




Electrocardiogram (ECG) is currently considered as an important diagnostic tool to monitor and evaluate patients with cardiovascular disease. This study aims to determine and analyze ECG recording patients with cardiovascular disease and analyze the specific characteristics of ECG for each cardiovascular diseases with and without complication.
MethodThis study applied descriptive study with 23 samples of outpatients with cardiovascular disease with and without complication selected using purposive sampling technique. Data collected was analyzed using descriptive analysis.
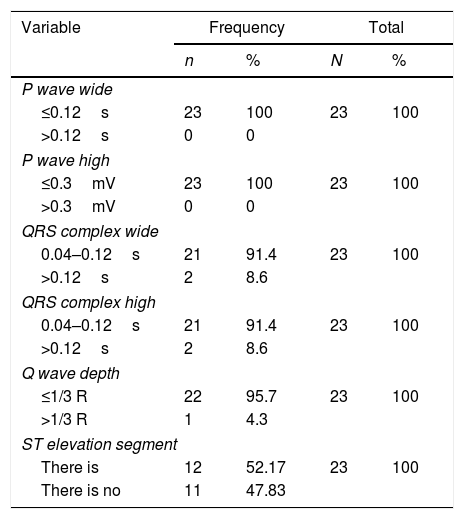
ResultsThis study results show that P wave is normal with a width of 0.12s (100%) and a height of <0.3mV (100%), the width of the QRS complex is between 0.04 and 0.12s (91.4%), PR interval width is 0.12–0.20s (100%), Q wave width is majority <0.04s and Q wave depth 1/3 R (95.7%). The ST segment on the lead II recorded that 52.17% of patients have ST Elevation and very little patient was identified with wide QRS complex and abnormal Q wave.
ConclusionMajority of patients experienced ischemia as shown by the average patients having myocardial ischemia. This could slow down the repolarization process. Some experienced ischemia as shown by the ST Elevation segment which could slow down the repolarization process. However, there were respondents who did not experience ischemia and were abnormal in ECG recording. This is likely to be influenced by several factors including proper handling at the first ischemia attack, age and patient adherence to treatment given that respondents are patients who always control to poly-outpatients.
The inability of the heart to carry out its function will cause damage both physical and physiologically. This can be caused by interference from other body systems or vice versa. This situation ultimately disrupts the function and adaptation of humans as a system. This damage triggers the emergence of various diseases in the cardiovascular system.1
In Indonesia, cardiovascular disease has also increased. This is evidenced by the data recorded by the Harapan Kita hospital, one of the national references. So that it can represent the incidence of cardiovascular disorders in Indonesia. In 2013 the highest number admitted to the Harapan Kita hospital was Acute Coronary Syndrome as many as 3186 people where data entered through the Emergency Unit. The details are as follows: Unstable Angina Pectoris was 1206 cases; Non ST Myocardial Infarction Elevation (NSTEMI) was 719 cases; ST Myocardial Infarction Elevation (STEMI) was 896 cases; and APS was 456 cases, followed by heart failure consisting of Congestive Heart Failure (CHF) as many as 662 cases. This also included later Acute Decompensation Heart Failure (ADHF) with 1932 cases.2
One of the important diagnostic tests to record the heart's electrical activity is the Electrocardiogram (ECG). The electrical activity of the heart in the body can be recorded through electrodes mounted on the surface of the body. Abnormalities in the electrical layout of the heart will cause abnormalities in ECG images. Therefore, researchers are interested in identifying the description of the P wave curve, QRS complex, PR interval and ST segment in patients with cardiovascular disorders.3
MethodThis study applied descriptive study with 23 samples of outpatients with cardiovascular disease with and without complication selected using purposive sampling technique. Data collected were analyzed using descriptive analysis. In this study ECG recording used 200×300 Fucuda Denshi type ECG machine.
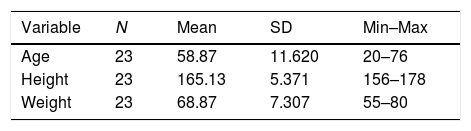
ResultsTable 1 shows that the average age of the respondents was 58.87 with a standard deviation of 11.620. The highest age was 76 years and the lowest age was 20 years. The average body height of respondents was 165.13cm with a standard deviation of 5.371 and the highest respondent was 178cm. The average weight of the respondent was 68.87kg with a standard deviation of 7.307 and the heaviest respondent was 80kg.
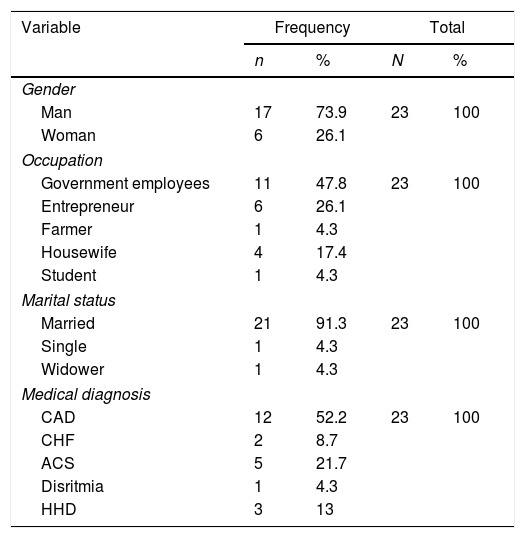
Table 2 shows the characteristics of respondents based on gender, occupation, marital status and medical diagnosis. In this study, 17 respondents were male (73.9%). In terms of occupation, the majority of the respondents were government Employees (11 respondents/47.8%). Based on marriage status, 21 respondents were married (91.3%). In terms of their medical diagnosis, 12 respondents (52.2%) were diagnosed with CAD (Coronary Artery Disease) and 5 respondents (21.7%) were diagnosed as with Acute Coronary Syndrome (Table 3).
Characteristics of respondents based on gender, occupation, marital status and medical diagnosis.
| Variable | Frequency | Total | ||
|---|---|---|---|---|
| n | % | N | % | |
| Gender | ||||
| Man | 17 | 73.9 | 23 | 100 |
| Woman | 6 | 26.1 | ||
| Occupation | ||||
| Government employees | 11 | 47.8 | 23 | 100 |
| Entrepreneur | 6 | 26.1 | ||
| Farmer | 1 | 4.3 | ||
| Housewife | 4 | 17.4 | ||
| Student | 1 | 4.3 | ||
| Marital status | ||||
| Married | 21 | 91.3 | 23 | 100 |
| Single | 1 | 4.3 | ||
| Widower | 1 | 4.3 | ||
| Medical diagnosis | ||||
| CAD | 12 | 52.2 | 23 | 100 |
| CHF | 2 | 8.7 | ||
| ACS | 5 | 21.7 | ||
| Disritmia | 1 | 4.3 | ||
| HHD | 3 | 13 | ||
Characteristics of respondents based on lead II electrocardiogram waves.
| Variable | Frequency | Total | ||
|---|---|---|---|---|
| n | % | N | % | |
| P wave wide | ||||
| ≤0.12s | 23 | 100 | 23 | 100 |
| >0.12s | 0 | 0 | ||
| P wave high | ||||
| ≤0.3mV | 23 | 100 | 23 | 100 |
| >0.3mV | 0 | 0 | ||
| QRS complex wide | ||||
| 0.04–0.12s | 21 | 91.4 | 23 | 100 |
| >0.12s | 2 | 8.6 | ||
| QRS complex high | ||||
| 0.04–0.12s | 21 | 91.4 | 23 | 100 |
| >0.12s | 2 | 8.6 | ||
| Q wave depth | ||||
| ≤1/3 R | 22 | 95.7 | 23 | 100 |
| >1/3 R | 1 | 4.3 | ||
| ST elevation segment | ||||
| There is | 12 | 52.17 | 23 | 100 |
| There is no | 11 | 47.83 | ||
The QRS complex in ECG recording showed that there were 21 respondents (91.4%) with a normal QRS complex width, and 2 respondents (8.6%) with an abnormal QRS complex. There were 22 respondents (95.7%) having the width and depth of normal Q waves, 1 respondent (4.3%) with the width and depth of the Q wave that was abnormal (pathological Q).
There were 12 respondents (52.17%) showing the ST segment elevation and 11 respondents (47.83%) did not show ST elevation segments.
DiscussionMyocardial ischemia will slow down the repolarization process, so that the ECG changes ST segments (depression) and T waves (inversions) depending on the severity of ischemia and the time to take the ECG. The specificity of ST segment changes in ischemia depends on the morphology. This study found 12 respondents who showed ST elevation, which means that some patients have suffered injury/ischemia in their heart muscle cells. However, when viewed from the results of the ECG recording, ST elevation has undergone an evolution, which means that there has been a decrease in oxygen supply to the heart muscle cell tissue for a long time. From the Q wave there was also one respondent who showed pathological Q which is also a characteristic feature of long-term infarction in patients with heart failure.
ConclusionIt can be concluded that the P wave on ECG recording of the respondents is in normal condition. Yet, if it is seen from the QRS sector, there was one abnormal respondent. Viewed from the Q wave there was one abnormal respondent. Most experienced ischemia as indicated by 12 respondents who experienced ST elevation. These are the findings of all the data in accordance with the diagnosis of respondents who are patients with cardiovascular disorders.
We would like to thank the Universitas Riau for funding this research by approving our research grant.
Our appreciation also goes to the Arifin Achmad Hospital where this study was conducted.
Peer-review of abstracts of the articles is under the responsibility of the Scientific Committee of Riau International Nursing Conference 2018. Full-text and the content of it is under responsibility of authors of the article.
