




To determine the effectiveness of music therapy on anxiety and pain in critical polytraumatised patients admitted to the resuscitation unit of a tertiary level hospital in Spain.
Material and methodRandomised clinical trial conducted in a tertiary level hospital, from June 2016 to May 2018. The study sample was 60 patients, 30 belonging to the intervention group (IG), and 30 to the control group (CG). The IG were given a 30-minute music session and heart rate (HR) and blood pressure (BP) were measured. The VAS (Visual Analogue Scale) was applied for anxiety and pain before and after each session. The same measures and scales were applied in the CG who did not receive a music session. The music session comprised 3 parts: the first was standard music selected by music therapists; the second was personalised, chosen by the patient and the third was a new standard. The intervention took place in a booth with headphones.
ResultsSignificant changes in anxiety levels (P<.01) were detected in the group of patients undergoing the intervention, measured with the VAS scale for anxiety, and pain levels (P<.01), measured with the VAS scale for pain. No significant differences were found in the physiological parameters of HR and BP.
ConclusionThe use of music in critical polytraumatised patients reduces anxiety and pain levels, increasing the patient's well-being and improving the quality of care. Music therapy, therefore, is considered beneficial as a complementary measure in critical care units. It would be worthwhile to continue studies in this and other hospital areas.
Determinar la efectividad de la musicoterapia sobre la ansiedad y el dolor en pacientes críticos politraumatizados ingresados en la unidad de reanimación de un hospital de tercer nivel en España.
Material y métodoEnsayo clínico aleatorizado realizado en un hospital de tercer nivel, desde junio de 2016 a mayo de 2018. La muestra del estudio fue de 60 pacientes, 30 pertenecientes al grupo intervención y 30 al grupo control. El grupo intervención recibió una sesión musical de 30 minutos y se midieron los parámetros de frecuencia cardiaca y presión arterial. Se aplicaron las escalas visuales analógicas (EVA) desarrolladas para la ansiedad y para el dolor antes y después de cada sesión. Al grupo control se le aplicaron las mismas medidas y escalas sin recibir sesión musical. La sesión musical estaba compuesta de 3 partes: primera parte de música estándar, seleccionada por musicoterapeutas; segunda parte personalizada, elegida por el paciente, y tercera parte de nuevo estándar. La aplicación de la intervención se realizó en el box mediante auriculares.
ResultadosSe detectaron cambios significativos en el grupo de pacientes que recibieron la intervención, tanto en los niveles de ansiedad (p<0,01), medidos con la escala EVA para la ansiedad, como en los niveles de dolor (p<0,01), medidos con la escala EVA para el dolor. No se encontraron diferencias significativas en los parámetros fisiológicos de frecuencia cardiaca y presión arterial.
ConclusiónEl uso de la música en pacientes críticos politraumatizados reduce los niveles de ansiedad y dolor, aumentando el bienestar del paciente y mejorando la calidad en sus cuidados. Por ello se considera beneficiosa la musicoterapia como medida complementaria en las unidades de cuidados críticos, y sería conveniente la continuidad de los estudios en esta y otras áreas de hospitalización.
What is known?
The effect of music therapy has been assessed in recent years as a therapeutic intervention in both hospital and out-of-hospital settings, examining its effectiveness in different fields, oncological care, paediatric care, mental health, post-surgical care, etc.
What does this paper contribute?
The results of this study provide scientific evidence on the use of music therapy in the critical patient. The study confirms with data the beneficial effect of the intervention and provides new bases for future research on the use of live music and personalised music.
Implications of the study
Nurses can use music as a complementary measure to reduce anxiety and pain in the critical polytraumatised patient, using it as daily practice in the personalised care of the critical patient.
Benenzon1 defined music therapy as “a psychotherapy that uses sound, music and body-sound-musical instruments to establish a relationship between music therapist and patient or group of patients, through it to improve the quality of life and enable recovery and rehabilitation of the patient into society”.
We can communicate through music in a more subtle way than by words alone, and effects can be produced at very different levels, so we can set different objectives and carry out a holistic intervention on the person, encompassing physiological, emotional, cognitive, social, and spiritual dimensions.2
Music therapy has been classified under Nursing Interventions Classification3 4400, since its first edition published in 1992, which describes it as: “the use of music to help achieve a specific change in patient’s behaviour, feelings or physiology”. Determining the specific behavioural and/or physiological change desired, determining the patient’s interest in music, identifying the patient’s musical preferences, and facilitating the patient's active participation if desired and feasible within the situation are included as nursing activities.3,4
As an example, in her book, Notes on Nursing, Florence Nightingale relates how she used music as part of the care she provided to soldiers in the Crimean War to alleviate pain.5 The effect of music therapy as a therapeutic intervention has been assessed in different hospital settings not only for its effectiveness on anxiety, but also on many other variables such as postoperative pain, length of stay, satisfaction with care, oncological care, paediatric care, mental health care, etc.6,7
JustificationThere are fewer studies in intensive care units (ICU) that assess the effectiveness of music therapy in this type of patient. Perpiñá-Galvan and Richart-Martinez8 published a review analysing the different scales and levels of anxiety perceived by patients admitted to ICU. In this review, 24% to 80% of ICU patients had moderate to severe levels of anxiety.
The study by Lin et al.,9 on postoperative spinal surgery patients, aimed to determine the effects of music therapy on the levels of anxiety, pain and psychological reactions to physical and emotional stress suffered by these patients, and found statistically significant differences. Following a quasi-experimental design, in which the intervention group listened to music the night before and after surgery, and the control group did not listen to music, the patients' anxiety and pain levels were measured with visual analogical scales (VAS), including heart rate (HR) and blood pressure (BP) among other physiological measures. There were statistically significant differences between the 2 groups in VAS scores for both anxiety (p=.018–.001) and pain (p=.001). BP measured one hour after surgery was significantly lower in the study group than in the control group (p=.014). Similarly, the study by Chang and Chen10 that looked at the effects of music therapy on anxiety and satisfaction levels in women undergoing scheduled caesarean sections found a lower degree of anxiety and higher degree of satisfaction associated with the experience in the women included in the intervention group.
However, in the study by Comeaux and Steele-Moses,11 also in postoperative patients, music therapy decreased pain and improved perception of ambient noise, but showed no effect on the patients’ state of anxiety.
A review of the recent literature was undertaken in a published article by Lázaro,12 which included numerous studies on the use of music in patients. Studies on critically ill patients in different clinical situations were included, for example, during mechanical ventilation, non-invasive mechanical ventilation and to facilitate nocturnal rest. Papers on postoperative, coronary and asthma patients were also included.
This same article12 refers to a 2014 Cochrane review on the evidence in adult patients on mechanical ventilation, its main objective being to update a first review carried out in 2010, in which anxiety, respiratory rate, HR, BP, arterial saturation and mortality were analysed. Other objectives of this review were to examine the effects of music therapy and music intervention compared to routine treatment, to compare the effects of music chosen or not chosen by the patient and to compare the effects of music therapy and music intervention. The authors concluded that music may have beneficial effects in reducing anxiety in ventilated ICU patients with reduced respiratory rate and systolic blood pressure (SBP). Moreover, it is a measure that is easy to implement, and therefore they recommend offering music as a stress reduction measure in critical patients.
In a recently published article by Golino et al.,13 the use of active music therapy as a non-pharmacological intervention in intensive care units was considered beneficial. They also laid some foundations for future research on music therapy in intensive care units.
In light of all the above, we considered it relevant to conduct a clinical trial to show the effects of music therapy in critical polytraumatised patients, given the scarcity of studies that use music therapy in this type of patient.
ObjectivesPrimary objective: to measure and compare the VAS scores for pain and for anxiety in polytraumatised critical patients with and without the use of music therapy.
Secondary objective: to measure and compare the haemodynamic parameters of HR and BP in critical polytraumatised patients with and without the use of music therapy.
Primary hypothesisHypothesis: polytraumatised patients admitted to the resuscitation unit of a tertiary hospital who receive music therapy show a decrease in anxiety and pain levels compared to those who do not receive music therapy.
MethodType of study: randomised clinical trial.
Setting: resuscitation unit of a tertiary hospital in Spain. This is a 12-bed unit with patients with different diseases, most are postoperative and polytraumatised.
Participants: critical polytraumatised patients. “Polytraumatised” is defined as any patient with multiple organic and/or musculoskeletal injuries with impaired circulation and/or ventilation that are life-threatening immediately or within hours.14
Inclusion criteria: critical polytraumatised patients without sedation, without invasive mechanical ventilation, with a score higher than or equal to 11 on the Glasgow scale15 and with signed informed consent.
Exclusion criteria: patients under 18 years of age, patients with hearing problems, non-Spanish speaking patients, professional musicians (as studies indicate that musicians process music differently to non-musicians16,17) and cognitively impaired patients.
Sample sizeThe sample size was estimated based on the literature reviews analysed. Sanjuán Naváis et al.16 published a prospective experimental study with randomised distribution in which they examined the effects of music on anxiety and pain in patients with invasive mechanical ventilation. According to the data obtained from that article on the effect at the end of the intervention (mean difference 7.32, giving a standardised mean difference of .88%, which is a high effect size), for a confidence level of 95% and power of 80%, 75 patients would be needed in each group. If we look at the effect 1hour later (mean difference 6.39, giving a standardised mean difference of .86), for a 95% confidence level and power of 80%, 73 patients would be needed in each group. Five percent of the total sample needed to cover possible losses was added, giving a final sample size of 80 patients for each group.
After piloting, with a total of 25 patients, the sample size was reduced to 60 patients (30 patients in the control group and 30 patients in the intervention group) for various reasons explained later in the discussion.
RandomisationPatients who met the inclusion criteria were randomised into 2 groups: an intervention group and a control group. A programme to generate the sequence of random numbers, Random Sequence Generator, available at: https//www.random.org/sequences/ was used for the randomisation into groups. This randomisation was carried out by a person outside the research team when the patient signed the consent form.
- -
Intervention group: use of music therapy through headphones.
- -
Control group: no music therapy.
Participants were recruited in the resuscitation unit of a tertiary hospital, after meeting the inclusion criteria for the intervention.
If they met the inclusion criteria, the patient was informed about the study and was given an informed consent form. Once the informed consent form was signed, the patients were randomised and informed whether they belonged to the control or intervention group. The music session was given according to musical tastes (collected in the music therapy form) and the standard session carried out specifically to reduce levels of anxiety and pain as recommended by music therapists, which were measured through the VAS.
The intervention group received a 30-minute music session, where the clinical parameters of HR, BP and pain and anxiety levels on the VAS scale were measured before and after each session. The control group underwent the same measurements and scales without receiving the music session.
The intervention took place in their booth with headphones.
- -
Intervention group: the researcher gave the music session through headphones for 30minutes. Music sessions with demonstrated efficacy in previous studies18–21 were used: 10minutes of classical music (Rodrigo's Concierto de Aranjuez, Vivaldi's Four Seasons, the Linz Symphony, Mozart's K425), 10minutes of personalised music and 10minutes of relaxing music (Liberation’s door Snatam Kaur, Tibetan singing bowls). The music ranged from 60-80r.p.m. and headphones were used throughout the session.21
- -
Control group: did not receive music therapy.
In both cases, the clinical parameters of HR and BP were measured and pain and anxiety levels using the VAS (with a range from 0 to 100,22 where a score of 0 means no pain or anxiety reported and 100mm is the maximum pain and anxiety) before and after each session. At 15min, without intervening in the session, HR and BP parameters were recorded to assess changes in these clinical parameters brought about by the personalised music. These data were recorded on a form created by the research team.
The control group underwent the same measurements and scales without receiving the music session. The intervention was always delivered in the patient’s own booth.
Description of the study variablesDependent variables: anxiety (measured by the VAS) and pain (measured by the VAS), physiological parameters (BP and HR, measured through patient monitoring).
Independent variables: receiving or not receiving music therapy, age, sex, rural or urban setting, musical taste, and interest in music (not much, quite a lot, a lot).
Ethical aspectsPrior to starting the project, the study was approved by the ethics and clinical research committee of a tertiary hospital in Spain (Act 4/2016).
All patients included in the study were informed about the process through the letter of introduction and informed consent. In addition, they were asked to participate voluntarily and sign the corresponding informed consent form in accordance with the Basic Law on Patient Autonomy, 41/2002, of 14 November, in compliance with the ethical principles concerning biomedical research of Law 14/2007, of 3 July. The data were treated confidentially, in compliance with the Organic Law on Personal Data Protection, 15/1999.
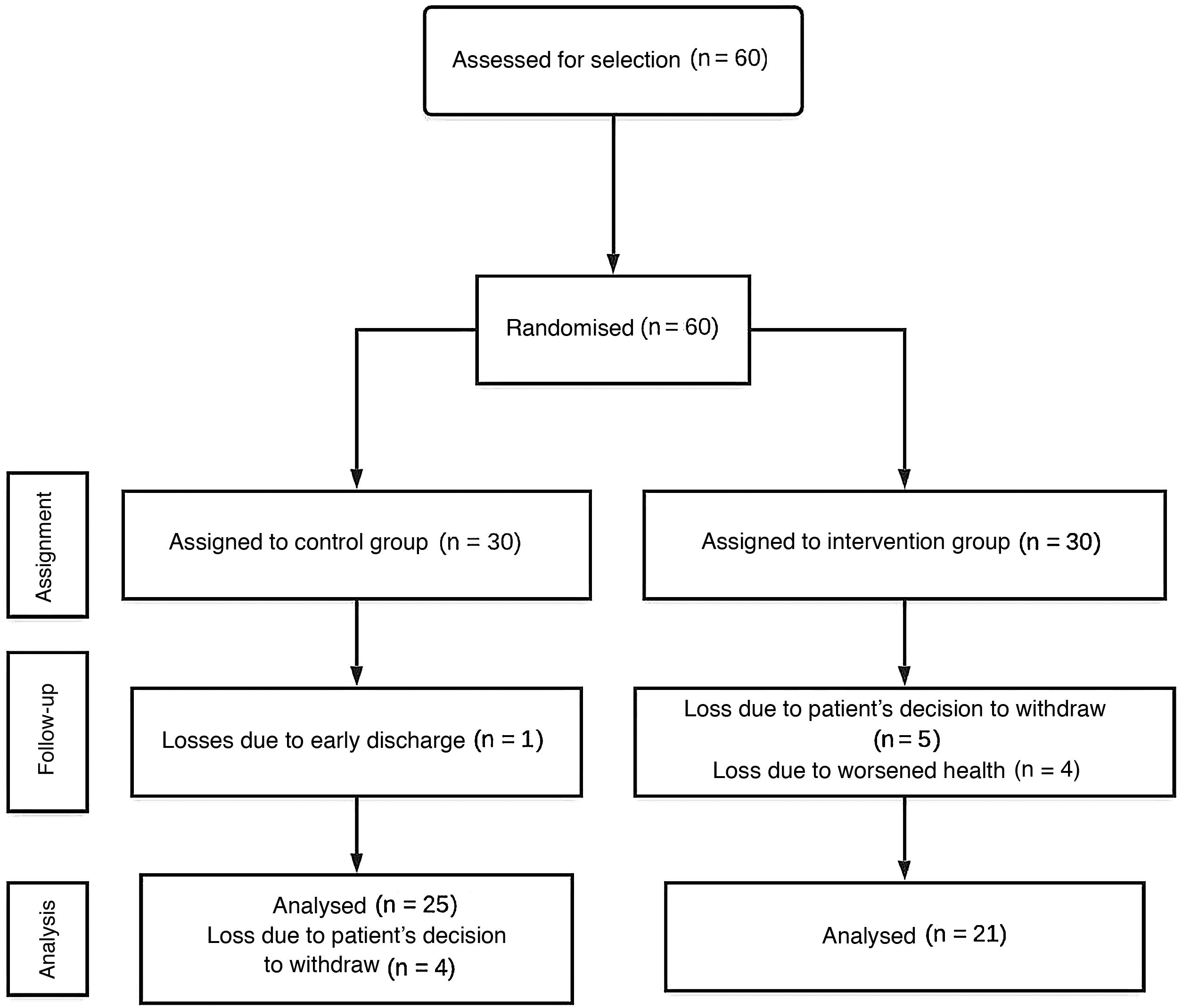
ResultsSixty patients were included in this study, 30 patients in the intervention group and 30 patients in the control group.
Of the individuals assigned to the intervention group, 5 patients withdrew their consent (at the beginning of the session) and 4 patients abandoned the study due to worsening of their state of health (the session could not be carried out), 21 patients were eventually studied.
Of the patients assigned to the control group, one patient was lost due to early discharge and 4 patients withdrew their consent (before the end of the session), 25 patients were eventually studied, as shown in Fig. 1.

In short, of the 60 participants 46 patients completed the study.
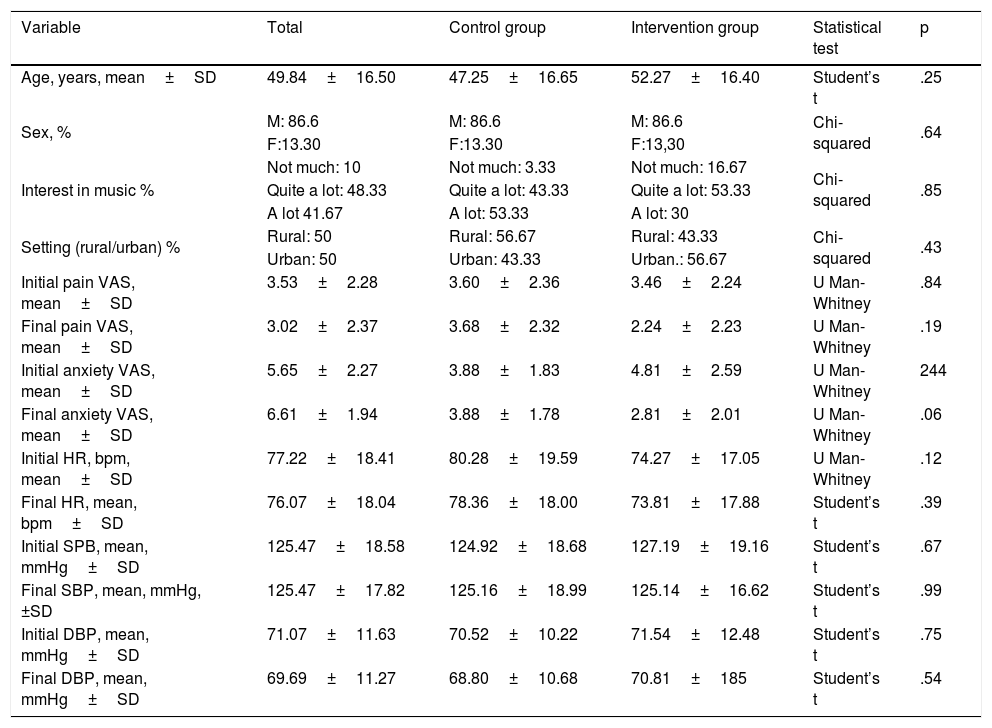
SPSS 24.0 for Windows was used for the data analysis. It was analysed on an intention-to-treat basis, including a 95% confidence interval in the measurement of the results. Table 1 shows frequencies and percentages for qualitative variables and for quantitative variables, mean and standard deviation. The level of statistical significance between the two groups is analysed using the Student’s t-test.
Homogeneity of the groups.
| Variable | Total | Control group | Intervention group | Statistical test | p |
|---|---|---|---|---|---|
| Age, years, mean±SD | 49.84±16.50 | 47.25±16.65 | 52.27±16.40 | Student’s t | .25 |
| Sex, % | M: 86.6 | M: 86.6 | M: 86.6 | Chi-squared | .64 |
| F:13.30 | F:13.30 | F:13,30 | |||
| Interest in music % | Not much: 10 | Not much: 3.33 | Not much: 16.67 | Chi-squared | .85 |
| Quite a lot: 48.33 | Quite a lot: 43.33 | Quite a lot: 53.33 | |||
| A lot 41.67 | A lot: 53.33 | A lot: 30 | |||
| Setting (rural/urban) % | Rural: 50 | Rural: 56.67 | Rural: 43.33 | Chi-squared | .43 |
| Urban: 50 | Urban: 43.33 | Urban.: 56.67 | |||
| Initial pain VAS, mean±SD | 3.53±2.28 | 3.60±2.36 | 3.46±2.24 | U Man-Whitney | .84 |
| Final pain VAS, mean±SD | 3.02±2.37 | 3.68±2.32 | 2.24±2.23 | U Man-Whitney | .19 |
| Initial anxiety VAS, mean±SD | 5.65±2.27 | 3.88±1.83 | 4.81±2.59 | U Man-Whitney | 244 |
| Final anxiety VAS, mean±SD | 6.61±1.94 | 3.88±1.78 | 2.81±2.01 | U Man-Whitney | .06 |
| Initial HR, bpm, mean±SD | 77.22±18.41 | 80.28±19.59 | 74.27±17.05 | U Man-Whitney | .12 |
| Final HR, mean, bpm±SD | 76.07±18.04 | 78.36±18.00 | 73.81±17.88 | Student’s t | .39 |
| Initial SPB, mean, mmHg±SD | 125.47±18.58 | 124.92±18.68 | 127.19±19.16 | Student’s t | .67 |
| Final SBP, mean, mmHg,±SD | 125.47±17.82 | 125.16±18.99 | 125.14±16.62 | Student’s t | .99 |
| Initial DBP, mean, mmHg±SD | 71.07±11.63 | 70.52±10.22 | 71.54±12.48 | Student’s t | .75 |
| Final DBP, mean, mmHg±SD | 69.69±11.27 | 68.80±10.68 | 70.81±185 | Student’s t | .54 |
bpm: beats per minute; DBP: diastolic blood pressure; HR: heart rate; mmHg: millimetres of mercury; SBP: systolic blood pressure; SD: standard deviation; VAS: visual analogue scale.
For the sociodemographic variables (age, sex, rural or urban setting and musical tastes), homogeneity was calculated using the Chi-squared test or other parametric or non-parametric tests depending on the type of variable. For the variables pain, anxiety and initial HR, homogeneity was calculated using the Mann-Whitney U test because the sample was not normal. On the other hand, age, SBP, diastolic blood pressure (DBP), HR during and at the end were analysed using the Student's t-test as they showed a normal distribution. The level of statistical significance was set at p<.05.
When the homogeneity of the groups had been checked, the next step was a paired mean comparison of the initial and final values of the variables described above, dividing them between the control and intervention groups.
The sex and age variables were compared; most participants were male, with a mean age of 49 years.
In terms of the rural or urban setting variable, there were no differences in either group (intervention or control); it was similar in both.
Regarding the musical tastes of the participants in both groups (rock-pop, classical, flamenco and folk, jazz, new age, or soundtracks), the most frequent type of music was pop-rock, and it varied according to the age of the subject, the older the subject, the greater the preference for folk music.
With respect to the interest in music variable (a lot, a little or none), the intervention group contained the subjects with the least musical interest compared to the control group.
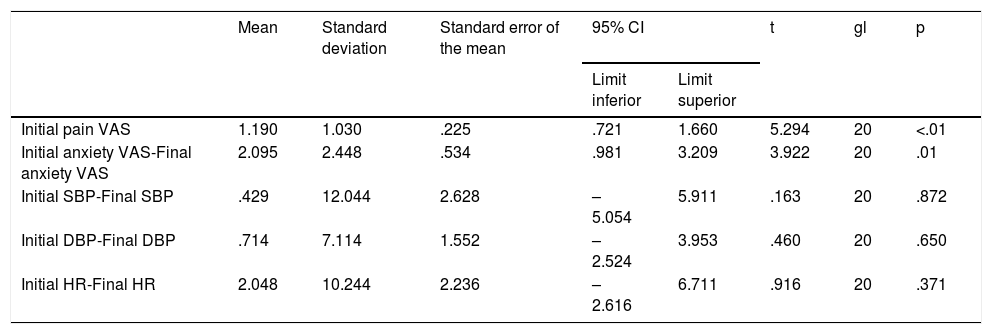
A session was held for each patient, whether they were included in the intervention or control group. In the measurements of the different variables, significant differences were found in the intervention group in relation to initial pain VAS and final pain VAS (p<.001) and initial anxiety VAS and final anxiety VAS (p=.01), as shown in Table 2. No significant differences were found in initial and final SBP (p=.872), initial and final DBP (p=.650) or initial and final HR (p=.371).
Paired sample test of the intervention group.
| Mean | Standard deviation | Standard error of the mean | 95% CI | t | gl | p | ||
|---|---|---|---|---|---|---|---|---|
| Limit inferior | Limit superior | |||||||
| Initial pain VAS | 1.190 | 1.030 | .225 | .721 | 1.660 | 5.294 | 20 | <.01 |
| Initial anxiety VAS-Final anxiety VAS | 2.095 | 2.448 | .534 | .981 | 3.209 | 3.922 | 20 | .01 |
| Initial SBP-Final SBP | .429 | 12.044 | 2.628 | –5.054 | 5.911 | .163 | 20 | .872 |
| Initial DBP-Final DBP | .714 | 7.114 | 1.552 | –2.524 | 3.953 | .460 | 20 | .650 |
| Initial HR-Final HR | 2.048 | 10.244 | 2.236 | –2.616 | 6.711 | .916 | 20 | .371 |
DBP: diastolic blood pressure; HR: heart rate; SBP: systolic blood pressure; VAS: visual analogue scale.
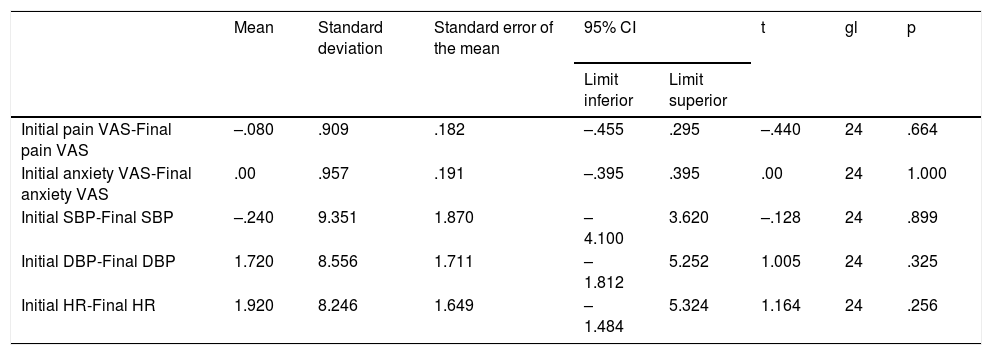
Table 3 shows that there were no statistically significant differences in the control group in initial and final VAS pain (p=.664) or initial and final VAS anxiety (p=1.000) or in the physiological parameters of SBP (p=.899), DBP (p=.325) or initial HR and final HR (p=.256).
Paired sample test of the control group.
| Mean | Standard deviation | Standard error of the mean | 95% CI | t | gl | p | ||
|---|---|---|---|---|---|---|---|---|
| Limit inferior | Limit superior | |||||||
| Initial pain VAS-Final pain VAS | –.080 | .909 | .182 | –.455 | .295 | –.440 | 24 | .664 |
| Initial anxiety VAS-Final anxiety VAS | .00 | .957 | .191 | –.395 | .395 | .00 | 24 | 1.000 |
| Initial SBP-Final SBP | –.240 | 9.351 | 1.870 | –4.100 | 3.620 | –.128 | 24 | .899 |
| Initial DBP-Final DBP | 1.720 | 8.556 | 1.711 | –1.812 | 5.252 | 1.005 | 24 | .325 |
| Initial HR-Final HR | 1.920 | 8.246 | 1.649 | –1.484 | 5.324 | 1.164 | 24 | .256 |
DBP: diastolic blood pressure; HR: heart rate; SBP: systolic blood pressure; VAS: visual analogue scale.
Music therapy can be used in the healthcare setting as a non-pharmacological tool, at both the psychological and the physiological level. The purpose of the study was to investigate the effects of music therapy in critical polytraumatised patients with a score greater than or equal to 11 on the Glasgow scale. Our results successfully confirmed the main hypothesis that music therapy reduces anxiety and pain in a single session. Different studies support our results in this regard,9,10,23,24 showing significant differences between the control and intervention groups. Despite there being scientific evidence in this respect,9,15 regarding the secondary objective, when the control and intervention groups were compared in terms of physiological parameters, there were no changes in BP or HR.
In contrast to the article by Sanjuán et al.,16 the results obtained regarding pain showed a reduction in final pain in the group receiving the music session. It is also striking that even though the intervention group showed less interest in music, their levels of anxiety and pain improved significantly.
It is likely that an increase in the number of music therapy sessions received by the patient would improve medical and/or psychological outcomes, as shown in the study by Golino et al..13 In the unit where our study took place, the type of patient selected for the clinical trial tended to have a short mean stay, either due to improvement, discharge to another hospital unit, transfer to another hospital or worsening of their state of health. Therefore, it was difficult to deliver several music sessions to the same patient.
After confirming, according to the results, that the musical intervention (pre-recorded session) reduced anxiety and pain, we believe that the effect of music therapy on physiological parameters should be studied through sessions given by music therapists with live music.25
Regarding the musical tastes’ variable, and irrespective of the musical style chosen, no differences were found between the choice of one type of music or another (rock-pop, classical, flamenco and folklore, jazz, new age, or soundtracks). After the study experience (as the participants expressed their opinion on it), the ideal would be to conduct future research to assess the effect of music therapy by comparing its effectiveness through sessions with classical and relaxing music exclusively versus sessions with personalised music chosen by the patient.
Finally, and thanks to the different studies consulted, we can confirm that music therapy can provide a safe, economical experience with an important emotional and historical impact on patients, as shown in the literature reviewed.26
Limitations of the studyThe number of participants was limited in establishing the inclusion criteria, and therefore in future studies this clinical trial could be extended to other types of patients in the critical care unit. After piloting, the study sample size was cut due to losses for the following reasons:
- •
In polytraumatised patients with traumatic brain injury, it is common to find oscillating Glasgow scale values, which results in a loss of study subjects due to worsening of their condition.
- •
On the other hand, when the patient was informed about the characteristics of the study and given the consent form for the study with their family present, in several cases they gave consent out of courtesy, and the session was not carried out because consent was later withdrawn.
This reduction in the number of participants led to a loss of statistical power of the data analysed, and we could not obtain positive results in the analysis of the physiological parameters.
Furthermore, music therapy was not used in the control group using headphones. Headphones were not used in the control group because this would be an intervention in itself, as they would isolate background noise. And the researcher delivering the session was the person who collected the data, and there was no double-blinding.
ConclusionThis clinical trial demonstrated that using music therapy it is possible to reduce anxiety and pain, thus improving the length of stay of patients admitted to critical care units. Furthermore, although physiological parameters were not affected using a single session during the study, thanks to its low cost and easy application, it would be advisable to use this tool as a non-pharmacological measure in these units, as part of the nursing care plan, to promote patient wellbeing and improve the quality of patient care.
The study aims to extrapolate its results to other intensive care units so that they can incorporate music therapy as a nursing intervention, and thus be able to offer a complementary action to sedoanalgesia in relation to pain and anxiety.
Means required- •
Two music players and headphones were used to deliver the therapy correctly.
- •
Unit monitors for non-invasive heart rate and blood pressure measurement (already present in each booth of the resuscitation unit of the Albacete General Hospital).
The authors have no conflict of interests to declare.
We would like to thank all the patients and relatives who participated in the study, the Nursing Management of the Complejo Hospitalario Universitario of Albacete, and in particular María Dolores Pardo, Juan David Fernández and Pilar Córcoles for their availability and help in providing the means to carry out the study, colleagues in the resuscitation department for their collaboration and above all our music therapists, María García and Juan Damián Villanueva, for their selfless help.
Please cite this article as: Contreras-Molina M, Rueda-Núñez A, Pérez-Collado ML, García-Maestro A. Efecto de la musicoterapia sobre la ansiedad y el dolor en el paciente crítico politraumatizado. Enferm Intensiva. 2021;32:79–87.

