




A 76-year-old patient presented at our hospital with intermittent fever of up to 40°C lasting three weeks, coinciding with stem cell inoculation in both hips. The patient had required aortic valve replacement six years earlier and, due to liver cirrhosis with hepatocarcinoma in segment 5, had also required partial hepatectomy and cholecystectomy five months earlier. Twenty days before, the patient had a dental filling for which he did not receive antibiotic prophylaxis. On examination, the patient had a fever of 39.1°C with a pansystolic murmur, and a blood test showed 12,900 leukocytes, 90% of which were neutrophils. Suspecting endocarditis, a blood culture was obtained and the patient was admitted for study and antibiotic treatment with vancomycin and cefepime (1 g/12h and 2g/24h intravenously [IV], respectively).
A transthoracic echocardiogram was performed, in which thickened aortic leaflets were observed, and also a transoesophageal echocardiogram, in which no clear images of endocarditis were observed. The blood culture was positive after 20h of incubation, showing Gram-positive cocci in chains in the Gram stain. The blood culture was inoculated on CNA agars (Becton Dickinson, New Jersey, USA), TSA agars with 5% sheep blood (BD™) and chocolate agar. At 24h, growth was observed, with its identification and antibiotic sensitivity provided by means of the SMIC-ID-11 (BD™) panel in the BD Phoenix™ AP system. The strain was identified as Streptococcus cristatus (S. cristatus), which was sensitive to penicillin (MIC ≤0.03mg/l), vancomycin (MIC = 1mg/l), teicoplanin (MIC ≤1mg/l) and clindamycin (MIC ≤0.03mg/l). In a subsequent blood culture, S. cristatus was identified again, changing the antibiotic treatment to ceftriaxone (2g/24h) while waiting to perform CT + PET-CT. After administration of IV contrast and 18-FDG, lesions compatible with small infarcts in the lower pole of the spleen and left kidney were found, as well as increased metabolic activity in the periprosthetic aortic valve, which did not prevent us from ruling out endocarditis (Fig. 1).
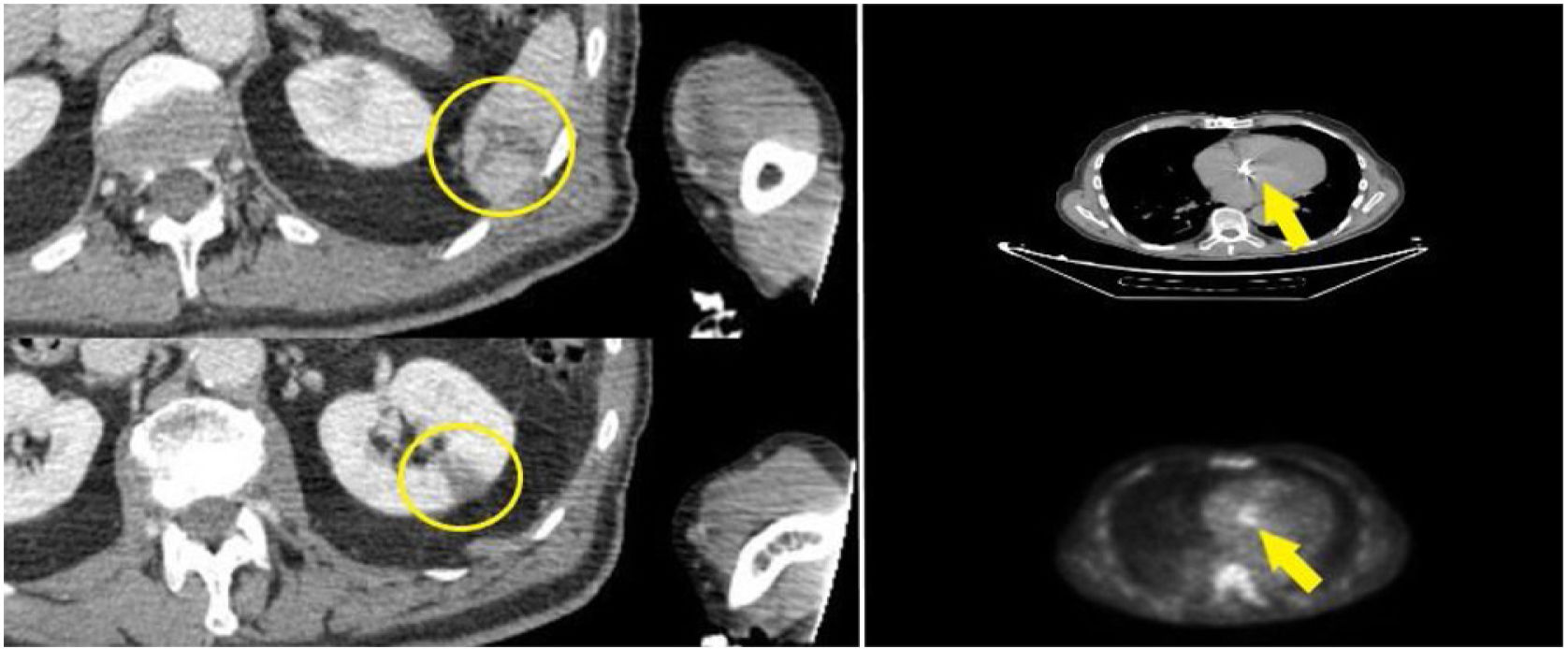
. Focal increase in metabolic activity (yellow line) on the prosthetic aortic valve annulus")
Joint CT and PET-CT study performed following endocarditis protocol after inconclusive result by transoesophageal echocardiogram by administration of intravenous contrast and 18-FDG, with imaging from the cervical region up to and including the pelvis. Hypodense lesions of triangular morphology and new appearance in the lower pole of the spleen and interpolar region of the left kidney, compatible with small infarcts (yellow circles). Focal increase in metabolic activity (yellow line) on the prosthetic aortic valve annulus's anterior region makes it impossible to rule out endocarditis without significant morphological findings.
The condition was considered as probable endocarditis (one major criterion and three minor criteria) and the patient completed six weeks of IV treatment. The patient was followed up through outpatient visits, confirming clinical improvement and normality in subsequent echocardiograms. To confirm the identification, the strain was reseeded to sequence the 16S ribosomal RNA gene. A 637bp sequence was obtained that was entered into BLASTR, and was identified as S. cristatus with an identification percentage of 99.37% (see sequencing protocol and sequence in Appendix B: Supplementary material attached).
S. cristatus was isolated for the first time from the human oral cavity, belonging to the mitisgroup.1 A 2014 study showed that S. cristatus, Streptococcus oligofermentans and Streptococcus sinensis are closely related, and a new phylogenetic clade, the “sinensis group”, was proposed to include these three microorganisms.2 The relationship between infections such as endocarditis and dental interventions has been proven, and prophylaxis is recommended in patients with risk factors, such as valve carriers. In addition, poor dental hygiene also seems to be associated with a higher risk of infections by S. cristatus.3 In the case presented here, and in another of those previously reported, the patients had minor dental interventions or a history of poor dental hygiene prior to the infection.4
Only nine clinical cases of infections caused by this microorganism have been described: six cases of infective endocarditis, one of septic arthritis and two of bacteraemia.4-9 At our institution, we have identified another case of endocarditis by sequencing the 16S rRNA gene from a prosthetic valve sample.
Current treatment guidelines recommend, in patients with viridans group streptococcal prosthetic valve endocarditis, six weeks of penicillin (24 million U/24h IV in continuous infusion or 4-6 doses) or ceftriaxone (2g/24h IV or IM), which can be combined with a 2-6 week regimen of gentamicin (3mg/kg every 24h IV or IM). In highly sensitive strains (MIC of penicillin ≤0.12mg/l), as in our case, the combination with gentamicin has not shown higher cure rates compared to monotherapy.10
This case adds more scientific evidence about the ability of S. cristatus to cause serious infections such as bacteraemia or endocarditis, although more studies are needed to explore its virulence.
FundingNo funding was received.
Conflicts of interestThe authors have no conflicts of interest to declare.
