




Bacteremia and infective endocarditis caused by Staphylococcus aureus are common and severe diseases. Optimization of treatment is fundamental in the prognosis of these infections. The high rates of treatment failure and the increasing interest in the influence of vancomycin susceptibility in the outcome of infections caused by both methicillin-susceptible and -resistant isolates have led to research on novel therapeutic schemes. The interest in the new antimicrobials with activity against methicillin-resistant staphylococci has been extended to susceptible strains, which still carry the most important burden of infection. New combinations of antimicrobials have been investigated in experimental and clinical studies, but their role is still being debated. Also, the appropriateness of the initial empirical therapy has acquired relevance in recent years. The aim of this guideline is to update the 2009 guidelines and to provide an ensemble of recommendations in order to improve the treatment of staphylococcal bacteremia and infective endocarditis, in accordance with the latest published evidence.
La bacteriemia y la endocarditis infecciosa causadas por Staphylococcus aureus son enfermedades frecuentes y graves. El tratamiento antibiótico es clave en el éxito terapéutico. El reciente descubrimiento de la relación entre la susceptibilidad a vancomicina y el pronóstico de estas infecciones, tanto cuando en cepas resistentes como sensibles a meticilina, ha llevado a la investigación de nuevos tratamientos. El interés por los nuevos antibióticos con actividad frente a cepas resistentes a meticilina se ha extendido a las cepas sensibles, aún responsables de la mayor parte de infecciones. Estudios clínicos y experimentales han evaluado la eficacia de nuevas combinaciones de antimicrobianos, si bien su indicación no ha sido aún establecida. También la necesidad de un tratamiento inicial empírico correcto ha cobrado relevancia. El objetivo de este documento es actualizar el documento de consenso del 2009 y obtener un conjunto de recomendaciones para mejorar el tratamiento de la bacteriemia y endocarditis estafilocócicas, de acuerdo a la última evidencia científica publicada.
It has only been six years since our panel published a Clinical Guideline on the management of methicillin-resistant Staphylococcus aureus bacteremia (SAB) and infective endocarditis (IE).1 However, SAB and IE continue to be a clinical problem of paramount importance, and considerable evidence has been published during the last few years. In addition to significant advances in the research of methicillin-resistant S. aureus (MRSA) bloodstream infection, very interesting studies focusing on the prognosis and clinical management of methicillin-susceptible S. aureus bacteremia have been performed. Indeed, methicillin-susceptible strains actually carry the most important burden of this clinical challenge. New studies suggest that some aspects such as the vancomycin MIC could be relevant, also in the setting of methicillin-susceptible S. aureus. Also, when initiating the treatment for SAB, some relevant information is still lacking, and the possibility of an underlying IE has not been ruled out. Thus, there is a clinical need for reconciling important aspects in the management of SAB, such as the empirical and definitive treatment, the length of therapy, or the antimicrobial treatment integration in a wider context of management optimization. Therefore, the main objective of this Clinical Guideline is to provide an ensemble of recommendations in order to improve the treatment of bacteremia and IE caused by S. aureus, in accordance to the latest evidence published.
This Guideline will review important microbiological and genetic concepts of SAB pathogenesis and epidemics. It will also analyze the management of three specific clinical scenarios: clinical suspicion of SAB; confirmed non-complicated and complicated SAB; and infective endocarditis. The management of secondary bacteremia in specific staphylococcal infections is beyond the scope of this Guideline. Finally, the role of care bundles that may contribute to ameliorate the prognosis of SAB will be also analyzed. The whole document is available in the online version.2
Microbiological aspects of SABWhat are the available techniques to identify methicillin-susceptible S. aureus (MSSA) or MRSA in positive blood cultures?Recommendation- •
The implementation of early detection of S. aureus in positive blood cultures by matrix-assisted laser desorption ionization time-of-flight spectrometry (MALDI-TOF MS), or other rapid techniques, combined with the detection of methicillin susceptibility by polymerase chain reaction (PCR) based methods has proven to be a convenient combination for the early diagnosis of S. aureus bacteremia and methicillin susceptibility (A-II).
- •
The active notification of the microbiological results is recommended, as part of a bundle of interventions aimed to improve the management of patients with SAB (A-I).
- •
The European Committee of Antimicrobial Susceptibility Testing (EUCAST) specific methods for the detection of antimicrobial mechanisms of resistance of clinical and/or epidemiological importance are recommended (B-III).
- •
For the detection of methicillin-resistance by disc diffusion, cefoxitin is the agent of choice (B-III).
- •
Broth microdilution is the gold standard method for determining vancomycin MIC, but it can also be determined by strip methods, agar dilution or automated systems (B-III).
- •
The constant changes in the pattern of antimicrobial resistance in S. aureus must be regularly monitored. Surveillance must be performed on a monthly basis in high-risk units, and at least once per year in a whole institution (B-III).
- •
It is also recommended to monitor the evolution of susceptibility to vancomycin, daptomycin and linezolid in successive isolates from the same patient (B-III).
- •
With the available evidence, it seems reasonable prescribing early appropriate treatment to any patient suspected to have SAB, although some subpopulations may have a more significant benefit as compared to others (A-II).
- •
Bacteremia by MRSA should be suspected in the following circumstances:
- (1)
nosocomial episodes, especially if occurring in wards with high MRSA prevalence (depending on each centre's local epidemiology) (A-II);
- (2)
non-nosocomial episodes in patients previously colonized by MRSA (A-II), coming from nursing homes (A-II) or hemodialysis centers (B-II), with a central venous catheter (CVC) (B-II) or chronic cutaneous ulcers (B-II).
- (1)
- •
Including antibiotics with activity against MRSA in community-acquired episodes with none of the former risk factors seems to be not necessary (B-II).
- •
In a suspected episode of SAB, a treatment with bactericidal activity against S. aureus must be started, so effective bactericidal concentrations are available as soon as possible, especially for cases presenting with severe sepsis or shock (C-III).
- •
The empirical treatment must include, if possible, a penicillinase-stable β-lactam (A-II).
- •
When the presence of MRSA seems likely, a second antibiotic with bactericidal activity against MRSA should be added (C-III). The following possibilities would be advisable:
- o
Vancomycin in combination with a β-lactam (B-III).
- o
In cases of severe sepsis or shock (C-III), recent use (previous 30 days) of vancomycin (C-III), a higher local prevalence of S. aureus isolates with vancomycin MIC≥1.5mg/L (measured by E-test) (C-III) and/or previous renal impairment (B-III) by the use of daptomycin in combination with a β-lactam is preferred (C-III).
- o
Alternatively, patients may be treated with daptomycin alone at recommended doses of 10mg/kg (A-II)
- o
- 1
Catheter-related bacteremia (CRB)
- •
The presence of inflammatory signs at the site of insertion of any intravenous line responsible for SAB forces the prompt removal of the catheter. Catheters should be also removed if infection is suspected (presence of catheter and no other obvious focus) and catheter is easily replaceable (A-II).
- •
A conservative approach to CRB caused by S. aureus should be only attempted in exceptional circumstances (e.g. absolute impossibility of removing the catheter for technical reasons), and taking into account the clinical and baseline characteristics of the patient (B-II). In these cases, the antibiotic lock therapy must be administered in combination with an effective systemic antimicrobial treatment (B-II). Anyway, the persistence of bacteremia beyond the first 72h of a conservative management will lead to the immediate removal of the catheter (B-II).
A careful evaluation of the patient's symptoms and an exhaustive clinical examination are essential in cases of catheter-related SAB in order to rule out possible sources of the infection. The presence of eventual metastatic septic foci must be identified (B-II).
- •
Blood cultures must be taken after 72h of the onset of appropriate antimicrobial therapy in order to rule out complicated bacteremia (A-II).
- •
Systematically performing transesophageal echocardiography (TEE) to all patients with CRB by S. aureus in order to decide the length of therapy remains controversial. The absence of valvular risk (no valvular disease, neither previous nor diagnosed at the moment of SAB) along with a clinical and microbiological response to therapy within the first 72h after the catheter removal and onset of adequate antibiotics are associated with a favorable outcome (absence of complications or relapse) in more than 95% of patients that receive treatment for at least 14 days after negative blood cultures (B-II).
- •
The length of therapy needs to be adapted to the findings of the TEE or central veins ultrasonography, when indicated (A-II).
- •
The role of new imaging molecular techniques for the diagnosis of intracardiac device-associated infections has not been fully elucidated (C-II).
- •
The treatment of choice for an episode of CRB caused by MSSA is cloxacillin (B-I).
- •
Alternatively, patients may be treated with daptomycin (A-I) or a glycopeptide (B-II).
- •
The best antimicrobial treatment in episodes caused by a strain of MSSA with low susceptibility to vancomycin (MIC≥1.5mg/L measured by E-test) has not been elucidated. This panel suggests to use a combination of cloxacillin and daptomycin when blood cultures remain positive and/or clinical improvement is not evident after catheter removal (C-III).
- •
In the case of CRB caused by MRSA, vancomycin is the treatment of choice (B-II). It may be continued in stable patients with negative blood cultures after 72h of treatment, regardless of the susceptibility of vancomycin (C-III).
- •
Alternatively, patients may be treated with daptomycin (A-I).
- •
Linezolid should be only used in patients who cannot take the previous agents (B-II).
An episode of CRB caused by S. aureus may be considered as non-complicated on the basis of several characteristics of the host (such as absence of diabetes, immunosuppressant conditions and intravascular devices), by the clinical presentation, and by the clinical and microbiological evolution (clearance of bacteremia in less than 3 days of adequate treatment).
For how long must the patients be treated?Recommendations- •
Systemic antibiotics in cases of non-complicated CRB caused by S. aureus must be administered for a period not shorter than 14 days (A-II).
- •
In patients with favorable clinical and microbiological evolution, sequential oral antibiotics may be considered (A-II).
- 2
Primary SAB
- •
A careful evaluation of the patient's symptoms and an exhaustive clinical examination are essential in cases of primary SAB in order to rule out possible sources of the infection (C-I).
- •
A reliable echocardiographic test should be performed in carriers of intracardiac devices and in cases of community-acquired SAB (A-II).
- •
Recommendations for the specific definitive antimicrobial treatment for primary SAB do not differ from those of CRB by S. aureus(B-II).
- •
The duration of antibiotics should be no shorter than 14 days (B-II).
- •
In patients carrying intravascular prostheses, the length of therapy will depend on the findings of the complementary tests performed to discard a secondary involvement of these devices (C-I).
Complicated SAB is defined as the persistence of positive blood cultures after three or more days of adequate treatment (including catheter removal), and/or the development of septic thromboflebitis, IE or other metastatic distant foci.
Which clinical and microbiological evaluation must be made in patients with complicated SAB?Recommendations- •
Blood cultures must be repeated every 72h in order to monitor the microbiological response to antibiotic therapy (A-II).
- •
Make it sure that an intravenous catheter left in place is not the origin of the persistent bacteremia (A-II).
- •
When a foreign body (i.e. prosthetic joints or prosthetic valves) becomes infected, the indication of surgery for debridement and/or removing the device must be considered (A-II).
- •
It is necessary to perform an echocardiography to all patients with complicated SAB. In patients with an intracardiac device or in those with persistent bacteremia performing a TEE (A-II) is preferable.
- •
The treatment of choice for complicated bacteremia caused by MSSA is cloxacillin, either 2g every 4h, or administered in continuous infusion (A-I).
- •
Combined therapy is recommended in the following scenarios: (1) persistence of fever; lack of improvement of signs and symptoms (B-III); (2) microbiological failure detected by positive subsequent blood cultures, especially in episodes caused by an isolate with vancomycin MIC≥1.5mg/L (measured by E-test). The possible options for combined therapy are (A-III):
- o
Cloxacillin 2g/4h iv+Daptomycin 10mg/kg/d iv
- o
Cloxacillin 2g/4h iv+Fosfomycin 2g/6h iv
- o
- •
The length of therapy in complicated bacteremia is variable, ranging between 4 and 6 weeks since the first sterile blood culture, according to the clinical evolution and the source of infection. The length of combined therapy is not established, but it seems reasonable to maintain it at least until blood cultures became negative.
- •
The best treatment for complicated MRSA bacteremia has not been elucidated
- •
Treatment with vancomycin is associated with a high rate of treatment failure (A-II), especially, in the following situations:
- o
if vancomycin MIC≥1.5mg/L (measured by E-test) (A-II)
- o
if the patient has renal impairment or is at risk of renal toxicity (A-II).
- o
- •
Doses of 6mg/kg/24h of daptomycin have been associated with treatment failure and emergence of resistance. Daptomycin at doses of 10mg/kg/d is the treatment of choice for MRSA complicated bacteremia (A-III).
- •
Patients with persistent bacteremia or severe sepsis or shock in the setting of treatment with high doses of daptomycin may benefit from combined therapy. The options are
- o
Daptomycin (10mg/kg/d)+fosfomycin (2g/6h) (A-III)
- o
Daptomycin (10mg/kg/d)+cloxacillin 2g/4h (A-III)
- o
Imipenem (1g/6h) plus fosfomycin (2g/6h) (A-III).
- o
- •
The administration of high doses of fosfomycin may lead to sodium overload and hypokalemia (1g of fosfomycin-disodium carries 13.5mEq [330mg] of Na).
- •
The duration of treatment for complicated bacteremia is variable, ranging from 4 to 6 weeks, depending on the clinical evolution and the source of the infection.
- •
In patients with complicated SAB, a daily clinical monitoring is necessary for evaluating the response to the antimicrobial therapy (A-III).
- •
Consecutive determinations of C-reactive protein (CRP) (every 24–48h) during the first week of treatment may be a useful marker for an early evaluation of the treatment efficacy (B-III).
- •
It is also recommended to take new blood cultures every 72h until they are negative (C-III).
- •
In cases of persistent bacteremia, the antimicrobial treatment should be re-evaluated (A-III).
- •
In complicated SAB, antimicrobial treatment should be administered entirely by the intravenous route.
- •
An oral sequential treatment may be considered for patients accomplishing the following requirements (C-III):
- o
the patient has presented no fever for at least 24h
- o
blood cultures are negative
- o
the origin of infection has been drained
- o
the parameters of systemic inflammation (i.e. CRP) have significantly decreased.
- o
- •
In exceptional situations where an intravenous access is not possible, there is some experience supporting the use of oral fluoroquinolones plus rifampin (BII).
- 1
Empirical antimicrobial treatment in IE caused by S. aureus
- •
The empirical antimicrobial treatment of complicated bacteremia or IE should include S. aureus whenever there are reasonable doubts on its potential role as etiology, given its high and increasing incidence and severity.
- •
Therefore, active antibiotics against S. aureus should be included in the empirical treatment in the following cases:
- o
suspicion of community-acquired IE [either in intravenous drug users (IVDUs) or not];
- o
suspicion of acute IE or presenting with severe sepis (B-II);
- o
and early PVE, associated to pacemakers or defibrillators (B-II), or in nosocomial cases or in health care associated cases (B-II).
- o
- •
In the setting of SAB, it is recommended considering the diagnosis of IE until it has been ruled out by complementary tests (namely TEE) in the following scenarios:
- o
community-acquired episodes (B-II);
- o
IVDUs (B-II);
- o
presence of skin lesions suggesting hematogenous seeding (B-II);
- o
and nosocomial bacteremia in the presence of prosthetic valves or intracardiac devices (B-II).
- o
- •
The empirical antimicrobial treatment for IE should include activity against MRSA in any of the following instances:
- o
nosocomial cases (B-II),
- o
previous nasal or skin colonization by MRSA (B-II),
- o
patients from nursing-homes (B-II) or in hemodialysis (B-II),
- o
surgical procedure within the 6 months preceding the bacteremia (B-II),
- o
or the presence of certain baseline conditions (diabetes, cancer, immunosuppressant therapy) (B-II).
- o
- •
When community-acquired IE caused by S. aureus is suspected, the treatment of choice is cloxacillin (B-II).
- •
In a critically ill patient, or in patients with severe sepsis or septic shock, many experts recommend adding daptomycin to the treatment with cloxacillin (C-III).
- •
Patients allergic to β-lactams may be treated with cefazolin (if no previous anafilaxia has been reported) (B-II), or with the combination of daptomycin plus fosfomycin (C-III).
- •
The inclusion of gentamicin in the empiricial treatment of community-acquired native valve IE caused by S. aureus during the first 3–5 days is not recommended (D-I).
- •
In the setting of health care related IE caused by S. aureus, monotherapy with vancomycin is not recommended (D-II).
- •
In this context, daptomycin in combination with cloxacillin is recommended (B-II). For patients allergic to β-lactams, cloxacillin may be substituted by fosfomycin (C-III).
- •
Faced with a suspected IE but no available blood cultures, the use of daptomycin in combination with a β-lactam with activity against nosocomial Gram-negative microorganisms is recommended (C-III).
- 2
Definitive antimicrobial treatment for IE caused by S. aureus
- •
For native valve left side IE caused by MSSA, cloxacillin for 4 to 6 weeks is recommended (B-II), and two weeks for non-complicated right valve IE among IVDUs (A-I).
- •
Daptomycin may be added to cloxacillin in the case of persistent bacteremia detected by the positivity of subsequent blood cultures, especially in episodes caused by an isolate with vancomycin MIC≥1.5mg/L (measured by E-test) (C-III).
- •
Systematic combination with gentamicin is not recommended (D-II). In patients allergic to β-lactams, the combination of daptomycin plus fosfomycin is recommended (C-III).
- •
Cloxacillin is recommended in prosthetic IE caused by MSSA (C-II), in association with rifampin after the first 5 days of treatment (C-III), and gentamycin in a once-daily dose during the first two weeks of therapy (C-II).
- •
In the case of allergy to β-lactams, the same combination of antibiotics may be used, with the substitution of cloxacillin by daptomycin (C-III).
- •
Daptomycin plus cloxacillin is recommended in native valve IE caused by MRSA when vancomycin MIC is ≥1.5mg/L (measured by E-test) (B-II).
- •
The same treatment may be administered when vancomycin MIC is <1.5mg/L (measured by E-test), or vancomycin is at doses providing trough levels of 15–20mg/L (B-II).
- •
In patients allergic to β-lactams, the combination of daptomycin plus fosfomycin is recommended (B-II), or the use of vancomycin at doses providing trough levels of 15–20mg/L (B-II).
- •
Neither the addition of rifampin (D-III) or gentamicin (D-III) to the treatment is recommended.
- •
In prosthetic valve IE caused by MRSA with vancomycin MIC≥1.5mg/L (using E-test), the use of daptomycin, in combination with rifampin after 5 days of treatment, and gentamicin in one single daily dose during the first two weeks of therapy is recommended (C-III). Daptomycin plus fosfomycin could be used alternatively (C-III)
- •
In the case of MIC<1.5mg/L (using E-test), the same combination may be used (C-III), or vancomycin combined with rifampin after 5 days of treatment, plus gentamicin in a one single daily dose during the first two weeks of treatment (B-II).
In patients with IE caused by MRSA presenting clinical failure with previous recommended schedules, the administration of daptomycin plus fosfomycin may be used (B-II). Fosfomycin plus imipenem could also be used (C-II)
- •
If this cannot be done, either because of allergy or a high risk of sodium overload, ceftaroline, either alone (B-II) or combined with daptomycin (C-II), or linezolid, alone (C-II) or associated with daptomycin (C-III), may be valid alternatives.
- 3
Role for surgery in IE caused by S. aureus.
- •
Patients suffering from IE caused by S. aureus share the same indications for surgery as other cases due to other microorganisms, with the exception of prolonged MRSA bacteremia (A-II).
- •
Therefore, international guidelines may be followed (A-II); but if blood cultures after 72h from the onset of appropriate treatment still yield MRSA, complementary tests should be performed in order to rule out metastatic foci, and the cardiac surgeons should be contacted (B-II).
- •
In patients with native or prosthetic valve IE caused by S. aureus undergoing valve replacement and cultures being negative, it is recommended to administer two more weeks of therapy or simply finish the initially scheduled treatment (B-II).
- •
In patients with positive valve cultures after surgery, it is recommended to restart the treatment of IE (i.e., ≥4 weeks for native valve IE, and ≥6 weeks for prosthetic IE) (C-III).
- •
At least quality-of-care indicators should be considered in all patients with SAB (BII).
- •
Active, unsolicited infectious diseases specialist (IDS) consultation for management and follow-up should be provided to physicians in charge of all patients with SAB (BII).
- •
The specialized recommendations to physicians in charge of patients with SAB should be provided in a structured manner so all quality-of-care indicators of the management are considered (BII).
Francesc Gudiol has received academic grants from Novartis, Astellas and AstraZeneca. José María Aguado has been a consultant to and is on the speakers’ bureau for Astellas Pharma, Astra Zeneca, Pfizer, Gilead Sciences, Novartis, Merck Sharp and Dohme, and Roche. Benito Almirante has carried out consultancy work or received monetary payments for giving talks from Astellas, Astra Zeneca, Gilead Sciences, Janssen-Cilag, Merck Sharp and Dhome, Novartis and Pfizer. Jesús Rodríguez-Baño has been a consultant and speaker for Pfizer, Novartis, Merck, AstraZeneca and Astellas, and has received research grants from Novartis and Gilead. Jose M. Miro has received consulting honoraria from Abbvie, Bristol-Myers Squibb, Gilead Sciences, Merck, Novartis and Sanofi, research and academic grants from Cubist, Gilead, ViiV, Novartis, Merck, Fondo de Investigaciones Sanitarias (FIS) del Instituto de Salud Carlos III (Madrid), Fundación para la Investigación y Prevención del Sida en España (FIPSE, Madrid), Ministerio de Sanidad, Servicios Sociales e Igualdad (MSSSI, Madrid), National Institutes of Health (NIH, Bethesda, MA, USA) and NEAT and honoraria for lectures from Abbvie, Bristol-Myers Squibb, Gilead Sciences, Merck, Novartis and ViiV Healthcare. Alex Soriano has been a speaker for Pfizer and Novartis.
We are indebted to Dr. Rafael San Juan for his invaluable help in the reference management of this article. REIPI is supported by the Plan Nacional de I+D+i 2008–2011 and the Instituto de Salud Carlos III, Subdirección General de Redes y Centros de Investigación Cooperativa, Ministerio de Economía y Competitividad, and Spanish Network for Research in Infectious Diseases (REIPI RD12/0015) – co-financed by European Development Regional Fund “A way to achieve Europe” ERDF.
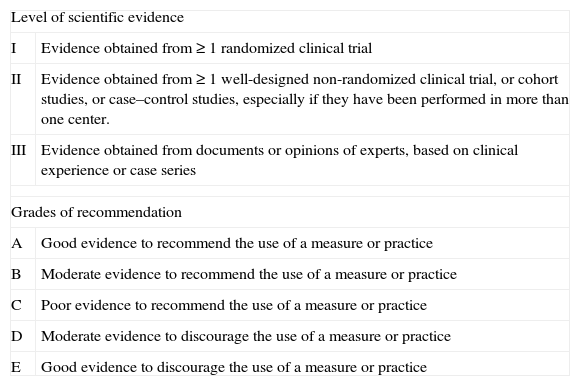
| Level of scientific evidence | |
| I | Evidence obtained from ≥ 1 randomized clinical trial |
| II | Evidence obtained from ≥ 1 well-designed non-randomized clinical trial, or cohort studies, or case–control studies, especially if they have been performed in more than one center. |
| III | Evidence obtained from documents or opinions of experts, based on clinical experience or case series |
| Grades of recommendation | |
| A | Good evidence to recommend the use of a measure or practice |
| B | Moderate evidence to recommend the use of a measure or practice |
| C | Poor evidence to recommend the use of a measure or practice |
| D | Moderate evidence to discourage the use of a measure or practice |
| E | Good evidence to discourage the use of a measure or practice |

