




Arterial infections due to Listeria monocytogenes are rare. We present two cases treated at our site.
Case 1: 80-year-old male patient, under follow-up by our department following the implantation of a right aorto-uni-iliac endograft (Endurant®, Medtronic), left hypogastric artery embolisation and a femorofemoral bypass due to the rupture of an infrarenal abdominal aortic aneurysm.
Three years later, the patient was seen with lumbar and abdominal pain that had begun two months prior, with no fever. Laboratory tests showed raised C-reactive protein (CRP) levels of 105mg/dl. Computed tomography angiography (CTA) revealed an increase in periaortic soft tissues and fraying of locoregional fat. In light of suspected aortitis, blood cultures were obtained and broad-spectrum antibiotics were initiated via the parenteral route, with piperacillin/tazobactam. A whole body scan was performed with gallium-67 labelled leukocytes; no pathological deposit was observed at the level of the aortic endograft. After 14 days of empirical treatment and sterile blood culture results, the patient was discharged with scheduled follow-up visits and no antibiotics. After one month, his control CTA revealed no significant changes in relation to the one before.
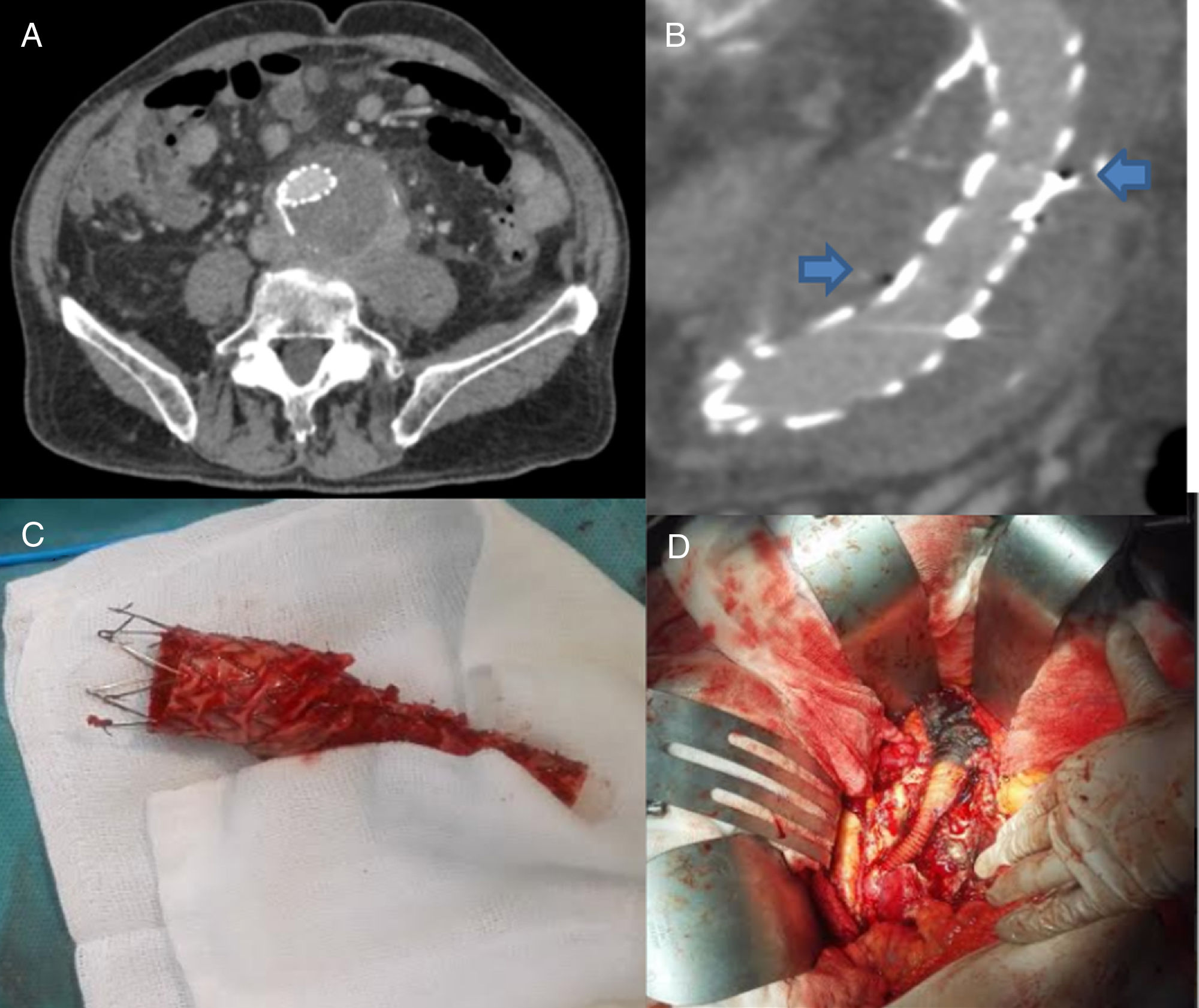
After two months, he was readmitted with diarrhoeal stools, pain in the hypogastric region and fever. Laboratory tests showed that CRP levels were still high, with no leukocytosis. Another CTA also revealed increased periaortic inflammation (Fig. 1A) and gas bubbles inside the aneurysm sac (Fig. 1B). Once the blood cultures were obtained, empirical antibiotic therapy was initiated (intravenous ceftriaxone and vancomycin), followed by emergency surgery involving the removal of the aortic endograft and the conduct of a right aorto-uni-iliac bypass with a silver-impregnated graft (Maquet Intergard Silver Knitted, Maquet Spain, SLU) (Fig. 1C and D). L. monocytogenes was isolated on the aortic endograft culture. Four weeks of ampicillin and gentamicin was followed with oral co-trimoxazole treatment. Given the risk of an infectious relapse, we decided to continue lifelong suppressive antibiotics with oral co-trimoxazole.
 Coronal slice of the CTA, showing increased volume of the periaortic tissues. (B) Sagittal slice of the CTA, revealing gas bubbles inside the aneurysm sac surrounding the aortic endograft. (C) Explanted aortic endograft. (D) Intraoperative image of the right aorto-uni-iliac bypass with the silver-impregnated graft.")
(A) Coronal slice of the CTA, showing increased volume of the periaortic tissues. (B) Sagittal slice of the CTA, revealing gas bubbles inside the aneurysm sac surrounding the aortic endograft. (C) Explanted aortic endograft. (D) Intraoperative image of the right aorto-uni-iliac bypass with the silver-impregnated graft.
After 16 months of follow-up, the patient remains asymptomatic.
Case 2: 83-year-old male patient presenting anorexia and weight loss over the course of seven months. Seen for syncope, the patient presented with associated pain in the right hypogastric region and a low-grade fever. His laboratory tests showed raised CRP (43.5mg/dl) and 15,100 leukocytes/mm3. Emergency CTA revealed the 73mm rupture of a right hypogastric artery aneurysm. After collecting blood cultures, the patient underwent surgery for the implantation of a bifurcated aortic endograft (Endurant®, Medtronic) with embolisation of the hypogastric aneurysm sac using coils (William Cook Europe, Denmark), with endograft extension to the right external iliac artery. Blood cultures were positive for L. monocytogenes, so antibiotics were initiated with intravenous ampicillin and gentamicin.
After completing six weeks of intravenous antibiotics with ampicillin (in combination with gentamicin for the first two weeks), the patient's blood cultures came back negative and the control CTA revealed no post-surgical complications. The patient was discharged on oral suppressive therapy with co-trimoxazole. After nine months of follow-up, the patient is asymptomatic.
Arterial infections due to L. monocytogenes are rare, with around 40 cases described in the literature worldwide.1–3 Regarding prosthetic vascular graft infections due to Listeria, over 10 cases have been published.4,5
L. monocytogenes is an intracellular Gram-positive bacillus, which usually causes symptoms of gastroenteritis in immunocompetent patients following the consumption of contaminated foods. Its incidence increases at both ends of the age spectrum (neonates and the elderly), in pregnant women, patients with impaired cellular immunity, corticosteroid treatment and chronic diseases such as cirrhosis, diabetes or kidney disease.
The most widely accepted surgical treatment in arterial or prosthetic vascular graft infections is open surgery, with the resection of infected tissues and graft material, and vascular reconstruction of the affected segment (prosthesis or homograft) or, where this is not deemed viable, ligature and extra-anatomic bypass.6,7
In selected cases, patients with endarteritis and a high level of comorbidity and haemodynamic instability may require the implantation of an aortic endograft, followed by long-term antibiotics.8,9 Likewise, in prosthetic infections with a difficult surgical approach, cases treated with long-term antimicrobial treatment alone have been described, with favourable short- and medium-term outcomes.5
Prolonged antimicrobial treatment is essential in the management of arterial infections due to Listeria (4–6 weeks). The recommended treatment is a combination of ampicillin and gentamicin, due to its synergic activity. Some studies have shown good results with a combination of ampicillin and co-trimoxazole. Oral co-trimoxazole is an option for ambulatory treatment.10
Please cite this article as: Romero Lozano MA, Martín-Davila P, Reyes Valdivia AA, Bernal Bernal C. Infección arterial causada por Listeria monocytogenes: a propósito de dos casos. Eficacia del abordaje combinado precoz y tratamiento supresivo oral. Enferm Infecc Microbiol Clin. 2019;37:60–61.
