




Chlamydia trachomatis infection is the most common bacterial sexually transmitted disease. Re-infections are a major problem in its control as they increase the probability of developing sequellae.
ObjectivesTo estimate the prevalence of C. trachomatis and re-infection rate after 6 months of treatment by determining the possible causes.
MethodsCross-sectional study in which a urine sample was analysed by PCR in a convenience sample of 506 sexually active youths aged 16–25years. An epidemiological survey and re-test was performed at 3months.
ResultsThe prevalence of C. trachomatis was 8.5%. The age (OR=2.34; 95%CI: 1.21–4.55) and concurrency (OR=3.64; 95% CI: 3.58–26.39) were determining factors for acquiring C. trachomatis. The re-infection rate was 10.34%.
DiscussionThe high prevalence of C. trachomatis, as well as the rate of reinfection, suggest the need to assess the effectiveness of the opportunistic screening program and ensure high levels of reporting of sexual partners. Ensuring these approaches facilitate the control of C. trachomatis among young people.
La infección genital por Chlamydia trachomatis es la infección de transmisión sexual bacteriana más común. Un problema importante para su control son las reinfecciones, ya que incrementan la probabilidad de desarrollar secuelas.
ObjetivosEstimar la prevalencia de C. trachomatis y la tasa de reinfección a los 6meses de tratamiento determinando las posibles causas.
MétodosEstudio transversal con muestra de orina analizada por PCR en una muestra de conveniencia de 506 jóvenes de 16–25años sexualmente activos con encuesta epidemiológica y re-test a los 3meses.
ResultadosLa prevalencia de C. trachomatis fue del 8,5%. La edad (OR=2,34; IC95% 1,21–4,55) y la concurrencia (OR=3,64; IC95% 3,58-26,39) fueron factores determinantes para su adquisición. La tasa de reinfección fue del 10,34%.
DiscusiónLa elevada prevalencia de C. trachomatis, así como la tasa de reinfección, plantean la necesidad de valorar la eficacia de un programa de cribado oportunista y garantizar altos niveles de notificación de parejas sexuales. Garantizar estos enfoques facilitaría el control de C. trachomatis entre los jóvenes.
The Chlamydia trachomatis genital infection is the most common bacterial sexually transmitted infection (STI), which most frequently affects the young population.1 If it is not detected or treated it can lead to serious consequences, such as pelvic inflammatory disease (PID), ectopic pregnancy and infertility.2C. trachomatis infections do not confer long-term immunity, so people who have been infected and treated can be reinfected. A high rate of reinfection has been observed in the months following treatment. Some authors have identified up to 20% of women are reinfected within a year of post-treatment follow-up.3 Studies have shown that the cumulative risk of long-term reproductive consequences increases with repeated C. trachomatis infections. In a study by Hillis et al.,4 women who tested positive for C. trachomatis on 2 occasions had a 4-fold higher risk of developing PID, and the risk increased up to 6-fold in women who tested positive on 3 or more occasions. Therefore, post-treatment control is important. That is why some agencies, such as the Centers for Disease Control and Prevention (CDC), and the European guide for the management of C. trachomatis infection recommend performing a re-test at 3 months, as well as the contact study.5,6
Reinfections can occur due to non-compliance with treatment regimens, and especially due to unprotected sexual contact, either with untreated partners in ongoing sexual relationships or with a new infected partner.7,8 Distinguishing between these causes is important for focusing recommendations and disease control activities.
In Catalonia, cross-sectional studies have been carried out among the young population since 2007 in order to determine and monitor the prevalence of C. trachomatis infections and to describe the characteristics and possible determinants of the affected population. However, neither the reinfection rate nor the reasons for it are known.
The present study aims to estimate the prevalence of C. trachomatis infection and the rate of reinfection at 3 months of treatment by determining the possible causes among the population of young people under the age of 25.
MethodologyCross-sectional study to detect C. trachomatis infection in a representative convenience sample of 506 sexually-active young people between 16 and 25 years of age, who received care between May and October 2012 in primary care centres with a specific program for sexual and reproductive healthcare for young people in Catalonia (distributed in the healthcare regions of Lleida, Barcelona, central Catalonia [Vallès Oriental, Occidental and Osona regions] and Girona).
To collect sociodemographic, clinical and sexual behaviour data (sex, age, origin, number and type of partners, sexual practices, drug use, etc.), an anonymous, semi-structured and standardised questionnaire was collected and urine samples analysed using a polymerase chain reaction, an Abbott Molecular real-time PCR, according to manufacturer's specifications (Abbott Real Time Chlamydia trachomatis/Neisseria gonorrhoeae Assay, Abbott Molecular, IL, USA) was used. Those who did not meet the established age, those who had not been sexually active in the last year, and menstruating women were excluded from the study.
In the event of a positive result, the clinical and preventive management was conducted according to the European clinical practice guidelines:6 (1) treatment (azithromycin 1g, single dose); (2) sexual counselling; (3) contact study: evaluation and treatment of the contacts of the last 3 months, and (4) re-test for C. trachomatis at 3 months of treatment.
Quantitative variables are stated with their frequency and standard deviation (SD). Qualitative variables are stated with their frequency and proportion. The proportions were compared using the Pearson chi-squared test. The multivariate analysis of logistical regression assessed the sociodemographic and sexual behaviour variables associated with the response variable (C. trachomatis infection). Variables with a p<0.10 in the univariate model were included in the multivariate model and the adjusted odds ratios (OR) and their respective confidence intervals (CI 95%) were calculated. The data were analysed with the SPSS Statistics software package (version 18.0, SPSS Ibérica, SLU).
The study was approved by the Independent Ethics Committee of Hospital Universitari Germans Trias i Pujol of Badalona.
ResultsA total of 506 young people were recruited with a mean age of 21 years (SD=2.7), the majority of whom were women (90.9%). 24.5% were foreigners, of whom 92.7% were women and 7.3% were men, from Latin America (83%), Eastern Europe (7.3%) and northern Africa (3.3%). Medium-high educational level (90% with secondary and higher education). The mean age for initiating sexual relations was 17 (SD=2.3; range 12–25), with no differences being observed by sex or origin. Most (96%) stated that they had heterosexual relationships. The mean number of partners in the last year was 2 (SD=1). Men had a higher average number of partners than women, although this difference was not significant (3.5 vs 2.7; p=0.95). Other behaviour characteristics are shown in Table 1.
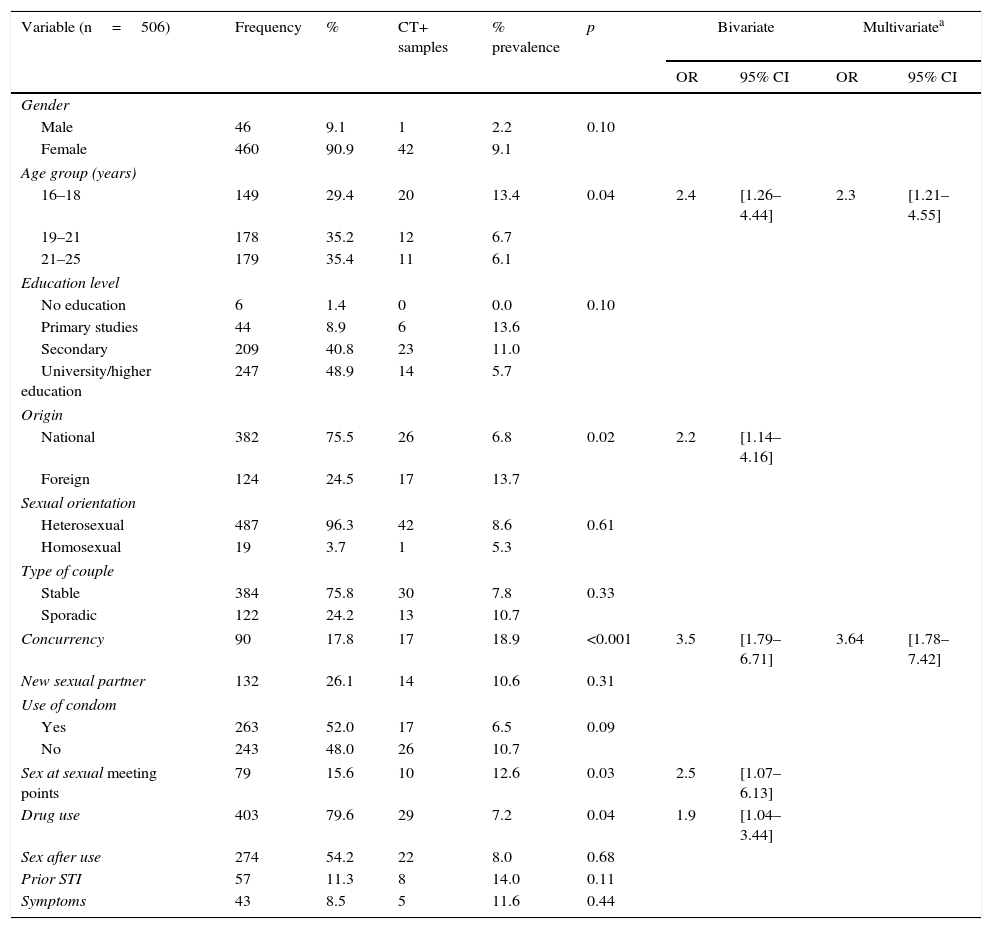
Sociodemographic and behavioural characteristics and associated factors for C. trachomatis (CT) infection among young people from 16 to 25 years.
| Variable (n=506) | Frequency | % | CT+ samples | % prevalence | p | Bivariate | Multivariatea | ||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | ||||||
| Gender | |||||||||
| Male | 46 | 9.1 | 1 | 2.2 | 0.10 | ||||
| Female | 460 | 90.9 | 42 | 9.1 | |||||
| Age group (years) | |||||||||
| 16–18 | 149 | 29.4 | 20 | 13.4 | 0.04 | 2.4 | [1.26–4.44] | 2.3 | [1.21–4.55] |
| 19–21 | 178 | 35.2 | 12 | 6.7 | |||||
| 21–25 | 179 | 35.4 | 11 | 6.1 | |||||
| Education level | |||||||||
| No education | 6 | 1.4 | 0 | 0.0 | 0.10 | ||||
| Primary studies | 44 | 8.9 | 6 | 13.6 | |||||
| Secondary | 209 | 40.8 | 23 | 11.0 | |||||
| University/higher education | 247 | 48.9 | 14 | 5.7 | |||||
| Origin | |||||||||
| National | 382 | 75.5 | 26 | 6.8 | 0.02 | 2.2 | [1.14–4.16] | ||
| Foreign | 124 | 24.5 | 17 | 13.7 | |||||
| Sexual orientation | |||||||||
| Heterosexual | 487 | 96.3 | 42 | 8.6 | 0.61 | ||||
| Homosexual | 19 | 3.7 | 1 | 5.3 | |||||
| Type of couple | |||||||||
| Stable | 384 | 75.8 | 30 | 7.8 | 0.33 | ||||
| Sporadic | 122 | 24.2 | 13 | 10.7 | |||||
| Concurrency | 90 | 17.8 | 17 | 18.9 | <0.001 | 3.5 | [1.79–6.71] | 3.64 | [1.78–7.42] |
| New sexual partner | 132 | 26.1 | 14 | 10.6 | 0.31 | ||||
| Use of condom | |||||||||
| Yes | 263 | 52.0 | 17 | 6.5 | 0.09 | ||||
| No | 243 | 48.0 | 26 | 10.7 | |||||
| Sex at sexual meeting points | 79 | 15.6 | 10 | 12.6 | 0.03 | 2.5 | [1.07–6.13] | ||
| Drug use | 403 | 79.6 | 29 | 7.2 | 0.04 | 1.9 | [1.04–3.44] | ||
| Sex after use | 274 | 54.2 | 22 | 8.0 | 0.68 | ||||
| Prior STI | 57 | 11.3 | 8 | 14.0 | 0.11 | ||||
| Symptoms | 43 | 8.5 | 5 | 11.6 | 0.44 | ||||
CT: C. trachomatis infection.
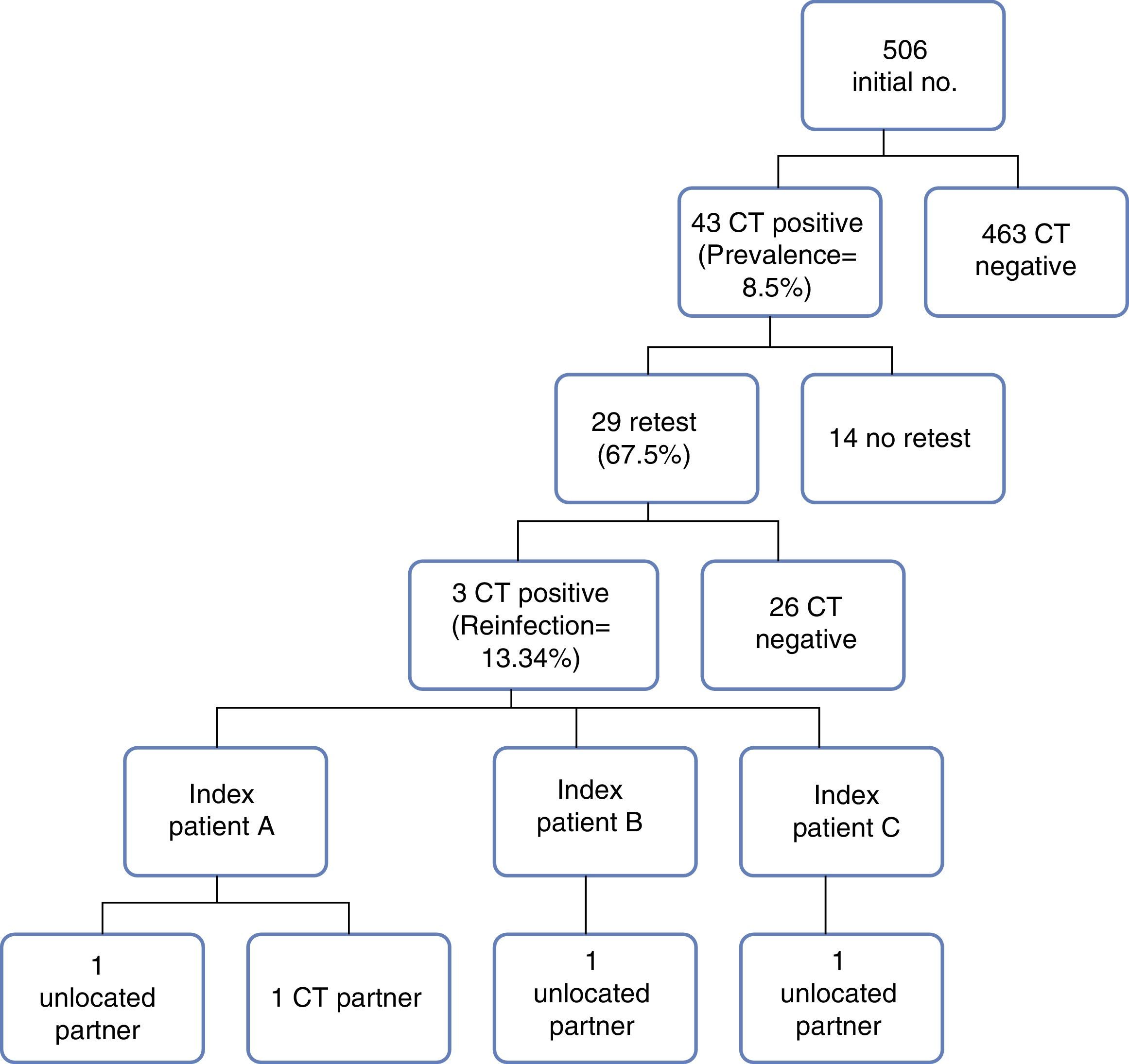
The prevalence of C. trachomatis was 8.5% (43/506), and was higher in women (p=0.10). There were significant differences in origin (foreign vs national, p=0.02) and in age (higher prevalence in the 16–18 year range, p=0.04) (Table 1). Age (OR=2.34; CI 95% 1.21–4.55) and the concurrency of partners (maintaining relationships simultaneously with more than one person) (OR=3.64; CI 95% 1.78–7.42) were determining factors for the acquisition of C. trachomatis in the multivariate analysis (Table 1). The 43 positive cases received treatment, with only 28% (12/43) being able to begin the contact study, obtaining: 5 positive and treated contacts, 4 contacts with epidemiological treatment (immediate treatment of the sexual partners of the last 3 months without performing any diagnostic study) and 3 negative contacts.
A new test was performed at 3 months of treatment on 2/3 of patients infected with C. trachomatis. The reinfection rate was 10.34% (3/29). These were 3 foreign women between 16 and 18 years of age and with a new partner in the last 3 months. The 3 cases had received initial treatment (azithromycin 1g, single dose) and the contact study had begun, the results of which were as follows: (a) one of the cases mentioned 2 sexual partners: one of whom was C. trachomatis negative and the other could not be located; (b) the second case mentioned a partner who could not be located, and (c) pregnant and treated but not the partner (Fig. 1).
Discussion
The prevalence of C. trachomatis obtained, despite not being a population study, resembles that of countries like England or Denmark where, with population data, it is around 8%.9 The prevalence values for C. trachomatis in Catalonia have increased in recent years among the young population.10 This increase is associated in part with the increase in the number of diagnoses, in the reporting of cases to surveillance systems and in sexual risk behaviours. Age is the most common socio-demographic risk factor for C. trachomatis. The imbalance between physiological maturity and the degree of psychological development makes young people more vulnerable to situations of risk in interpersonal and sexual relations.11 Other determining factors for C. trachomatis infection include, in our case, being of foreign origin, associated in part with the situation of social and economic precarity that is related with behaviours of low personal self-care, and the frequency of partners. The latter is indicated as a predictor for C. trachomatis infection by other authors. A certain number of people connected in the same period of time who tend to use a condom less than in simple monogamous relationships, increasing the probability of infection.12–14
The rate of reinfection found is comparable to that reported by other authors, although in the case of population data, it ranges from 7% to 21%.3,15,16 Likewise, the determinants of reinfection found—not screening or treatment of the partner—have been evidenced in other publications,7,8 which raises the need to establish effective control mechanisms.
In Catalonia, although the mandatory disease reporting regulation establishes that the contact study is the responsibility of doctors, and in spite of the tools provided to them to facilitate their practice, this remains a point to be strengthened within the healthcare system. The main reasons that make it difficult to carry out and/or follow-up on the contact study are, on the one hand, the scarce use of health services by men when it comes to their sexual health, and on the other hand, the difficulty in contacting casual couples. These difficulties mean that the practice of conducting the contact study has been reduced to recommending that the patient informs their partners of their condition so that they go to the doctor. In our case, the contact study was completed in only 28% of the cases. Therefore, the results show the need to use strategies to speed up identification and treatment of sexual partners, especially when we consider that C. trachomatis infection is asymptomatic in about 70% of cases, and the contact study is a tool to detect these cases. In our context, given that young people, especially men, tend not to use health services as much, the single dose treatment strategy for azithromycin as an epidemiological treatment “expedited partner therapy” (EPT) should be recommended11 in contrast with standard contact treatment guidelines. Studies designed to compare EPT with standard uptake approaches suggest that EPT is a useful cost-effective strategy to ensure treatment of the partner(s), reduce the frequency of sexual relations with untreated partners17,18 and reduce the frequency of C. trachomatis infection.19 In fact, there are studies that show that where the partner is not treated, the expected rate of reinfection is 19.4%. On the other hand, if these partners received EPT, the expected likelihood of reinfection would be reduced to 4.2%.19,20
As mentioned earlier, the scarce use of health services by men made them difficult to track down, and as a result, the contact study was only performed in 12 out of 43 possible cases, which is one of the limitations of the study. In turn, the reinfection rate identified can only be explained for 2/3 of the possible cases to be retested. Also added to the limitations is the possible social desirability bias for questions related to drug use or sexual behaviour, leading to an underestimation of risk behaviours.
In spite of the limitations, due to the results obtained we emphasise that both the high prevalence of C. trachomatis and the reinfection rate suggest the need to establish an opportunistic screening program in our country to reduce the burden of morbidity and associated reproductive effects, as is already done in several European countries.9 Other prevention strategies must also be performed, including behavioural interventions, the screening of infected persons, and, since the contact study is effective in both preventing the transmission of the infection to sexual partners and reinfection of the index case, it is important to ensure high levels of partner notification. This entails a greater involvement by healthcare professionals in the diagnosis and follow-up of STIs and the implementation of strategies to reduce the time between diagnosis and treatment of the index case and of their partners (for example, the use of EPT), thereby ensuring a substantial reduction in reinfection rates.
FundingWe appreciate the funding from the Department of Health of the Generalitat de Catalunya and the partial funding from CIBER Epidemiology and Public Health (CIBERESP).
Conflicts of interestThe authors declare that they have no conflicts of interest.
We appreciate the collaboration of the members of the work group created for this project.
ASSIR CAP II Prat de la Riba, Lleida (M.J. Garrofé), ASSIR Hospital de Palamós, Palamós (E. César, E. Folch), ASSIR BSA Mare de Deu de Lorda, Badalona (A. Avecilla, M. de Sebastián, M. Teixido), ASSIR Mataró-Maresme, Mataró (A. de Castro, I. Gonzalez, C. Coll), ASSIR CAP II Sant Fèlix, Sabadell (R. Espelt, M. Abella, G. Falguera), ASSIR CAP II Cerdanyola-Ripollet, Ripollet (A. Acera, M. Robert, A. Cárceles, N.A. Sánchez, M. Robert, M. Llucià, P. Soteras, A, Cuenca, S. Mesa), ASSIR CAP Osona, Vic (J. Tarres, J. Grau), ASSIR Bages-Solsonès, Manresa (N. Crespo, P. Piqué), ASSIR Terrassa, Terrassa (M.I. Cayuela), ASSIR Mollet, Mollet del Vallès (E. López, M. Manzanares, E. Adarve, A, Torrent), ASSIR Granollers, Granollers (D. Guix), ASSIR Esquerre, Barcelona (C. Seguí, J. Xandri, R. Almirall, F. Valenzuela, A. Payaró, L. Zamora, C. Piorno, M. Roure, G. Labay, R. Astudillo, X. Diez, E. Picola, R. Escriche, E. Vela, C. Fernandez), Centre de Salut per a Joves de l’Hospitalet, Hospitalet del Llobregat (E. Arranz, E. Castillo), Centre Jove d’Anticoncepció i Sexualitat, CJAS, Barcelona (I. Campo, R. Ros), Centre Jove de Salut, Girona (M. Hernandez, C. Fornells).
Please cite this article as: López-Corbeto E, González V, Casabona J, Grupo de estudio CT/NG-ASSIR. Prevalencia y tasa de reinfección de la infección genital por C. trachomatis en menores de 25 años en Cataluña. Enferm Infecc Microbiol Clin. 2017;35:359–363.
