




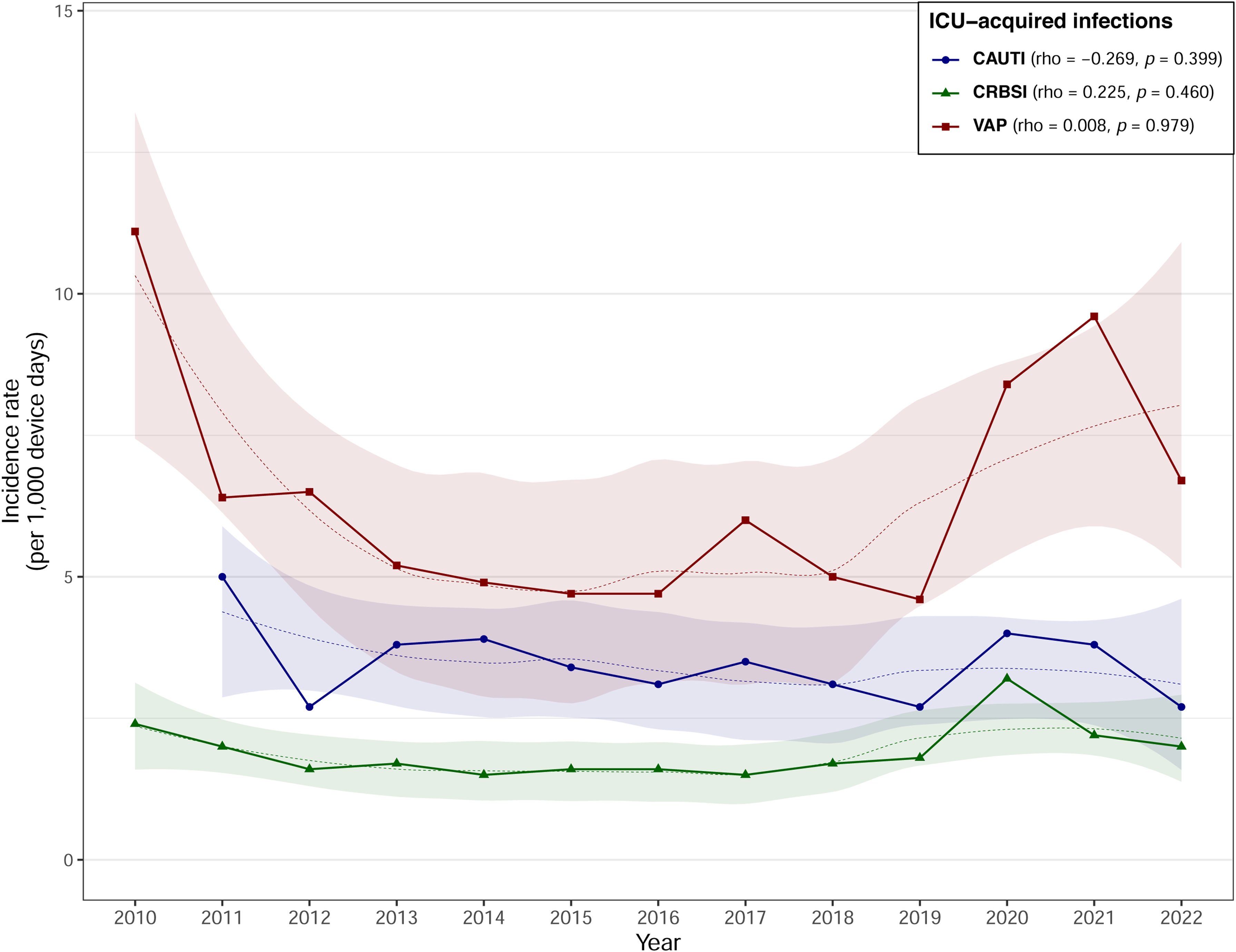
Surveillance is an essential part of the control of device-related nosocomial infections (NI) in intensive care units (UCIs). The aim of this study was to analyze the evolution of device-related infection rates in ICUs over the last 13 years, including ventilator-associated pneumonia (VAP), catheter-related bloodstream infection (CRBSI) and catheter-associated urinary tract infection (CAUTI).
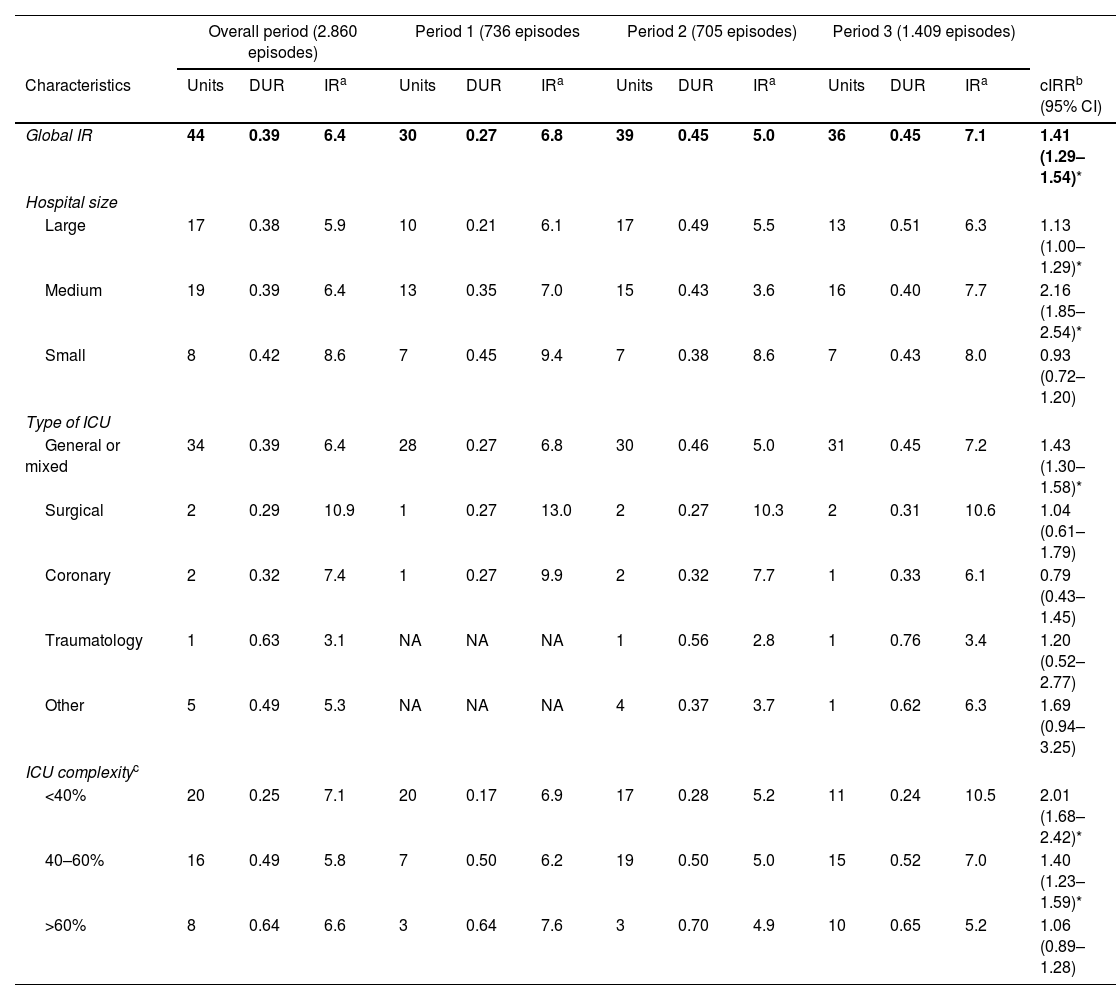
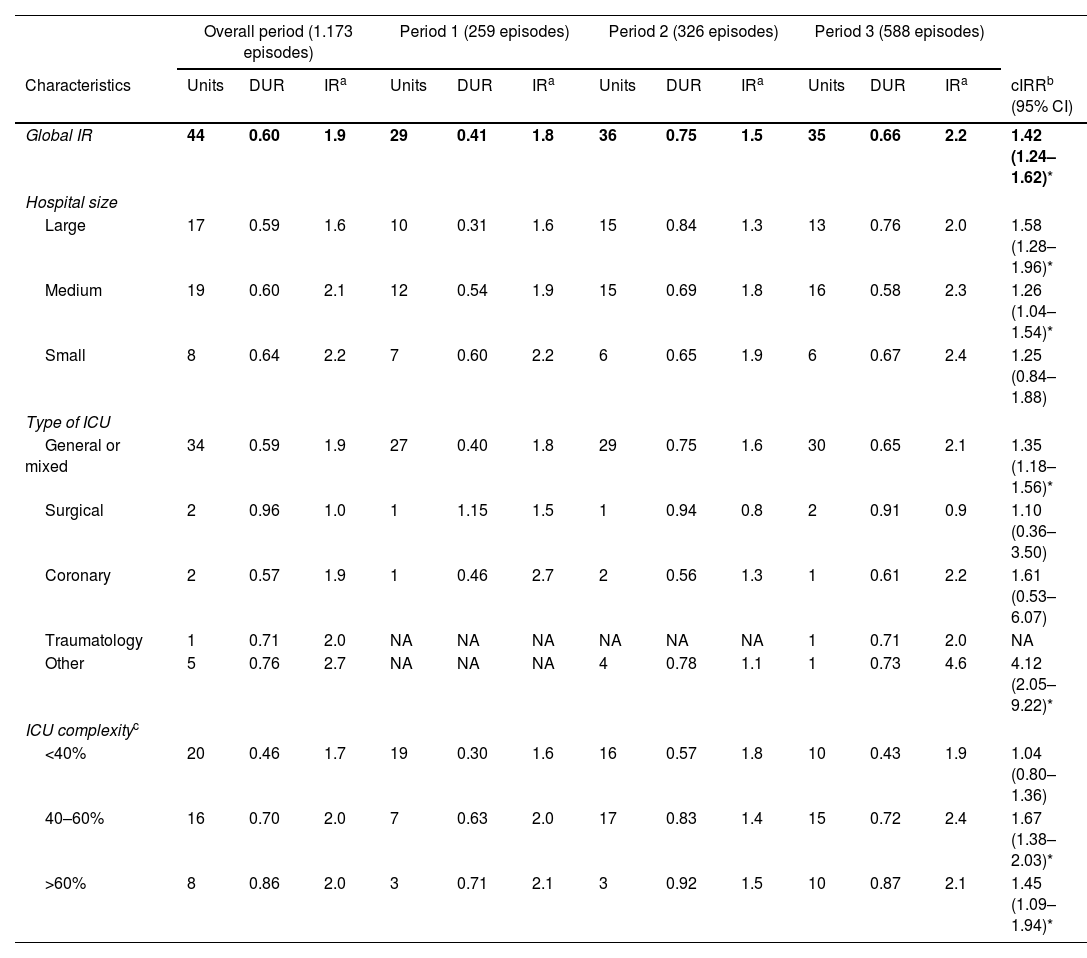
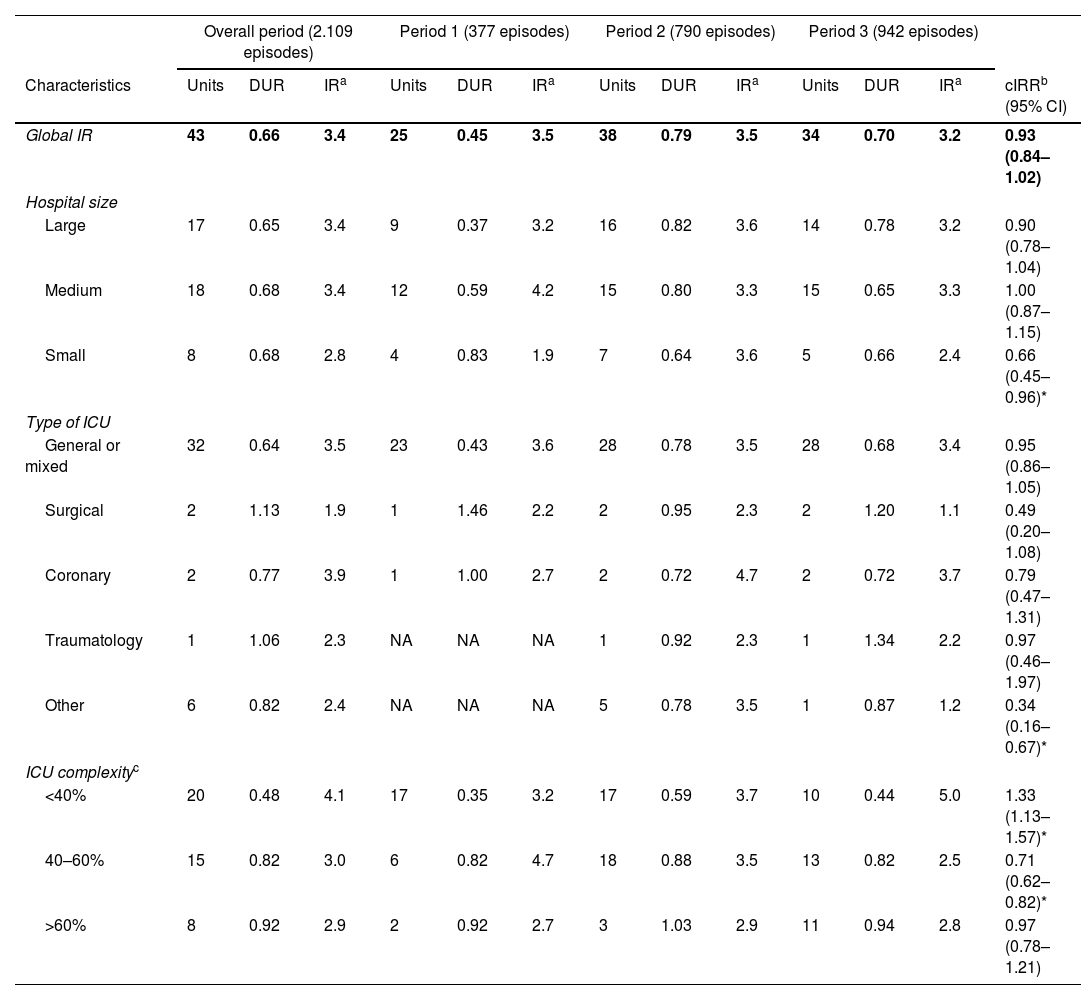
Material and methodsPatients admitted to the 44 ICUs at 43 participating hospitals of the VINCat Program from 2010 to 2022 were included, taking into account three periods: first period (2010–2013), second period (2014–2017) and third period (2018–2022). Hospitals were classified into three groups according to their size: small (<200 beds), medium (200–500 beds) and large (>500 beds). Complexity was assessed based on the use of invasive mechanical ventilation. The incidence rate of VAP, CRBSI and CAUTI was recorded at least during three consecutive months/year in each unit by an intensivist with extensive experience.
ResultsThe device utilization ratio (DUR) of mechanical ventilation was 0.39, varying between 0.38 in large hospitals and 0.42 in small hospitals. The DUR of central venous catheter was 0.6, ranging from 0.59 (large hospitals) to 0.64 (small). The DUR of urinary catheter was 0.66, with a range of 0.65 (large hospitals) to 0.68 (small). The complexity of the different ICUs influenced the DUR of the different devices and the infections associated with them. The average rates of VAP, CRBSI, and CAUTI were 6.4, 1.9, and 3.4 episodes per 1000 device days respectively.
ConclusionsSurveillance systems provide information on intra-ICU infections. ICU complexity, measured in terms of the use of mechanical ventilation, influences device-associated infections.
La vigilancia es una parte esencial para el control de las infecciones asociadas a dispositivos en los servicios de medicina intensiva. El objetivo de este estudio es establecer las tasas de neumonía asociada a ventilación mecánica (NAVM), bacteriemia asociada a catéter (BRC) e infección urinaria asociada a sonda vesical (ITUC) que ayuden a reducir las infecciones.
MétodosSe incluyeron pacientes ingresados en las 44 UCI (43 hospitales participantes) del Programa VINCat desde el año 2010 al año 2022. Los hospitales se clasificaron en 3 grupos: pequeños (<200 camas), medianos (200-500 camas) y grandes (>500 camas). La complejidad se evaluó según el uso de ventilación mecánica invasiva. Se registraron la densidad de incidencia de NAVM, BRC e ITUC, mínimo de 3 meses consecutivos/año en cada unidad.
ResultadosEl uso promedio (DUR) de ventilación mecánica fue de 0,39 (0,38-0,42 hospitales grandes y pequeños, respectivamente). El DUR de catéter venoso central fue de 0,6 (0,59-0,64 hospitales grandes y pequeños, respectivamente). El DUR de sonda vesical fue de 0,66 (0,65-0,68 hospitales grandes y pequeños, respectivamente). La complejidad de las UCI influyó en la ratio de uso de los diferentes dispositivos y en las infecciones asociadas a los diferentes dispositivos. El promedio de la densidad de incidencia de NAVM, BRC y la ITUC fueron de 6.4, 1,9, y 3,4 episodios por cada 1.000 días de dispositivo.
ConclusionesLos sistemas de vigilancia permiten obtener información de las infecciones intra-UCI. La complejidad de las UCI, medida como uso de ventilación mecánica influye en las infecciones asociadas a los dispositivos.
Artículo
Socio de la Sociedad Española de Enfermedades Infecciosas y Microbiología Clínica
![]()
Para acceder a la revista
Es necesario que lo haga desde la zona privada de la web de la SEIMC, clique aquí
Para realizar los cursos formativos
La actividad estará abierta para socios de la SEIMC. IMPORTANTE, recuerde que requiere registro previo gratuito. Empezar aquí
