D y obesidad. Endocrinol Nutr. 2012;59:401–2.
