


Introducción: No existen datos en la literatura médica provenientes de algún país latinoamericano, en relación con la calidad de la preparación para colonoscopia. El objetivo del presente estudio fue describir la calidad de la preparación colónica para el estudio de colonoscopia, obtenida con el uso de polietilenglicol (PEG) a dosis altas (4 litros), de acuerdo a la escala de Boston.
Material y métodos: Se realizó un estudio prospectivo de pacientes consecutivos evaluados, de octubre del 2011 hasta abril del 2012.
Resultados: Se incluyeron 835 pacientes, de los cuales 516 (61.8%) fueron mujeres. La media ± DE para la edad fue 58.3 15.2 años. Un total de 607 (72.7%) fueron provenientes del centro mexicano. La preparación colónica se catalogó como buena/ excelente en el colon derecho, colon transverso y colon izquierdo en 80.7%, 87.1% y 84.7% de los casos, respectivamente.
Conclusiones: La preparación con PEG-4 L es una buena opción para la preparación del colon, en pacientes que serán sometidos a colonoscopia.
Introduction: There is no data about quality bowel preparation from Latin-American centers. The aim of this study was to evaluate quality of colonic preparation with polyethylene glycol (PEG)-based solutions with large volumes (4 L) according to Boston bowel preparation scale in two different centers from Latin-American.
Material and methods: A prospective study was conducted. Consecutive patients evaluated during the period from October 2011 to April 2012 were included.
Results: Eight hundred thirty five patients were included; 516 (61.8%) were female. The mean SD of age was 58.3 15.2 years. A total of 607 (72.7%) patients were from Mexican center. Good/excellent (2/3 points) quality of preparation in right colon, transverse colon, and left colon was present in 80.7%, 87.1%, and 84.7%, respectively.
Conclusion: Quality of bowel preparation with PEG-based solutions with 4-L is a good option in patients whom will be undergone to colonoscopy.
Introduction
Adequate bowel cleansing is an important determinant of the efficacy of colonoscopy. Polyethylene glycol (PEG)-based solutions with large volumes (4 L) is used commonly in our media. Until 20% of colonoscopies have an inadequate preparation which is defined as "preparation when is not possible to detect polyps < 5 mm".1 Quality of bowel preparation must be evaluated always in the written report of colonoscopy procedure.2 Unfortunately, because many score systems, bowel-cleaning evaluation´s is not uniform. The scores used most often are: Aronchick, Ottawa and Boston bowel preparation scales.3 Until our knowledge, there are not previous reports about quality bowel preparation from a Latin-American centers.
The aim of this study was to evaluate quality of bowel preparation with 4-L PEG solution for colonoscopy according to Boston bowel preparation scale in two different centers from Latin-American.
Material and methods
This is a prospective study with two different centers. Patients undergoing colonoscopy for any indication at the Instituto Nacional de Ciencias Médicas y Nutrición "Salvador Zubirán" (Center A) Mexico City, Mexico, and the Hospital Las Américas (Center B), Guatemala City, Guatemala, during the period from October 2011 to April 2012 and to give informed consent. The protocol was reviewed and accepted by the Ethics Committee of the participating institutes. Were excluded patients who did not wish to participate in the study.
Colonoscopy was carried out under conscious sedation by specialist in anesthesiology, with the presence of continuous monitoring of vital signs, oxygen saturation and ECG tracing through automatic and assisted by nurses trained in endoscopic procedures, and management supplemental oxygen after standard preparation and which is conducted independently of this study, we performed the colonoscopy procedure according to standard recommendations, emphasizing lasting at least seven minutes during withdrawal maneuver.
The preparation for intestinal cleaning was made by administration of PEG (Nulytely®, Asofarma de México, México) as follow: one envelop diluted on 1 liter of drinking water in one hour (total four envelopes in four hours) the day previous of the study. Colonoscopy was carried out with standard equipment (CFQ 140-180L Olympus®, USA). Scope was advanced until cecum was identified by their anatomical characteristics (ileocecal valve, appendiceal orifice and tapeworms colonic junction). During the withdrawal all colonic segments were assessed (cecum, ascending colon, transverse colon, descending colon, sigmoid colon and rectum) in not less than seven minutes. Quality of colonic preparation was assessed by the Boston bowel preparation scale.4
A different person to who undertake the study of colonoscopy performed the data capture. All polyps measuring 5 mm or more were removed by snare polypectomy and submitted for histopathologic analysis. Endoscopic measurement of the polyp size was first made using a biopsy forceps.
Statistical analysis
The demographic and clinical characteristics were summarized with means, medians and standard deviations. To assess whether there were differences in relation to the characteristics of the patients according to the center of origin, the number of lesions detected was tested with t-test and X2 test according to variable type evaluated. A p value (α) of < 0.05 was considered significant. All statistical analyses were conducted using the statistics program SPSS version 20 (Chicago, IL, USA).
Results
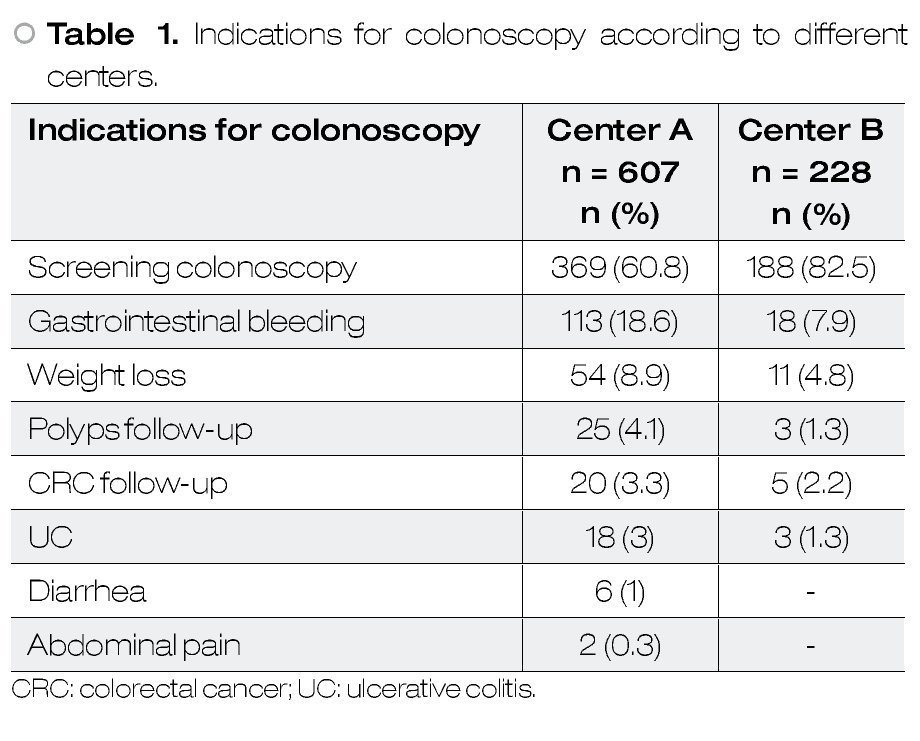
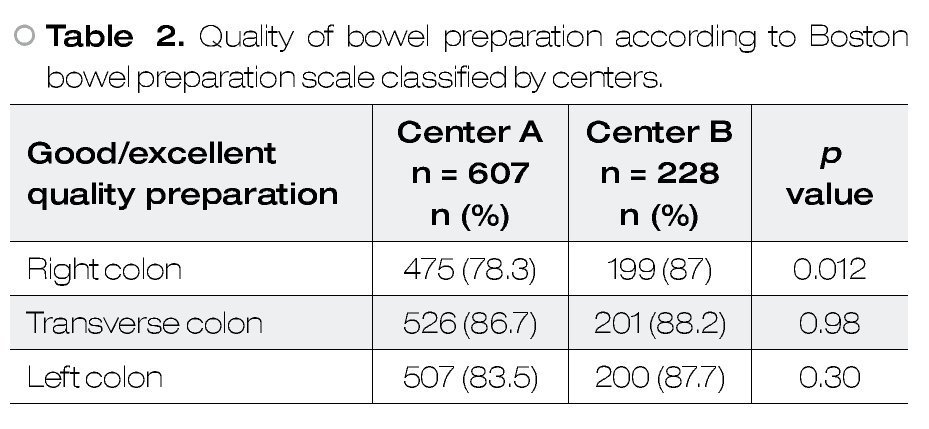
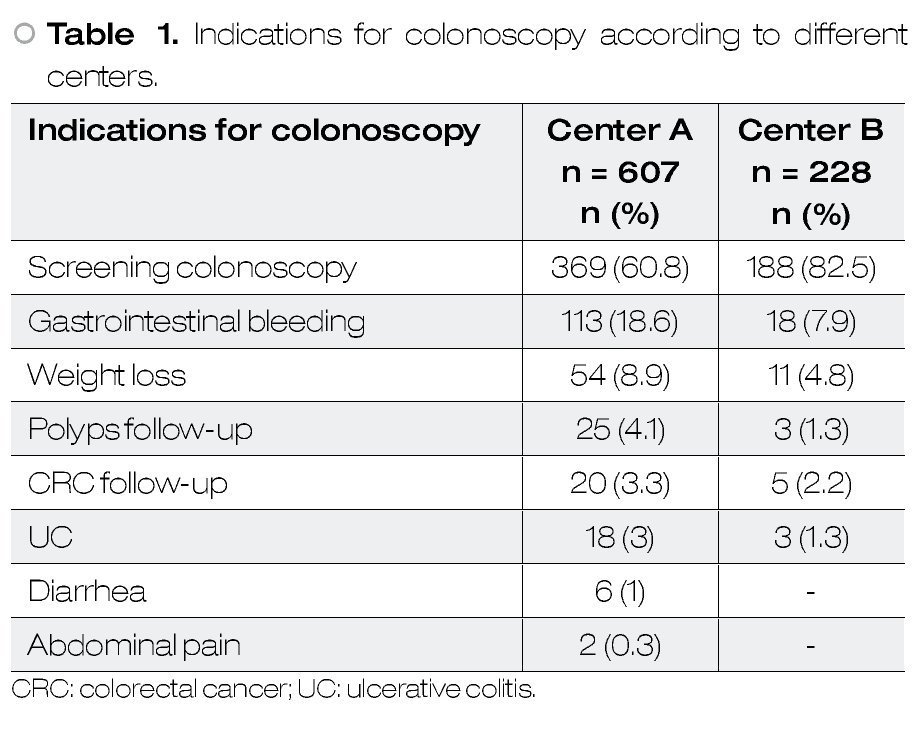
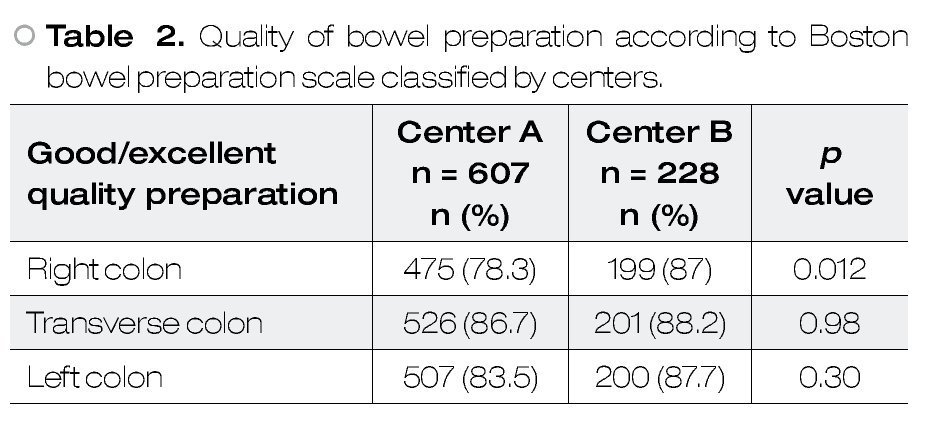
A total of 835 patients were included and 516 (61.8%) were female and 319 (38.2%) were male. The mean SD of age was 58.3 15.2 years. The number of patients included in each center was: Center A = 607 (72.7%), and Center B = 228 (27.3%) patients. Indications for colonoscopy classified by different centers are shown in Table 1. Good/excellent (2/3 points) quality of preparation in right colon, transverse colon, and left colon was present in 80.7%, 87.1%, and 84.7%, respectively. Data classified by centers are shown in Table 2.
Complications
There were three (0.3%) patients with minor complications. Anyone required endoscopic treatment. All three cases consisted of erosions with minor bleed spontaneously resolved. No cases of rectal perforation were seen in this study.
Discussion
In our media, colon bowel preparation with PEG-based solutions with large volumes (4-L) is a good option in patients whom will be undergone to colonoscopy. Previous reports from different countries conclude that colon bowel preparation with PEG-based solutions with large volumes is good option; however there is not data from Latin-American countries.
Regardless these positive results, we have to consider that actually, there are some studies that have studied different options about the total volume of PEG-based solutions, and split dose (2 liters PEG day before procedure followed by another 2 liters PEG same day of procedure) are the best option.5-8 We think that studies to evaluate different doses of PEG-solution must be done in our countries: split dose, PEG-low-volume solutions, etc.
Some limitations of this study must be considered; 1) we did not considered the time between the final PEG-dose and the time of colonoscopy procedure; 2) diet was not evaluated; and 3) in-hospital and out-patients were included. There are previous data regarding the importance of time for predict an inadequate colonic preparation.5,6 There are some studies that showed that a liquid diet and with low-residue have a good impact in the quality of bowel cleaning.9 Traditionally in our center, in-hospital patients are evaluated in colonoscopy room at the end of the day (with the idea that they are in-hospital and that is easier to call them any time), because of that, these group of patients commonly have more time since the end of the bowel preparation.
In conclusion, quality of bowel preparation with PEG-based solutions with 4-L is good in patients whom will be undergone to colonoscopy.
Conflict of interest
All authors declare no financial disclosures.
Financial support
This study was supported partially (donation of PEG preparation for Mexican patients) by a grant of Laboratorios Asofarma, S.A. de C.V.
Correspondence:
Félix Ignacio Téllez-Ávila, Ph.D.
Endoscopy Department, Instituto Nacional de Ciencias Médicas y Nutrición "Salvador Zubirán".
Vasco de Quiroga 15, Tlalpan, Z.P. 14000.
Phone: (525) 554870900, ext. 2150.
E-mail: felixtelleza@gmail.com