




This study aimed to explore sociodemographic characteristics and psychosocial wellbeing of elderly with chronic illnesses who live with family at home.
MethodsThis is a descriptive correlational study that was conducted in Pekanbaru. This study involved 85 elders that were recruited using purposive sampling technique. Data were obtained by using questionnaires.
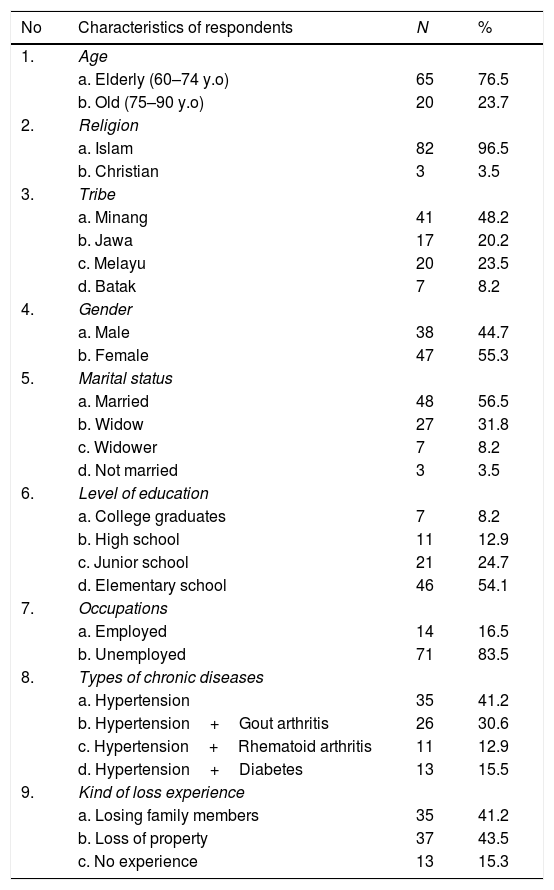
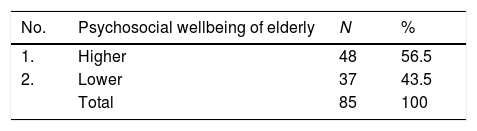
ResultsDescriptive analysis using a computer software showed that 96.5% of elderly were Muslim, 48.2% were from Minang tribe, 55.3% were female, 56.5% were married, 78.8% were low-educated, 83.5% were unemployed, and 84.7% had experience of losing a spouse, and showed that 56.5% of elderly have high psychosocial wellbeing state, which reflected psychological health and the ability to interact socially. Of all sociodemographic characteristics of the elders, all indicated higher psychosocial wellbeing state except for single elders or don’t have a life partner and unemployed elders. Chi-square test showed no significant relationship between educational level, marital status, employment status, and bereavement experience with psychosocial wellbeing of the elders (p>0.05).
ConclusionsThe majority of the elderly with chronic illnesses who live with family at home were at good psychosocial wellbeing. Measures are needed to improve psychosocial wellbeing of single elders or don’t have a life partner and unemployed elders.
Non-communicable chronic diseases are the main health problems that occur in the elderly in the world with a fairly high prevalence rate. More than 50% of the elderly population in the world experienced at least one type of chronic disease.1–3 This condition also occurs in Indonesia, including in Riau Province and Pekanbaru City.4–6
These chronic diseases are the main cause of disability in the elderly. This greatly affects the quality of life of the elderly and is even the main cause of death of the population in the world, especially if the disease is not controlled early.7–9 According to the authors,9–11 health conditions and the impact of chronic diseases experienced by the elderly become one of the risk factors for increased psychosocial health problems in the elderly, such as anxiety, feeling of worthlessness, depression, despair, social isolation and loneliness, alcoholism, fear of becoming a burden for family and society, even suicidal behavior. The prevalence of depression in elderly living in the community, in hospital and in nursing homes was 10–20%, 11–45%, and 50% respectively.8,10
This psychosocial condition is related to psychological and social demographic conditions, such as: level of education, loss of job, marital status, loss of spouse and loved ones, and social interaction of the elderly with the surrounding environment both inside and outside the house.8 Psychosocial conditions for the elderly, especially the elderly with chronic diseases, one of which is influenced by the existence of social support from the family. The family is the main support system for the elderly. According to the authors,8,9 every ethnic group, family in general is the first and foremost support system for the elderly. Mahler et al.17 explained that houses are the best place for the elderly to improve their health. Even various research results show that there is a relationship between family support for status, health condition, duration and severity of illness and death, psychological well-being, elderly healthy behavior, self-esteem and quality of life for the elderly.12,13
Based on this description, researchers were interested in conducting research on sociodemographic characteristics and psychosocial wellbeing of elderly people with chronic illness who live with family at home. This study aimed to explore sociodemographic characteristics and psychosocial wellbeing of elderly people with chronic illness who live with family at home.
MethodThis is a descriptive correlational study that was conducted in the working area of Payung Sekaki subdistrict Public Health Center in Pekanbaru. This subdistrict had the highest elderly population compared to other Public Health Centers. This study involved 85 elders who were recruited using purposive sampling technique according to the inclusion criteria, including: elderly aged 60 years and above, having at least 1 type of chronic disease, and live with family. The data was collected through questionnaires. The data collection tool used was closed statement questionnaires compiled based on literature studies. The questionnaires consisted of questions about respondents’ characteristics and social demographics including age, gender, religion, ethnicity, marital status, level of education, occupation, and experience of loss, and statements about elderly psychosocial well-being which reflected psychological condition or elderly self-concept and social interaction ability of elderly inside and outside the house. The total number of questions was 30 statements that have been tested for validity and reliability. Data analysis in this study was univariate and bivariate using computer software. Univariate analysis in the form of frequency distribution (%) and bivariate analysis using Chi Square test with p value (0.05).
Results1. Sociodemographic characteristics (Table 1).
Frequency distribution of sociodemographic characteristics of elderly.
| No | Characteristics of respondents | N | % |
|---|---|---|---|
| 1. | Age | ||
| a. Elderly (60–74 y.o) | 65 | 76.5 | |
| b. Old (75–90 y.o) | 20 | 23.7 | |
| 2. | Religion | ||
| a. Islam | 82 | 96.5 | |
| b. Christian | 3 | 3.5 | |
| 3. | Tribe | ||
| a. Minang | 41 | 48.2 | |
| b. Jawa | 17 | 20.2 | |
| c. Melayu | 20 | 23.5 | |
| d. Batak | 7 | 8.2 | |
| 4. | Gender | ||
| a. Male | 38 | 44.7 | |
| b. Female | 47 | 55.3 | |
| 5. | Marital status | ||
| a. Married | 48 | 56.5 | |
| b. Widow | 27 | 31.8 | |
| c. Widower | 7 | 8.2 | |
| d. Not married | 3 | 3.5 | |
| 6. | Level of education | ||
| a. College graduates | 7 | 8.2 | |
| b. High school | 11 | 12.9 | |
| c. Junior school | 21 | 24.7 | |
| d. Elementary school | 46 | 54.1 | |
| 7. | Occupations | ||
| a. Employed | 14 | 16.5 | |
| b. Unemployed | 71 | 83.5 | |
| 8. | Types of chronic diseases | ||
| a. Hypertension | 35 | 41.2 | |
| b. Hypertension+Gout arthritis | 26 | 30.6 | |
| c. Hypertension+Rhematoid arthritis | 11 | 12.9 | |
| d. Hypertension+Diabetes | 13 | 15.5 | |
| 9. | Kind of loss experience | ||
| a. Losing family members | 35 | 41.2 | |
| b. Loss of property | 37 | 43.5 | |
| c. No experience | 13 | 15.3 |
2. Description of psychosocial wellbeing of elderly with chronic illnesses who live with family at home (Table 2).
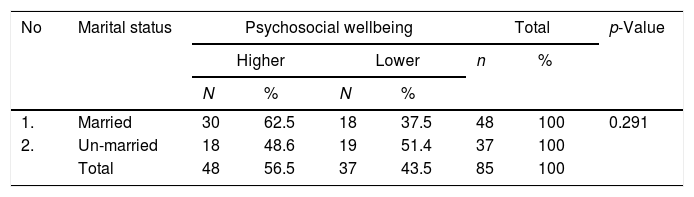
3. Marital status and psychosocial wellbeing of elderly.
Table 3 shows that there was no relationship between marital status with elderly psychosocial well-being of chronic diseases living with family (p value: 0.291).
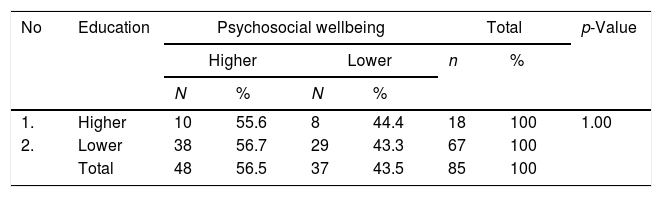
4. Level education of elderly and psychosocial wellbeing of elderly.
Table 4 shows that there was no relationship between the level of education with psychosocial wellbeing of elderly (p value: 1.00).
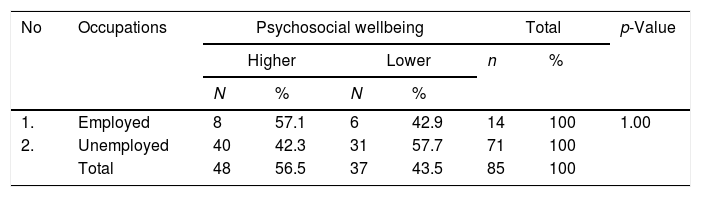
5. Employment status and psychosocial wellbeing of elderly (Table 5).
Table 6 shows there was no relationship between employment status and elderly psychosocial wellbeing (p value: 1.00).
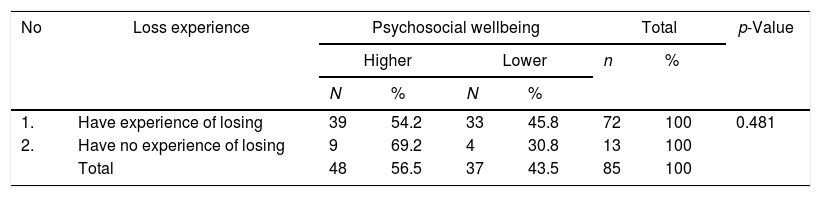
6. Loss experience and psychosocial wellbeing of elderly.
Table 6 shows there was no correlation between loss experience with elderly psychosocial wellbeing (p value: 0.481)
DiscussionHealth conditions and the impact of chronic diseases experienced by the elderly become one of the risk factors for an increase in psychosocial health problems in the elderly, such as anxiety, feelings of worthlessness, depression, despair, social isolation and loneliness, alcoholism, fear of being a burden on family and society, even suicidal behavior.9 These psychosocial conditions are related to psychological and social demographic conditions such as level of education, marital status, loss of job, loss of spouse and loved ones.8
The results showed that all the social demographic characteristics did not have a relationship with elderly psychosocial wellbeing with p value >0.05. This was due to the elderly live with the family he loved despite having chronic illnesses. The family is the main support system for the elderly, especially for the elderly with chronic diseases. According to 14–16, the family is a natural social support system and as the main support system for all its members, especially for the elderly who experience chronic diseases.
Family as the closest person and is the most important source of support in elderly life. According to 8,9, every ethnic group, family in general is the first and foremost support system for the elderly. Mahler et al.17 explained that houses are the best place for the elderly to improve their health. The results showed that there was a relationship between family support for status, health condition, duration and severity of illness and death, psychological well-being, elderly healthy behavior, self-esteem and quality of life for the elderly.12,13
ConclusionsThe majority of the elderly with chronic illnesses who live with family at home were at good psychosocial wellbeing. Of all sociodemographic characteristics of the elders, all indicated higher psychosocial wellbeing state except for single elders or do not have a life partner and unemployed elders. Chi-square test showed no significant relationship between educational level, marital status, employment status, and bereavement experience with psychosocial wellbeing of the elders (p>0.05). Measures are needed to improve psychosocial wellbeing of single elders or do not have a life partner and unemployed elders.
Researchers highly appreciate the School of Nursing for providing grant for this research, Pekanbaru Local Health Department, and the Head of Payung Sekaki Public Health Center.
Peer-review of abstracts of the articles is under the responsibility of the Scientific Committee of Riau International Nursing Conference 2018. Full-text and the content of it is under responsibility of authors of the article.
